


There are many known relationships between diet and health outcomes(Reference Mozaffarian1). An unbalanced diet may cause nutrient deficiencies and excessive energy intake which can increase the risk of becoming overweight or obese. Being overweight or obese is a risk factor for various diseases such as diabetes mellitus type 2 or CVD. In addition, being overweight or obese in childhood is very likely to be continued into adulthood(Reference Ebbeling, Pawlak and Ludwig2). Taste preferences and dietary habits developed during childhood may also last for a lifetime(Reference Ellrott and Kersting3,Reference Kelder, Perry and Klepp4) . Associations between social disparities and health behaviour among adolescents have been observed; a lower socio-economic status (SES) is associated with less participation in sports, poorer diets and higher prevalence rates for being overweight and obese(Reference Drewnowski5–Reference Singh, Siahpush and Kogan7). International and national research focusing on dietary behaviour shows that there is lower consumption of fruit(Reference Borrmann and Mensink8,Reference Fismen, Smith and Torsheim9) and vegetables(Reference Borrmann and Mensink8–Reference Niven, Scully and Morley10) among adolescents with a low SES compared with adolescents with a high SES. Among adolescents with a low SES, the consumption of sugar-sweetened beverages(Reference Borrmann and Mensink8,Reference Hanson and Chen11–Reference Holstein, Damsgaard and Due13) and fast food(Reference Niven, Scully and Morley10,Reference Moosburger, Lage Barbosa and Haftenberger14) is higher than that of their counterparts with a high SES.
Food consumption habits are changing continuously due to changes in the food supply and other reasons that include an extension of the range of products as well as changes in living conditions. For example, the all-day school system in Germany has been expanded in the last years. Therefore, school meals have an increasing influence on food consumption among children and adolescents(Reference Klemm and Zorn15). In former East Germany, all-day schools were more common than in former West Germany; therefore, the utilisation of school meals among children and adolescents was also more common(Reference Klemm and Zorn15). Therefore, it is still interesting to compare food consumption in former East and West Germany almost 30 years after the reunification.
National representative dietary surveys provide relevant information on food consumption of the general population and specific groups. Such information, including deficits in food consumption in specific population groups, is needed to identify relevant fields of action for public health interventions. This is relevant for decision-makers in the field of public health nutrition. The ‘German Health Interview and Examination Survey for Children and Adolescents’ (KiGGS) is part of the national health monitoring system of the Robert Koch Institute(Reference Kurth, Kamtsiuris and Holling16). Within the KiGGS baseline survey (2003–2006), a study with in-depth focus on nutrition, the ‘Eating Study as a KiGGS Module’ (EsKiMo), was conducted in 2006(Reference Mensink, Bauch and Vohmann17). About a decade later, EsKiMo II (2015–2017) was conducted as part of KiGGS Wave 2. This newly available information about food consumption of children and adolescents living in Germany may help to identify deficits and excesses in food consumption and risk groups(Reference Lage Barbosa, Brettschneider and Haftenberger18,Reference Brettschneider, Lage Barbosa and Haftenberger19) . The aim of this analysis is to describe the food consumption among 12- to 17-year-old adolescents in general and to stratify it by SES as well as by the region of residence and to evaluate their food consumption in relation to German food-based dietary guidelines according to the concept of the Optimized Mixed Diet (OMD)(Reference Kersting, Kalhoff and Lücke20).
Methods
Study design
EsKiMo II was implemented within the second wave of KiGGS – KiGGS Wave 2 and conducted between 2015 and 2017 with the aim of providing representative data on food consumption and nutritional status among children and adolescents living in Germany. For EsKiMo II, an age- and sex-stratified sample of 2644 children and adolescents aged 6–17 years was drawn from the study sample of the cross-sectional part from KiGGS Wave 2. Since different instruments were used to assess food consumption depending on participants’ age(Reference Lage Barbosa, Brettschneider and Haftenberger18,Reference Brettschneider, Lage Barbosa and Haftenberger19) , the present analysis is restricted to 1353 adolescents aged from 12 to 17 years.
Dietary assessment
Participants aged from 12 to 17 years were interviewed about their food consumption during the past 4 weeks using the software DISHES (Dietary Interview Software for Health Examination Studies) which is based on a modified dietary history method developed by the Robert Koch Institute(Reference Mensink, Bauch and Vohmann17,Reference Mensink, Haftenberger and Thamm21) . The interviews were conducted face-to-face by trained nutritionists during home visits. Following a daily meal structure (breakfast, mid-morning snack, lunch, mid-afternoon snack, dinner, small late meal and snacks throughout the day), the consumption frequencies and portion sizes of all foods consumed were recorded. Tableware models and a picture book of portion sizes(Reference Ocké, de Boer and Brants22,Reference Van Kappel, Amoyel and Slimani23) were used to assist in the estimation of portions. A validation study among adults showed that differences in macronutrient intake between DISHES and 3-d dietary records and 24-h recalls were within an acceptable range for assessing food consumption in epidemiological studies(Reference Mensink, Haftenberger and Thamm21). Estimation of food consumption using DISHES showed fairly good agreement with a FFQ among children(Reference Truthmann, Mensink and Richter24). For the selection of food items, the German Nutrient Data Base (Bundeslebensmittelschlüssel, Max Rubner Institute) Version 3.02 was integrated in the DISHES software.
Food group quantities
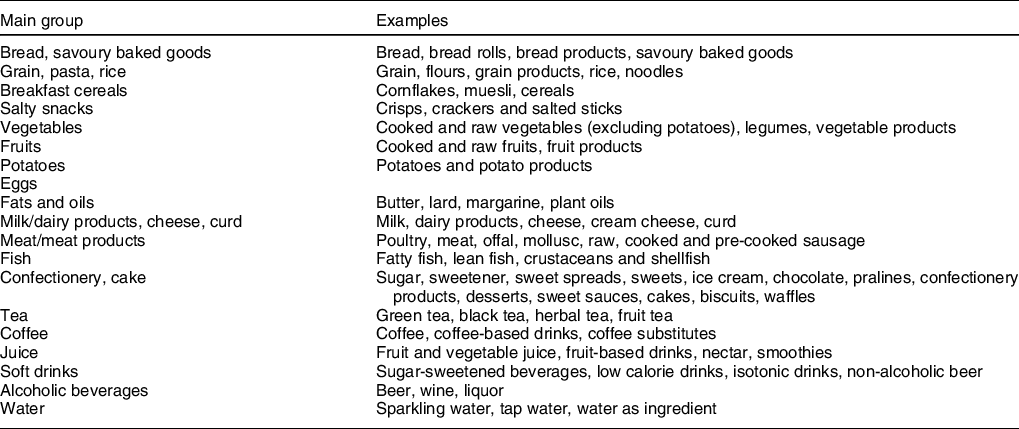
Quantities were calculated on the basis of the amount of foods as they were consumed (e.g. cooked, fried, raw). Composed dishes, which could not be unequivocally assigned to one food group, were decomposed into their ingredients, and these were assigned to the corresponding food group. The mean daily amount of each food consumed was obtained by multiplying the consumption frequency by the portion amount and dividing this by 28 (4 weeks ≙ 28 d). The daily amounts consumed were summarised in food groups. For solid foods, fourteen different groups (bread, savoury baked goods; grain, pasta, rice; breakfast cereals; salty snacks; vegetables; fruits; potatoes; eggs; fats and oils; milk/dairy products, cheese, curd; meat/meat products; fish; confectionery, cake; other food items) and for beverages, six groups (tea; coffee; juice; soft drinks; alcoholic beverages; water) were constructed. Table 1 gives an overview of the food groups.
Table 1 Description of the analysed food groups
Food-based dietary guidelines for children and adolescents in Germany
The food consumption in EsKiMo II was compared with the OMD recommendations of 2017(Reference Kersting, Kalhoff and Lücke20). Within the concept of OMD, the German nutrient recommendations (D-A-CH reference values) were translated into sex- and age-specific food-based dietary guidelines for children and adolescents(Reference Kersting, Kalhoff and Lücke20). The recommended age-specific amounts were derived for eleven food groups, considering an energy requirement for a low level of physical activity (PAL 1.4)(Reference Kersting, Kalhoff and Lücke20). The foods reported in EsKiMo II were summarised into the eleven OMD food groups. These can generally be categorised in three recommended consumption amount groups:
-
foods to be consumed plenty – ‘beverages’, ‘vegetables’, ‘fruits’, ‘bread/(breakfast) cereals’, ‘potatoes/pasta/rice’;
-
foods to be consumed moderately – ‘milk/dairy products’, ‘meat/meat products’, ‘eggs’, ‘fish’;
-
foods to be consumed sparingly - ‘oil/margarine/butter’, ‘unfavourable foods’ (sweets, pastries, sugar-sweetened beverages).
In order to evaluate food group consumption according to the concept of the OMD, for each individual, we divided the particular food group consumption by the corresponding age- and sex-specific recommendations and multiplied this by 100. The distribution characteristics of these proportion values are presented. For the present analysis, the food groups ‘bread/(breakfast) cereals’ and ‘potatoes/pasta/rice’ were summarised as ‘starchy foods’ (referring to foods with high content of complex carbohydrates). For comparison with the OMD, sugar-containing beverages were included in the food group beverages. In addition, the energies obtained from sugar-containing beverages were included in the group ‘unfavourable foods’. Age- and sex-specific OMD-recommended quantities for adolescents aged 12–17 years are shown in Table 2.
Table 2 Recommendations for food consumption quantities according to the food-based dietary guidelines(Reference Kersting, Kalhoff and Lücke20)

* Milk equivalents, i.e. 100 g milk corresponds to 100 g yogurt or 30 g cheese.
† 100 kcal corresponds to about 20 g chocolate or 30 g jam or 45 g fruit cake or 10 chips or 200 ml lemonade.
Socio-economic status and region of residence
In KiGGS Wave 2, comprehensive information from participants and their parents was collected. A multidimensional SES index was derived from information provided by the parents about their level of education, occupational status and net income. Therefore, point scores were assigned according to the level of each status dimension ranging from 1 to a maximum of 7, and the sum of these scores was calculated. The three equally weighted subscales of education, occupational status and income provide the basis for calculating the SES index, which means that SES index values ranged between 3·0 and 21·0. This SES index was divided into quintiles and classified into (1) low SES (lowest quintile), (2) medium SES (middle three quintiles) and (3) high SES (upper quintile)(Reference Lampert, Hoebel and Kuntz25). Information about the region of residence was classified into (1) former West Germany and (2) former East Germany (including Berlin).
Statistical analyses
Mean, median, 5th and 95th percentiles for food and beverage consumption in g/d were described separately for girls and boys. Distributions of individual consumption in proportion to the OMD-recommended amounts are presented using Box–Whisker plots with the inner box corresponding to the interquartile range around the median and the whiskers corresponding to the 5th and 95th percentiles.
Mean values with 95 % CI for absolute amounts of food consumption in g/d as well as the proportion of adolescents who achieved the OMD-recommended amounts (%) were calculated in total and for categories of SES and region of residence. Differences in mean food group consumption by SES and region were tested using ANOVA. Differences in the proportion of adolescents who achieved the OMD-recommended amounts by SES and region were tested with the χ 2 test.
To correct for deviations from the German population with regard to age (in years), sex, federal state (as of 31 December 2015), nationality (as of 31 December 2014) and parents’ level of education (Microcensus 2013), as well as for differences in participation in EsKiMo II by parental SES, school type visited by the child and season, a weighting factor was applied in EsKiMo II. To take the cluster design of the study sample into account, the analyses were conducted using the survey procedures of SAS version 9.4 (SAS Institute Inc.). All analyses were stratified by sex.
Results
The present analysis included 727 girls and 626 boys. Twenty-three percent of the girls and 16 % of the boys lived in families with a low SES and 14 % of the girls and 21 % of the boys in families with a high SES. One-sixth of the adolescents were from former Eastern Germany (Table 3).
Table 3 Basic characteristics of the study population of Eating Study as a KiGGS Module (EsKiMo) II (n 1353)

Generally, mean and median food group consumption was higher among boys than girls (Table 4). The mean consumption of beverages among girls amounted to approximately 1700 ml/d, whereas the mean consumption among boys was more than 2000 ml/d. The main beverage was water which contributed to two-thirds of the total beverage consumption of girls and boys. Meanwhile, the contribution of soft drinks, juices and alcoholic beverages to total beverage consumption was about one quarter among girls and one-third among boys. Median consumption of meat/meat products among girls was 74 g/d, whereas among boys, it was 114 g/d. Only the consumption of vegetables, fruits and tea was higher among girls than boys. Median consumption for fruits was 121 g/d and for vegetables 167 g/d among girls and 98 g/d and 142 g/d, respectively, among boys.
Table 4 Mean and distribution characteristics of total energy (kcal/d) and food consumption (g/d) among adolescents aged from 12 to 17 years from Eating Study as a KiGGS Module (EsKiMo) II, stratified by sex (n 1353)*
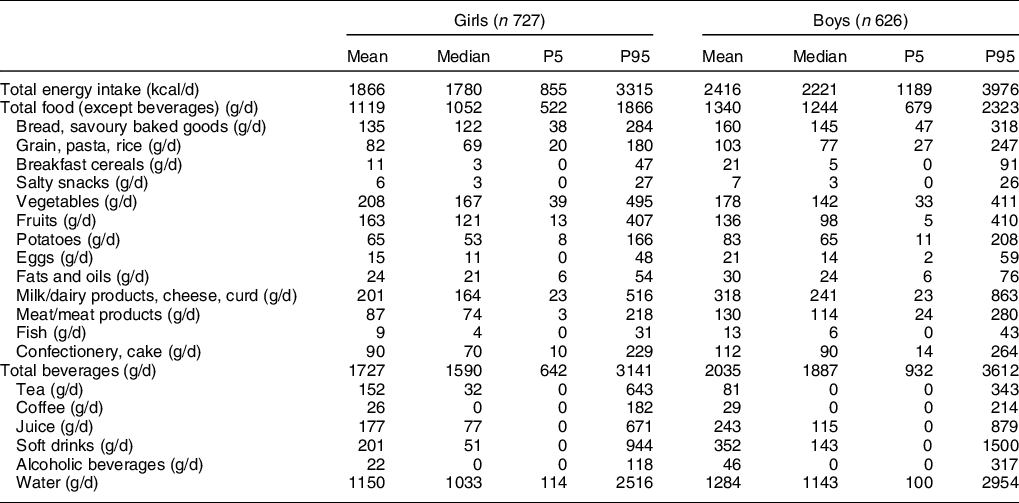
P5, 5th percentile; P95, 95th percentile.
* Weighted figures except n (= unweighted sample number).
Figure 1 shows the distribution (using Box–Whisker plots) of food group consumption among girls and boys expressed as proportions of the OMD-recommended amounts. The total amount of beverages consumed by most of the adolescents was above the minimum amount recommended. The median consumption of fruits, vegetables, starchy foods, milk/dairy products, eggs, fish and oil/margarine/butter of adolescents was below the recommended amounts. This indicates that more than half of the adolescents did not achieve the recommendations for these food groups. For meat/meat products and unfavourable foods, the median consumption was far above the recommended amounts. More than half of the boys had a consumption of unfavourable foods twice as high as the recommended amounts (Fig. 1).

Fig. 1 Distribution of food consumption expressed as the proportion of the recommended amounts for an OMD among 12- to 17-year-old (a) girls and (b) boys in EsKiMo II (n 1353) (Box–Whisker plots*) * Box–Whisker plots with the inner box corresponding to the interquartile range around the median and the whiskers corresponding to the 5th and 95th percentiles
A comparison of the mean consumption of food groups by the SES of the family is presented in Table 5. Girls with a low SES consumed on average more meat/meat products than girls with a high SES (103 g/d v. 67 g/d; P < 0·01). The mean consumption of soft drinks was five times higher among girls with a low SES than those with a high SES (314 g/d v. 62 g/d; P < 0·001). Among boys, it was three times higher for those with a low SES compared with their counterparts with a high SES (587 g/d v. 188 g/d; P < 0·001). Meanwhile, boys with a high SES had a higher juice consumption than boys with a low SES (155 g/d v. 254 g/d; P < 0·05).
Table 5 Mean and 95 % CI of food consumption (g/d) among adolescents from Eating Study as a KiGGS Module (EsKiMo) II by sex and socio-economic status (SES) (n 1334)*

* Weighted figures except n (= unweighted sample number), number of adolescents with missing SES: n 19.
† Significant differences between groups were tested using ANOVA.
For most food groups, there were no statistical differences among SES groups regarding the proportion achieving the OMD-recommended amounts (Table 6). However, the proportion of boys who achieved the recommended amounts of fruit differed significantly by SES. Boys with a low SES met the recommended amount of fruit more often compared with boys with a medium or high SES (P < 0·05).
Table 6 Proportion of adolescents from Eating Study as a KiGGS Module (EsKiMo) II achieving the Optimized Mixed Diet (OMD)-recommended amount by sex and socio-economic status (SES) (n 1334)*
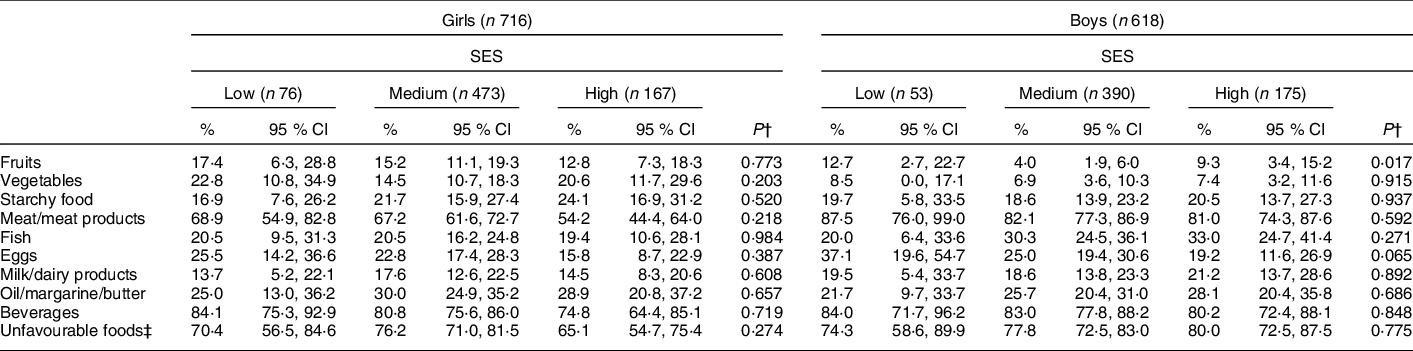
* Weighted figures except n (= unweighted sample number), number of adolescents with missing SES: n 19.
† Significant differences between groups were tested using the χ 2 test.
‡ Sweets, pastries, sugar-sweetened beverages.
Table 7 shows the mean consumption of foods by region of residence. Among girls from former West Germany, the mean consumption of total beverages was significantly higher than among girls from former East Germany (1768 ml v. 1517 ml; P < 0·01). Considering the specific beverages, we observed that compared with girls from former East Germany, girls from former West Germany had a higher mean consumption of water (1215 ml v. 814 ml; P < 0·001) but a lower mean consumption of tea (133 ml v. 247 ml; P < 0·05). In addition, girls from former West Germany had a higher mean consumption of grain, pasta, rice (85 g v. 68 g; P < 0·001), vegetables (214 g v. 179 g; P < 0·01) and meat/meat products (90 g v. 74 g; P < 0·01) and a lower consumption of breakfast cereals (11 g v. 16 g; P < 0·01) than girls from former East Germany. Among boys from former West Germany, the consumption of oils and fat was lower compared with counterparts from former East Germany (37 g v. 29 g; P < 0·01).
Table 7 Mean consumption and 95 % CI of foods (g/d) among adolescents from Eating Study as a KiGGS Module (EsKiMo) II by sex and region of residence (n 1353)*

* Weighted figures except n (= unweighted sample number).
† Significant differences between groups were tested using ANOVA.
There were differences in food consumption regarding the proportion of adolescents achieving or exceeding the recommended amounts of the OMD according to the region of residence. Girls from former West Germany achieved the recommended amount for vegetables significantly more often than girls from former East Germany (vegetables: 18·6% v. 10·4%; P < 0·05). The recommended amount for total beverages was met significantly more often by girls from former West Germany (81·9 %) compared with girls from former East Germany (71·7 %; P < 0·05). The recommended amounts for oil/margarine/butter were achieved more often among boys from former East Germany (38·8 %) than among boys from former West Germany (23·8 %; P < 0·01) (Table 8).
Table 8 Proportion of adolescents from Eating Study as a KiGGS Module (EsKiMo) II achieving the Optimized Mixed Diet (OMD)-recommended amount by sex and region of residence (n 1353)*

* Weighted figures except n (= unweighted sample number).
† Significant differences between groups were tested using the χ 2 test.
‡ Sweets, pastries, sugar-sweetened beverages.
Discussion
While the majority of adolescents in Germany consumed sufficient amounts of beverages, they did not achieve the recommended amounts of the OMD for most food groups. In particular, the consumption of fruits, vegetables, starchy foods and milk/dairy products of most adolescents aged 12–17 years in Germany was below the recommended amounts. The consumption of meat/meat products and unfavourable foods like sweets, pastries and sugar-sweetened beverages, which should be consumed sparingly, exceeded the recommended amounts. Though the total beverage consumption of the majority of adolescents was above the minimum amount recommended, a large part was reached through juices and soft drinks. Differences in food group consumption were also observed according to SES and region of residence; adolescents with a low SES had a higher soft drink consumption than those with a high SES. Girls from former West Germany more often achieved the recommended amount of vegetables compared with girls from former East Germany.
Our results are largely in line with results from the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study of a sample of European adolescents aged from 12 to 17 years(Reference Diethelm, Jankovic and Moreno26). For most food groups, the deviations from the recommended amounts of the OMD observed in HELENA are in a similar range and the same direction as the ones observed in EsKiMo II. There seems to be a clear discrepancy between HELENA and EsKiMo II only for total beverage consumption, with a higher proportion of adolescents achieving the recommended amount for beverages in EsKiMo II compared with HELENA. This can be explained by differences in food group classification between both studies. In HELENA, only water, tea and coffee were assigned to the food group beverages, whereas in EsKiMo II, fruit and vegetable juices as well as soft and alcoholic drinks were also included.
Both the HELENA Study(Reference Diethelm, Jankovic and Moreno26) and EsKiMo II observed that the consumption of fruit and vegetables of adolescents was clearly below the recommended amount of the OMD. In other European countries, children and adolescents also did not reach the recommendation for fruit and vegetable consumption(Reference Diethelm, Jankovic and Moreno26,Reference Lynch, Kristjansdottir and Te Velde27) . The WHO recommends a daily consumption of 400 g of fruit and vegetables for adolescents(28), which is lower than the recommended amount of the OMD. However, the mean consumption of 371 g/d among girls is almost in accordance with the WHO recommendation. According to the ranking of the Health Behaviour in School-aged Children (HBSC) study for daily fruit consumption in Europe, the fruit consumption among adolescents living in Germany is at midrange, whereas countries like Greenland and Finland are at the bottom and Armenia and Albania are at the top of this ranking(Reference Inchley, Currie and Young29). An improvement of fruit and vegetable consumption could be achieved by consuming one additional portion of fruit and one additional portion of vegetables daily.
In EsKiMo II, only about 20 % of the adolescents reached the recommended amount for starchy foods. Shortcomings in the consumption of starchy foods of adolescents were also observed previously(Reference Diethelm, Jankovic and Moreno26).
Low consumptions of milk and dairy products by adolescents have been published previously(Reference Diethelm, Jankovic and Moreno26). The observation that even <25 % of the adolescents achieved the recommended amount for milk/dairy products indicates a need for action, especially because preliminary analysis of the nutrient intakes from EsKiMo II showed that Ca intake of the majority of adolescents is below the German nutrient recommendations (D-A-CH reference values) (unpublished results). Since milk and dairy products are an important Ca source(30), a major cause of the deficits in Ca intake among adolescents may be the low consumption of milk and dairy products.
The median consumption of meat/meat products of adolescents in EsKiMo II was lower, as observed among adolescents in the HELENA Study(Reference Diethelm, Jankovic and Moreno26), but far above the recommended amount. A reduction of meat consumption is highly recommended. Current social developments and public discussions about vegetarianism, bio-industry, animal welfare, climate impact of meat consumption and feeding the increasing world population may lead to a reduction of meat consumption in the near future(Reference Sanchez-Sabate and Sabaté31).
The recommended amount of unfavourable food was also largely exceeded. An excessive consumption of energy-dense, nutrient-poor food is also seen in other European studies among adolescents(Reference Diethelm, Jankovic and Moreno26,Reference Vandevijvere, De Vriese and Huybrechts32) . As this food group mainly consists of foods with a high energy density and a low nutritive value, a reduction in the consumption of these foods or rather a shift of consumption from unfavourable to more favourable food groups like fruits, vegetables and unsweetened beverages is urgently needed.
Next to a comparison of the results from EsKiMo II and in the view of actual literature on food consumption of adolescents, a comparison with the results from EsKiMo I (2006)(Reference Mensink, Heseker and Richter33) is possible. This comparison indicates some changes in food consumption between 2006 and 2015–2017; the proportion of adolescents who achieved the recommended amounts of fruits, vegetables and milk/dairy products decreased over time. However, the proportion of adolescents who achieved the recommended amount of starchy foods has increased. The proportion of the recommended amount achieved for beverages, unfavourable foods and fish was similar in EsKiMo I and EsKiMo II. However, it should be considered that the recommended amounts of the OMD for the food groups fruits, vegetables, milk/dairy products and starchy foods have been changed between 2006 and 2015(Reference Kersting, Kalhoff and Lücke20). Additional analysis evaluating the food group consumption within EsKiMo I according to the actual OMD recommendations also shows a decrease in the proportion of adolescents achieving the recommended amount for fruits and milk/dairy products between both EsKiMo studies, and also the proportion of adolescents achieving the recommended amount of starchy foods decreased when using recalculated data for EsKiMo I (data not shown).
In both EsKiMo I(Reference Mensink, Heseker and Richter33) and EsKiMo II, sex differences in food consumption and in adherence to the food-based dietary guidelines have been observed. In both studies, absolute food consumption was higher among boys, conforming to the mainly higher requirements for boys than for girls. However, compared with girls, a lower proportion of boys achieved the recommended amounts of fruit and vegetables. Furthermore, boys showed a higher consumption of soft drinks. Generally, a poorer dietary quality among boys has already been reported in several studies conducted among adolescents and young adults in Belgium, New Zealand and the USA(Reference Vandevijvere, De Vriese and Huybrechts32,Reference Conner, Thompson and Knight34,Reference Olson, Hummer and Harris35) . Reasons for the differences between boys and girls might be differences in preferences, amongst others. Girls have a higher affinity for fruits and vegetables and perceive a lower barrier to their consumption(Reference Brug, Tak and te Velde36). Sex differences in fruit and vegetable consumption were also seen among adults living in Germany(Reference Heuer, Krems and Moon37,Reference Mensink, Truthmann and Rabenberg38) .
The results of EsKiMo II indicate a poorer dietary quality for adolescents with a low SES. The strongest social gradient is seen for soft drinks; boys and girls with a low SES have a significant higher consumption of soft drinks than adolescents with a high SES. This is in line with previous studies among adolescents, for example, the KiGGS Wave 1 and HBSC studies conducted in Germany and European Countries, respectively(Reference Hanson and Chen11,Reference Mensink, Schienkiewitz and Rabenberg12,Reference Vereecken, Inchley and Subramanian39) . Girls with a low SES have a significantly higher consumption of meat/meat products compared with girls with a high SES. A similar association between meat consumption and SES has already been reported for other populations(Reference Chan and Zlatevska40). However, the association between SES and the consumption of fruit(Reference Borrmann and Mensink8,Reference Fismen, Smith and Torsheim9) and vegetables(Reference Borrmann and Mensink8–Reference Niven, Scully and Morley10) observed in previous studies, also among adults(Reference Heuer, Krems and Moon37,Reference Mensink, Truthmann and Rabenberg38) , is not seen in EsKiMo II. This may be due to projects focused on the improvement of fruit and vegetable consumption, such as the EU school fruit and vegetable schemes that reach adolescents from all social backgrounds or projects focusing on socially disadvantaged adolescents conducted in the last decade(41).
To our knowledge, this is the first investigation of food consumption including a comparison with food-based dietary guidelines among adolescents by region of residence in Germany. Several differences in consumption were observed for former East and West Germany. These differences are especially seen among girls. One explanation for these differences may be that former East Germany has more rural regions, a different SES structure and a longer tradition of school meal supply and a higher utilisation of school meals(Reference Heide, Brettschneider and Lehmann42), which may contribute to the observed differences and may have a larger impact among girls. In Germany, the availability and usage of school meals have grown in recent years. In addition, there is a programme to improve the quality of these meals(Reference Arens-Azevêdo, Bölts and Girbardt43). This development may contribute to preferable changes in the diet of adolescents.
This study has strengths and limitations. A limitation is that information on food consumption was collected retrospectively and based on self-reports, which might lead to recall bias. Also, particular foods may be under-reported (e.g. confectionery, sugar-sweetened beverages) or over-reported (e.g. fruits and vegetables) due to social desirability. As a consequence, the deficits of food consumption may be larger. In addition, the assignment of food groups is very complex as composed foods can be included as such in a food group, that is, bread and cakes, while other composed foods, which cannot be assigned to a single food group, were decomposed to their ingredients, being assigned into the corresponding food groups. Although this process was highly standardised, conducted by a nutritionist and double-checked, some level of misclassification of single foods cannot be excluded. The consumption of fruits might be slightly higher than reported, as cakes were not decomposed into food groups. In case of disaggregating particular cakes containing fruits into their ingredients, there might be a shift in the allocation of foods to food groups from unfavourable foods to fruits. There are also some restrictions in comparison with the OMD amounts. The definition of food groups of the OMD is relatively broad and lacks some details about which particular foods should be included or excluded. Although the OMD does not specifically mention this, we assumed that the recommended amounts of the OMD refer to amounts of foods as consumed (not as raw quantities). These amounts were used as the basis for our calculations. In addition, the inclusion of sugar-sweetened beverages in the total amount of beverages as well as in the food group of the unfavourable foods is ambiguous. So, the consumption of fruit and vegetables expressed as proportion of recommended amounts may be underestimated, and evaluation of total beverage consumption does not differentiate between the contribution of preferable and non-preferable beverages. This study gives an overview of the recent food intake of adolescents in Germany and its distribution in subgroups. It is mainly a descriptive analysis without intending to detect causal relationships or to test a priori hypotheses. Nevertheless, many P-values are presented, and the implication of multiple testing should be considered. However, for this explorative situation using variables which are not completely independent (food groups as well as SES/region), a correction for multiple testing may be difficult and not appropriate, as suggested in literature(Reference Bender and Lange44,Reference Perneger45) . Nevertheless, the significance of results should be interpreted with caution. The strength of the study is that it was conducted nationwide with a large representative sample and reflects the food consumption of adolescents in Germany.
The results underline the need for interventions that improve the food consumption of adolescents, especially to accomplish the shift from a high consumption of unfavourable foods and meat to a higher consumption of fruit, vegetables, foods with complex carbohydrates and milk/dairy products or adequate substitutes. This is a major challenge for all public health professionals. In 2008, the national action plan ‘IN FORM – German national initiative to promote healthy diets and physical activity’ was launched with the aim to promote a healthy lifestyle with a balanced diet and sufficient exercise in all living environments. Already developed initiatives and strategies from federal and state governments and municipalities were complemented and deepened. Most measures, projects or recommendations take place in the living environment as a way to make changes in behaviour easier in everyday life. For instance, projects in schools can reach the whole generation of young people of all social levels(41). However, the observed differences in food consumption between EsKiMo I and II indicate that the existing measures may have led to only limited improvements in preferable food consumption so far. Further approaches to promote a healthy diet, such as easy to understand front-of-package labelling, a restriction on the promotion of unhealthy foods through all media and price policies for healthy and unhealthy foods, should be considered.
In conclusion, the current overview of the food consumption of adolescents in Germany shows that the consumption of fruit and vegetables is far below the recommendation, whereas the consumption of meat and unfavourable foods, like sugar-sweetened beverages and confectionery, is too high. Social disparities are seen in the consumption of soft drinks. This indicates that approaches to promote healthy diets should be continued and the focus on social inequalities should be strengthened.
Acknowledgements
Acknowledgements: First, we would like to thank the adolescents and their parents for their participation in EsKiMo II. We are also very grateful to the KiGGS staff and colleagues at the Robert Koch Institute who supported the conduction of the survey. We would especially like to thank the interviewers of EsKiMo II for their excellent work during the 2-year data collection phase. Financial support: The nutrition survey EsKiMo II was funded by the German Federal Ministry of Food and Agriculture (BMEL) on the basis of a resolution of the German Bundestag. Funding is provided by the German Federal Agency for Agriculture and Food (BLE), funding code 2814HS004. Conflict of interest: ‘None.’ Authorship: G.B.M.M. conceptualised, designed, managed and supervised the study. A.K.B. analysed the data for the manuscript, wrote the first draft and coordinated the field work of the study. C.L.B. coordinated the study. M.H. managed the study data. A.K.B., C.L.B., M.H. and F.L. assured consistency and quality control of the data. All authors contributed to analysis concepts and have read and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the ethics committee of the Hannover Medical School and the German Federal Commissioner for Data Protection and Freedom of Information as an amendment of KiGGS Wave 2 (No. 2275–2014). A written informed consent was obtained from all participants aged 14 years or older and all parents/caregivers.










 Open access
Open access