
Abstract
Introduction
Breast surgical oncology is a defined sub-specialty of general surgery that focuses on the surgical management of breast disease and malignancy within a multidisciplinary context. The fellowship directors (FD) that lead these programs have been selected for their abilities. As programs do research to ensure proper training for the next generation of breast surgical oncologists, we wanted to look into the FDs responsible for their training.
Methods
The Breast Surgical Oncology care program list was compiled via the Society of Surgical Oncology and American Society of Breast Surgeons Accredited programs (n = 60). The demographic information that was of interest included, but was not limited to, gender, age, ethnicity/background, past residency training, past fellowship training, year graduated from residency and fellowship, year since graduation to FD appointment, time at institution till FD appointment, and Hirsch index (h-index).
Results
Data were collected on all 60 FDs. The average age of FDs was 52 years old, 27% of FDs are men and 73% of FDs are women. The average H-index, number of publications, and number of citations were 19, 67, and 2648, respectively. The mean graduation year from residency was 2003, and from fellowship was 2006; with a mean of 9 years post fellowship graduation until becoming an FD. The most frequently attended residency was Rush (n = 4), and the most common fellowships were Memorial Sloan Kettering (n = 8), MD Anderson Cancer Center (n = 7), and John Wayne Cancer Institute (n = 4). Nine of the FDs stayed at the same institution after doing both residency and fellowship there (15%).
Conclusion
This is the first study to examine the demographics of those in FD positions in Surgical Breast Oncology, which is a relatively young fellowship. We found that FDs in Breast Surgical Oncology are defined by their high output of research. This qualification may be why the average age, and the number of years to FD are higher compared to other specialties where this research has been undertaken. Initial evaluation of FDs suggest more diversity in this field is needed. Further insight into the leaders training our next generation of surgeons is warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast surgical oncology is a defined sub-specialty of general surgery that focuses on the surgical management of breast disease and malignancy within a multidisciplinary context [1]. This is a relatively new surgical subspecialty that has grown incredibly quickly since the inception of its first fellowship programs nearly 30 years ago [2]. Rapid changes in breast oncology management and practice have further ascertained the need for dedicated expertise in the field; however, it is unclear how it has affected those in the fellowship director role (FDs). Training programs are structured to develop excellence in their trainees in advanced surgical techniques and clinical decision-making as well as exposure to the multidisciplinary aspects of breast cancer management. The fellowship directors that lead these programs have been explicitly selected for their ability to achieve these goals. The Society of Surgical Oncology (SSO) sets requirements that FDs must meet prior to appointment, such as certification by the American Board of Surgery or subspecialty qualifications acceptable to the SSO Training Committee and certain scholarly requirements. However, other qualifications of these requirements are broad in their description and do not provide explicit prerequisites. Thus, our group seeks to identify the detailed measurable factors that directly influence the selection of FDs [3].
FDs have incredible influence on the future of trainees within the field. Understanding the characteristics and attributes that breast surgical oncology FDs share may allow trainees, as well as burgeoning leaders, to better understand how these programs have been able to develop excellent breast surgeons. There have been a number of similar leadership papers published in accredited specialties that may now further serve as a roadmap for future leaders [4,5,6,7,8,9]. No previous study has analyzed demographics and prior training of FDs in the field of breast surgical oncology. Using a sample of all current breast surgical oncology FDs, we sought to analyze demographic background, institutional training, and academic experience to find the distinct qualifications that may have paved the ascent to their current role.
Methods
Data source and collection
The Breast Surgical Oncology program list was compiled via Society of Surgical Oncology and American Society of Breast Surgeons Accredited programs and fellowship-specific information was collected on institutional websites (accessed November 5, 2021) and was reviewed to incorporate all breast surgical oncology fellowships in North America (n = 59) and Canada (n = 1). All listed FDs with established program director roles within each fellowship program were listed for data collection. This generated a list of 60 programs and 60 directors, of which all 60 were included in this study. We did not include co-directors or associate directors in this study. All FDs were identified first through the fellowship directory, and subsequently confirmed via their university or hospital fellowship information webpage. The professional education history, residency, residency year, fellowship, and fellowship year were obtained through their respective institutional biographies, Doximity (Doximity.com, Doximity Inc., San Francisco, CA), and curricula vitae (CV), and/or LinkedIn (Linkedin.com, Sunnyvale, CA). The information was cross-referenced between these platforms when applicable. The age of each FD was established using Healthgrades (Healthgrades Operating Company Inc, Denver, CO).
After initial data collection, email questionnaires were sent directly to FDs via listed email and/or program coordinator email to acquire the respective FD’s CV, which combined, were used to assess and/or confirm the year hired by their institution, year appointed to the fellowship director position, and other demographic information that was not readily available via their respective webpages. CVs, when sent by FDs, were author reviewed for the missing information, and used to cross-check publicly available information. The demographic information that was of interest included, but was not limited to, gender, age, ethnicity/background, past residency training, past fellowship training, year graduated from residency and fellowship, year since graduation to FD appointment, time at institution till FD appointment, and Hirsch index (h-index). For non-responders to surveys, the FD and/or coordinators of the program were called twice by the lead author, and emailed multiple times to attempt to gain contact.
Leadership in national societies
Involvement in a national society, such as Society of Surgical Oncology, American Society of Breast Surgeons, and American Cancer Society, or other, was collected via questionnaires or CVs. Leadership was defined as holding a position, such as President, President-Elect, Vice President, Secretary, or Chair of any of the various committees, in any of the national societies. Those who were committee members were excluded from the total count of leadership positions.
Research productivity and impact
Level of scholarly or research productivity and impact was measured by the use of each individual’s number of publications, citations, and h-index. H-index is a numerical value associated with the number of publications that are then cited at the same rate and is a way to quantify scientific output of a researcher [10]. This metric has been used in a number of similar previously published papers [11,12,13]. The h-index, publication count, and citation count were obtained for each FD by searching their full first name and last name within the Scopus database (Elsevier B.V., Waltham, MA, USA). All data collected by the authors were reviewed, verified, and cross referenced to ensure accuracy. Scopus was used to retrieve the publication count, citation count, and H-index for every FD in the study. Pearson’s correlation coefficients were determined via Statistical Analytics System (Version 9.4 of the SAS System. Copyright © 2013 SAS Institute Inc) software. Data were interpreted according to the guide of Mukaka for correlation coefficients. Values under 0.3, 0.3–0.5, 0.5–0.7, 0.7–0.9, and greater than 0.90 are indicative of negligible, low, moderate, high, and very high positive correlation, respectively.
Statistical analysis
The following data points were gathered for each fellowship leader as set forth by previous leadership papers: current institution, number of years in current role, specific role, age, name of residency institution and year of graduation, name of fellowship institution and year of graduation, year hired by current institution, year appointed FD, and Scopus H-index. Added data points included publication count, citation count, and leadership positions in national surgical and surgical oncological societies [5]. All of the data were recorded and analyzed using Excel 365 (Microsoft Inc, Redmond, WA). Mann–Whitney U tests were conducted between groups for non-parametric data. Statistical significance was considered at an alpha value of p < 0.05.
Results
There were a total of 60 FDs included in the study, of which 17 (28.33%) were males and 43 (71.67%) were females (Table 1). The mean age of FDs was 52.3 years (SD = 9.1, median 51, min 37, max 74, n = 50) (Table 1). There was a statistically significant difference between the mean age of female FDs and male FDs (50.25 vs. 57.57 years, p = 0.0091). The average age of FDs at time of appointment was 47 (SD = 9, n = 32). The breakdown of distribution by race and ethnicity was self-reported via E-mail survey and was as follows; Twenty-eight total respondents (46.7% of FDs) 22 White/Caucasian (78.6%), 3 Asian (10.7%), 2 Hispanic (7.1%), and 1 Black (3.6%). We only evaluated race/ethnicity on self-reporting, and not on evaluation from institutional websites or other sources.
Residency information was available for all FDs, and the average calendar year of graduation from residency was 2003 (SD = 10 n = 48) (Table 2). Fellowship information was available for all FDs that attended fellowship programs; however, 5 FDs did not complete fellowship training. The average age for these 5 individuals was 61.6 years, with an average residency graduation year of graduation of 1991. Overall, the average calendar year of graduation from fellowship was 2006 (SD = 9, n = 44) (Table 2). The mean duration from residency graduation until appointment to the position of FD was 18 years (SD = 10, n = 48), while the mean duration from fellowship graduation to appointment was 11 years (SD = 8, n = 34). The average length of duration of employment at the FD’s current institution until the time of this study was 11 years (SD = 7, n = 49), while the average length of time between hire and FD appointment was 5 years (SD = 6, n = 37). The mean duration of tenure from appointment to the date of this study was 6 years (SD = 5, n = 37) (Table 2).
Institutional loyalty was compared by assessing the FDs’ institutions for residency, fellowship, and FD appointment. Three FDs were at the same institution for residency as they were in their current employment (5%), while 8 (13.3%) of FDs also maintained loyalty at their same fellowship (Table 2). Only 1(1.67%) FD was appointed at the same institution they completed both their residency and fellowship training, although 9 (15%) FDs completed training at the same residency and fellowship institutions.
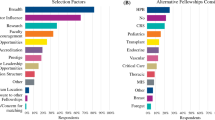
The top five residency institutions that ultimately produced the most future FDs were assessed and are Rush Presbyterian St. Luke’s Medical Center (n = 4), Medical University of South Carolina (n = 2), Johns Hopkins University (n = 2), UCLA (n = 2), and Baylor College of Medicine (n = 2). The top three fellowship institutions that ultimately produced the most future FDs were assessed and are displayed in Fig. 1. The top institutions were Memorial Sloan-Kettering Cancer Center (n = 8), UT MD Anderson Cancer Center (n = 7), and University of Arkansas and John Wayne Cancer Institute were tied (n = 4).

Fellowship programs that produced the most surgical breast oncology FDs
Scholarly performance was assessed using the Scopus h-Index, number of publications, and number of citations of which data for all FDs were available. There was significant, moderate strength correlation between age and h-index (r = 0.6, p = < 0.0001). Significant, moderate correlation was found between time since residency graduation and h-index (r = 0.63, p < 0.0001). H-indices ranges were grouped, and the number of total FDs in each range were assessed as follows: 0–10 (n = 23), 10–20 (n = 14), 20–30 (n = 10), 30–40 (n = 7), 40–87 (n = 4) (Fig. 2).

Scopus h-indices for all surgical breast oncology FDs distributed by frequency of 10 s. The symbol “(indicates that the range includes the adjacent value. The symbol)” indicates that the range does not include the adjacent value. Of note, these h-indices were collected on November 4, 2021, so these figures may be different since the time elapsed since collection
Gender-wise comparison of mean h-indices revealed a mean H-index of 27 for males and 16 for females, with a significant difference between the two groups (p = 0.0195). Individual linear regressions for age and H-index grouped by gender showed r2 = 0.2567 (p = 0.0016) and r2 = 0.4879 (p = 0.0055) for females and males, respectively. The H-index measurement correlation between age and sex is stronger in male FDs compared to female FDs. As a summary of H-indices; the mean H-index was 19.12 (SD = 16.62, median 14, min 0, max 87, n = 60). In terms of total publications, the mean number of publications at time of this study was 69.2 (SD = 88.5, median 35, min 0, max 456, n = 60). Finally, mean number of citations was 2773.9 (SD = 5027.6, median 971, min 0, max 33,828, n = 58).
Leadership within breast surgical oncology FDs was measured by leadership roles in national organizations which was acquired via questionnaire. Four (18.2%, n = 22 responses, 6.67% of total), reported having a leadership role in the Surgical Society of Oncology, four reported having a leadership position in American Society of Breast Surgeons (18.2%, n = 22 responses, 6.67% of total); two of these FDs had leadership in both societies. Seventeen (28.3%) of FDs had a secondary degree; 4 (6.67%) PhDs, 3 (5%) MBAs, 2 (3.33%) MPHs, and 8 (13.3%) other master’s degrees (listed as MA, MS, MSc, MHCM). Eight (42% n = 19 responses, 13.3% of total) of FDs reported being on an editorial board (Journals ranging from; Annals of Surgical Oncology, Annals of Surgery, Breast Journal, American Journal of Surgery, Current Breast Cancer Reports, Surgery, Journal of Clinical Oncology, Journal of Surgical Oncology, and Journal of Surgical Research). Eleven (18.3%) of FDs reported on their institutional homepage, CV, or other that they had completed more than one fellowship.
Discussion
Age and years from post-fellowship completion to FD appointment
This current study summarizes the demographics, academic and research backgrounds, and leadership appointments of the FDs of breast surgical oncology fellowship programs. In this cohort, the average age of appointment to the FD position was 46 years old, with FDs achieving appointment 11 years following fellowship training completion. Having ample time dedicated to the breast surgical oncology specialty prior to FD appointment allows for appointees to establish themselves professionally, ensuring that future trainees are provided the best scholarly and educational experience. Compared to other fellowships with reported statistics, breast surgical oncology FDs were 18 years out from their residency graduation and, at the time of this cross-sectional research, were 52 years old and had been in their roles for 6 years, on average. Our findings are similar to similar reports across other specialties (spine surgery FDs = 52.9 years old, Cardiothoracic surgery FD 52 years old, Interventional radiology- 47.39 years old, ophthalmology residency PDs- 42.9 years old) [5, 7, 8, 14]. This is likely due to both objective and subjective requirements to ascend to the FD role, likely including research output, faculty appointment, and other institutional leadership positions that further support the experience required to hold this position.
Our research suggests that the average tenure as FD, time to FD, and time at the current institution is 6, 5 and 11 years respectively. SSO only requires that FDs be 2 years removed from fellowship before attaining the role of FD. We believe that this mandate may have been created to minimize overlap between colleagues and to ensure proper experience particularly in the attending role with increased surgical, clinical, and administrative responsibility as a young surgeon. With 11 years of academic practice, FDs should be well equipped to train upcoming surgeons, conduct meaningful research, and understand the direction of the field. However, this large gap encountered in our research between fellowship graduation to appointment of FD, could foster, lead to a disconnect between the needs of current fellows and the perspectives of their FD. Further investigation in regard to trainees would be needed to fully answer this question. Academic breast surgeons who strive for the FD position could be at a single institution for a decade, unless they are hired as an FD at a different institution and ascend in this manner. Within our results, there was large standard deviations with this metric, so this hypothesis would need more data from other general surgery fellowships to draw larger conclusions. It does appear that breast surgical oncologists ascend in a stepwise fashion over years of training through hire to FD. This may be of additional concern, especially when considering the high burnout rate associated with surgical sub-specialization and other physician professionals. A recent 2021 study suggested that breast surgeons who have been in practice for 5–9 years have particularly high overall burnout rates. In a survey conducted among members of the American Society of Breast Surgeons, 40% of respondents report feeling burnt out [15, 16]. The American College of Surgeons conducted a survey in 2008 to evaluate burnout and career satisfaction among surgeons, which included 7905 respondents, 407 of whom were surgical oncologists. Surgical oncologists had a similar incidence of burnout, and better indices of career satisfaction relative to all other surgical specialties [17]. In addition to the years required to become a surgeon in a subspecialty, the burnout is further aggravated by the additional experience required to become an FD and time spent at a single institution [18]. Additional support, such as protected academic time, additional personnel to assist in non-clinical tasks, and increased pay may mitigate high rates of burnout. Implementation of these resources functions to keep academic surgeons at their home institutions as well as to ensure that FDs can progress professionally while limiting the risk of burnout.
Gender and ethnicity
In our study, 28.33% of PDs were male and 71.67% were female. Compared to other specialties, i.e., neurointerventionalists (7.7% female) and spine specialists (4% female), surgical breast oncology FDs had a much higher female representation within leadership positions [5, 19]. Additionally, mean H-index in Breast surgery fellowship faculty increased with rank for both genders, however H-index was significantly higher for male compared to female professors. Moreover, linear regression showed a stronger r2 for age versus H-index in men as compared to females (0.4879 vs. 0.2567). While more data are needed, the data do suggest that men have a higher h-index compared to women FDs due to tenure, and time in the field. With more years in practice, the FDs H-index is likely to be significantly higher. Despite women making up a majority of FDs, it was found previously that they are underrepresented overall at higher academic ranks, and the average h-index for male professors in breast surgery were higher than their female counterparts [20]. This representation of women FDs is in stark comparison to 14 surgical subspecialty fields in which this has been studied, where women only represented < 20% of the fellowship directors. [21]. However, breast surgery programs have a significantly higher proportion of women comparatively in positions of leadership. In years past, a combination of gender bias in the medical environment and lack of mentors could have had a negative impact by creating and perpetuating gender discrepancies [22]. There may be cultural, institutional, or specific mentorship roles that have influenced the proportion of female to male FDs in Breast Surgical oncology. It may also be due to the type of pathology being treated in this field of surgery, as women are the primary population affected. Female surgeons may be more motivated to enter the field of breast surgery than their male surgeon counterparts due to the draw toward this patient population. This discrepancy could also be due to higher participation among women at national breast conferences and societies [23]. This participation may increase likelihood of career advancement through research production, relationship formation, committee participation, and presentations given to wide audiences.
Men far outnumber women in the leadership roles of General Surgery PDs and ADPs at 82 and 70% respectively [24]. As evidenced by breast oncology surgery FDs, the climate of women in academic leadership appears to be changing. In other surgical sub-specialty fields; however, there is room to grow, as evidenced by thoracic surgery PDs (90% men, 10% women) and Abdominal transplant surgery (83% men, 17% women) [8, 25]. These male dominated numbers hold true among other sub-specialty FDs including interventional radiology, ophthalmology, orthopedic reconstruction, radiologists, and gastroenterology [7, 9, 26, 27]. Currently, surgical oncology/complex surgical oncology does not have a similar demographic paper published in the literature to our knowledge. This represents an opportunity to evaluate surgical oncology FDs in future.
In our study, we found very limited diversity among FDs. A majority (78%) of FDs reported to be White/Caucasian, with minorities making up the remaining 22% (8.7% Asian, 8.7% Hispanic, and 4.4% African American). Although the feedback from our respondents was narrow, with only 40% of FDs responding, it is clear that progress is needed to continue to broaden the race and ethnicities of FDs. Interestingly, data show that 81% of new breast cancer diagnoses are made in white women, 11.6% in Black women, 4.7% in Asian and Pacific Islander women, and in 8.8% Hispanic women [28]. The percentage of minority FDs are not representative of the population of breast cancer minority patients, which shows that there is continued room to grow. Larger conclusions on race and ethnicity in this study, however, remain limited. Overall, our analysis identifies that pipeline programs, as well as other initiatives to increase representation among minorities are warranted.
Leadership transition and diversification
Mentorship has a known role in both medical and surgical education, as well as career advancement [29]. Current fellowship directors in breast oncology can play a role in setting up the next generation of FDs by having a set plan and time course for transitions of power. Further, in selecting this next generation of leaders, we should obtain excellence for the profession through diversity. Education, both formal and informal, may be instrumental in leadership transition. Expertise in complex hospital organization, financial and quality of care measures, and other administrative duties that come with being in leadership should be intertwined in leadership education prior to becoming chair or FD [13]. The fellowships at Memorial Sloan Kettering Cancer Center and, MD Anderson Cancer Center both accept four fellows a year, which may result in the larger number of FDs (25% of all FDs) produced by these programs. However, John Wayne Cancer Institute and University of Arkansas only offer one and two spots, respectively, yet they proportionally produced a large number of FDs (13.3% of all FDs). It is not clear why this is the case, this may be secondary to institutional focus or historical opportunities due to the amount of time they have existed.
Other degrees, fellowship training, training location and institutional exposure
While there is no defined path to become FD, there is some similarity in the educational journey of those in leadership positions. Seventeen (28.3%) of FDs had additional degrees, the most common being an MS, followed by PhD. Four (6.67%) FDs pursued a PhD degree; the low number of FDs with a PhD in breast oncology may be due to the extensive training time. Surgical breast oncology programs are part of broadly academic health centers which may attract MD-PhD trainees as they are more likely to receive funding for their research at these institutions [30]. This would allow for individuals interested in leadership positions to have access to better opportunities, such as fellowship director roles, at those institutions. In addition to additional degrees, 11(18.3%) FDs had additional fellowship training in research and advanced gastrointestinal/MIS with research fellowship training being the most popular. Trainees with robust prior research experience could be better poised both for acceptance into breast surgical oncology programs as well as leadership positions in future.
Further influence on the ability for individuals to ascend to the FD position stems from institutional exposure through residency, fellowship, or length of tenure at their institution. Previous research in interventional radiology program directors described that nearly half (45%) of PDs had exposure to that institution before becoming the PD [7]. This could be due to personal connections, prior training, or research relationships created before achieving the leadership role. Similarly, in orthopedic sports medicine, 22% of FDs worked at the same institution they completed fellowship at [4]. This observation is even more striking in the surgical sub-specialty of cardiothoracic surgery, where 60% of FDs stay in the same region, and 30% had institutional exposure to their program via medical school or training [8]. Within oncology, a survey of surgical oncology fellowship graduates from 2005–2016 found that 57% of respondents took their first positions out of fellowship at university-based/affiliated hospitals, with 15% returning to their home residency institution [31]. In our study, there were 3 (5%) of FDs working at the same institution as residency training, 9 (15%) at the same institution as fellowship training, and 9 (15%) who completed both residency and fellowship at the same institution. These numbers may be influenced by job availability at the time, and trends in breast disease nationally.
Previous research shows that surgical trainees cite increased income potential as a motivation for pursuing fellowship training, despite financial return of fellowship being highly variable [33]. Financial incentives of private practice vs hospital employed practice vs academic careers may be a limitation for retaining academic faculty, and therefore potential FDs, although more data and research into this would be needed before drawing any conclusions [34]. We do observe however, limited institutional loyalty and retainment among FDs.
Further, geographic distribution of healthcare resources can be influential on where physicians decide to train. Recent research has shown a positive correlation between breast cancer incidence and the National Accreditation Program for Breast Centers (NAPBC) program distribution throughout the United States [32]. Our study demonstrates that breast oncology FDs are concentrated in areas with NAPBC designations as follows: 12 (20.34%) programs in the Midwest, 21 (35.59%) in the Northeast, 18 (30.51%) in the South, and 8 (13.56%) in the West. The ability to practice in an area with a high case load may benefit FDs and programs through the ability to have larger clinical trials and studies, thus advancing the field of breast oncology further, as well as their individual careers.
Research and leadership
Research productivity was high among breast surgical oncology FDs with mean publications, citations, and h-index being 69, 2774, and 19.12 respectively. The large standard deviation within these values can be attributed to the difference in interest, dedicated time, and degree of research focus of the different programs. Top surgeon scientists among breast surgeons based on Scopus H-index include Dr. Armando Giuliano (87), Dr. Patrick Borgen (60), Dr. Judy Boughey (49), Dr. V. Suzanne Klimberg (48) and Dr. Brian Czerniecki (48). However, by distribution, these FDs make up a minority of all FDs. Most commonly, FDs have H-indices of 0–10 (23 FDs), followed by 10–20 (14 FDs). Many studies note that research productivity of a PD while holding their leadership position is reduced secondary to the time commitment of the position [35].
A recent paper found that H-index among breast surgery faculty for both genders increased with rank, however, it also found that H-index was significantly higher for men professors compared to women professors [20]. These findings are similar to those reported in another study assessing the composition of academic cardiology program leadership in which women had lower h-index values than men [36]. Our research has found that among FDs, 2 out of the top 5 highest H-indices belonged to women, and that there was a significant difference between men and women’s H-index among the FDs. The H-index overall from breast surgical oncology FDs is similar to other published data in surgical specialties compared to ophthalmology residency PDs (8.7), orthopedic reconstruction FDs (16.5), Orthopedic sports FDs (23.5), and Orthopedic pediatric FDs (17.2) [4, 9, 14, 37]. Interestingly, in a review of academic neurology leaders, it was found that although men outnumber women at all faculty ranks, the gap between men and women in publications narrows with advancing rank [38]. By having more opportunities for women in academic positions, equality may increase in research output and academic productivity.
While H-index provides a metric to evaluate cumulative scholarly output, it is not the most reliable way to measure success. In addition to research commitments, 5 (n = 19 respondents) of FDs also hold leadership positions in National Societies and 7 (n = 16 respondents) are on journal editorial boards, the most common being Annals of Surgical Oncology. This is of importance to us, because earlier studies of almost 2700 young surgeons in American College of Surgeons (< 45 years) found that 4.7% were medical students, 41% were resident members, 18.2% were associate fellow members, and 35.4% were fellows [39]. By joining professional organizations, young students, residents, fellows, and junior faculty may be able to ascend to leadership positions through mentorship and holding meaningful roles in a number of these societies. Among the many accolades our study population may possess, teaching awards in the clinical science and surgical education that are institution specific and highlight a clinician’s value to their pupils. Because of the lack of centralized record of these institution specific awards, these data were not available for this study, and must be reviewed on a case-by-case basis.
Limitations
There are several limitations of this study, including a lack of a comprehensive database of all available breast surgical oncology fellowships in the country, and the hesitancy of FDs to share personal information. Although we tried to identify a comprehensive list of fellowship programs, it is possible that some programs are not included as we did not have access to an official database of available fellowship programs. Additionally, the nature of personal information collected results in hesitancy of FDs to share their information and CVs, leading to missing and incomplete data collection. Of note, a number of emails were no longer in use, and/or were undeliverable for a variety of reasons. Future studies may focus on interpersonal relationships that may contribute to ascending to the FD position, a more in-depth data collection including rankings of fellowships, and training by specific physicians, although any data collection may face the same challenges as outlined above.
Due to the times we live in, we would be remiss without mentioning how SARS-CoV-2 may affect the future of FDs. Thus far, most fellowship programs have transitioned to virtual interviews to adapt to the limitations of our active global pandemic [40]. Future research could examine how institutional or regional leadership may be changing during and post pandemic.
Breast surgical oncology fellowship directors are likely to be a female, in their early 50 s, who have practiced in the field for over 18 years with a strong research output. All in all, we believe that this study sets the precedent for future investigations studies in general surgery sub-specialties to examine trends and demographics in the FD role. Further, this study sets up a roadmap of sorts, for aspiring academic breast surgeons. With further research in this area, we can continue to examine where improvements in diversity, burnout, and gender equality can be made.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Teshome M, Kuerer HM. Training of breast surgical oncologists. Chin Clin Oncol. 2016;5(3):43.
Berman RS, Weigel RJ. Training and certification of the surgical oncologist. Chin Clin Oncol. 2014;3(4):45.
Sclafani LM, et al. Training a new generation of breast surgeons: are we succeeding? Ann Surg Oncol. 2012;19(6):1856–61.
Schiller NC, et al. Trends in leadership at orthopaedic surgery sports medicine fellowships. World J Orthop. 2021;12(6):412–22.
Donnally CJ 3rd, et al. Trends in Leadership at Spine Surgery Fellowships. Spine. 2020;45(10):E594-e599 ((Phila Pa 1976)).
Webber GR, et al. A survey of diagnostic radiology residency program directors and the increasing demands of program leadership. J Am Coll Radiol. 2013;10(7):523–6.
Wadhwa V, et al. Descriptive analysis of interventional radiology residency program directors in the United States. Clin Imaging. 2020;68:232–5.
Singh SK, et al. A cross-sectional review of cardiothoracic surgery department chairs and program directors. J Surg Educ. 2021;78(2):665–71.
Schiller NC, et al. Trends in leadership at orthopedic surgery adult reconstruction fellowships. J Arthroplasty. 2020;35(9):2671–5.
Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U S A. 2005;102(46):16569–72.
Gershoni A, et al. Academic background, professional experience, and research achievements of United States academic ophthalmology leadership 1971. Irish J Med Sci. 2021. https://doi.org/10.1007/s11845-020-02495-x.
Patel A, et al. Demographics of surgical specialty residency program directors in the united states: a cross-sectional analysis. Annals of Surgery Open. 2021;2(1):e044.
Lee TC, et al. The road to academic surgical leadership: Characteristics and experiences of surgical chairpersons. Surgery. 2020;168(4):707–13.
Kloosterboer A, et al. Residency program directors of united states ophthalmology programs: a descriptive analysis. Am J Ophthalmol. 2020;209:71–6.
Zhang JQ, et al. Assessing burnout and professional fulfillment in breast surgery: results from a national survey of the american society of breast surgeons. Ann Surg Oncol. 2019;26(10):3089–98.
James TA, Zhang JQ. ASO author reflections: a closer look at burnout and professional fulfillment in breast surgery. Ann Surg Oncol. 2019;26(Suppl 3):717–8.
Balch CM, et al. Burnout and career satisfaction among surgical oncologists compared with other surgical specialties. Ann Surg Oncol. 2011;18(1):16–25.
Zhang JQ, et al. Burnout and professional fulfillment in early and early-mid-career breast surgeons. Ann Surg Oncol. 2021;28(11):6051–7.
Vilanilam GK, et al. Analysis of demographic and educational backgrounds of interventional neuroradiology fellowship program director workforce in North America. Curr Probl Diagn Radiol. 2021;50(4):477–80.
Radford DM, et al. h-index and academic rank by gender among breast surgery fellowship faculty. J Womens Health (Larchmt). 2021;31(1):110–6.
Filiberto AC, et al. Gender differences among surgical fellowship program directors. Surgery. 2019;166(5):735–7.
Zhuge Y, et al. Is there still a glass ceiling for women in academic surgery? Ann Surg. 2011;253(4):637–43.
Chang JH, et al. Has breast surgery shattered the glass ceiling? trends in female representation at the american society of breast surgeons annual meeting 2009–2019. Ann Surg Oncol. 2020;27(12):4662–8.
Carpenter AM, et al. Gender diversity in general surgery residency leadership. J Surg Educ. 2018;75(6):e68–71.
Choubey AP, et al. Diversity among transplant surgery fellowship program directors: a call to action. HPB (Oxford). 2021;24(3):386–90.
Goswami AK, et al. Academic radiology in the united states: defining gender disparities in faculty leadership and academic rank. Acad Radiol. 2021;29(5):714.
Woodward Z, et al. Gender disparities in gastroenterology fellowship director positions in the United States. Gastrointest Endosc. 2017;86(4):595–9.
Prevention CfDCa. Leading Cancers by Age, Sex, Race and Ethnicity. U.S. Cancer Statistics 2018 [cited 2021; Available from: https://gis.cdc.gov/Cancer/USCS/#/Demographics/.
Entezami P, Franzblau LE, Chung KC. Mentorship in surgical training: a systematic review. Hand (N Y). 2012;7(1):30–6.
Brass LF, et al. Are MD-PhD programs meeting their goals? An analysis of career choices made by graduates of 24 MD-PhD programs. Acad Med. 2010;85(4):692–701.
Ruff S, et al. Survey of surgical oncology fellowship graduates 2005–2016: insight into initial practice. Ann Surg Oncol. 2019;26(6):1622–8.
Pardo JA, et al. Impact of geographic distribution of accredited breast centers. Breast J. 2020;26(11):2194–8.
Inclan PM, et al. For love, not money: the financial implications of surgical fellowship training. Am Surg. 2016;82(9):794–800.
Killelea BK, et al. The 2018 compensation survey of the american society of breast surgeons. Ann Surg Oncol. 2019;26(10):3052–62.
Gilbert DL, et al. Child neurology residency program directors and program coordinators 2016 workforce survey. Pediatr Neurol. 2018;79:21–7.
Khan MS, et al. Women in leadership positions in academic cardiology: a study of program directors and division chiefs. J Womens Health (Larchmt). 2019;28(2):225–32.
Cohen LL, et al. Trends in leadership at pediatric orthopaedic fellowships. J Pediatr Orthop. 2021;41(6):385–8.
McDermott M, et al. Sex differences in academic rank and publication rate at top-ranked US neurology programs. JAMA Neurol. 2018;75(8):956–61.
Cherr GS, et al. Young surgeons’ attitudes regarding surgery and professional organizations. Am J Surg. 2009;198(1):142–9.
Vining CC, et al. Virtual surgical fellowship recruitment during COVID-19 and its implications for resident/fellow recruitment in the future. Ann Surg Oncol. 2020;27(Suppl 3):911–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors did not receive support from any organization for the submitted work.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Schachner, B., Fanfan, D., Zippi, Z. et al. Trends in leadership at breast surgical oncology fellowships. Global Surg Educ 1, 49 (2022). https://doi.org/10.1007/s44186-022-00046-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44186-022-00046-9