
Abstract
Background
Approximately one-quarter of emergency department (ED) visits for alcohol withdrawal result in unscheduled 1-week ED return visits, but it is unclear what patient and clinical factors may impact this outcome
Methods
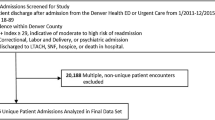
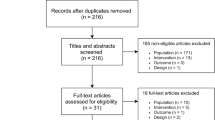
From January 1, 2015, to December 31, 2018, at three urban EDs in Vancouver, Canada, we studied patients who were discharged with a primary or secondary diagnosis of alcohol withdrawal. We performed a structured chart review to ascertain patient characteristics, ED treatments, and the outcome of an ED return within 1 week of discharge. We used univariable and multivariable Bayesian binomial regression to identify characteristics associated with being in the upper quartile of 1-week ED revisits.
Results
We collected 935 ED visits among 593 unique patients. Median age was 45 years (interquartile range 34 to 55 years) and 71% were male. The risk of a 1-week ED revisit was 15.0% (IQR 12.3; 19.5%). After adjustment, factors independently associated with a high risk for return included any prior ED visit within 30 days, no fixed address, initial blood alcohol level > 45 mmol/L, and initial Clinical Institute Withdrawal Assessment—alcohol revised score > 23. These factors explained 41% of the overall variance in revisits.
Conclusion
Among discharged ED patients with alcohol withdrawal, we describe high-risk patient characteristics associated with 1-week ED revisits, and these findings may assist clinicians to facilitate appropriate discharge planning with access to integrated follow-up support.
Résumé
Contexte
Environ un quart des visites aux urgences pour sevrage alcoolique se traduit par un retour non programmé aux urgences pendant une semaine, mais les facteurs cliniques et relatifs aux patients qui peuvent avoir une incidence sur ce résultat ne sont pas clairs.
Méthodes
Du 1er janvier 2015 au 31 décembre 2018, dans trois urgences urbaines de Vancouver, au Canada, nous avons étudié les patients qui sont sortis avec un diagnostic primaire ou secondaire de sevrage alcoolique. Nous avons procédé à une analyse structurée des dossiers afin de déterminer les caractéristiques des patients, les traitements aux urgences et l'issue d'un retour aux urgences dans la semaine suivant la sortie. Nous avons utilisé une régression binomiale bayésienne univariable et multivariable pour identifier les caractéristiques associées au fait d'être dans le quartile supérieur des visites aux urgences à une semaine.
Résultats
Nous avons recueilli 935 visites aux urgences parmi 593 patients uniques. L'âge médian était de 45 ans (intervalle interquartile de 34 à 55 ans) et 71 % étaient des hommes. Le risque d'une nouvelle visite aux urgences à une semaine était de 15,0% (IQR 12,3 ; 19,5%). Après ajustement, les facteurs indépendamment associés à un risque élevé de retour comprenaient toute visite antérieure à l’urgence dans les 30 jours, aucune adresse fixe, le taux d’alcoolémie initial > 45 mmol/L, et l’évaluation initiale du sevrage de l’Institut clinique – cote d’alcoolémie révisée > 23. Ces facteurs expliquaient 41 % de la variance globale des visites.
Conclusions
Parmi les patients sortants des urgences en sevrage alcoolique, nous décrivons les caractéristiques des patients à haut risque associés à la réadmission aux urgences après une semaine de sevrage alcoolique. Ces résultats peuvent aider les cliniciens à planifier de manière appropriée la sortie de l'hôpital et à accéder à un suivi intégré.

Similar content being viewed by others

Data availability
De-identified data herein are accessible to other interested parties by application to the corresponding author.
References
Canadian Institutes for Health Information. Alcohol Harm in Canada. 2017. Available at https;//www.cihi.ca/sites/default/files/document/report-alcohol-hospitalizations-en-web.pdf. Accessed August 23, 2022
Myran DT, Hsu AT, Smith G, Tanuseputro P. Rates of emergency department visits attributable to alcohol use in Ontario from 2003 to 2016: a retrospective population-level study. CMAJ. 2019;191:804–10. https://doi.org/10.1503/cmaj.181575.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington: American Psychiatric Publishing 2013DSM; 2013.
British Columbia Center for Substance Use. Provincial guidelines for the clinical management of high-risk drinking and alcohol use disorder. 2019. Available at https://www.bccsu.ca/wp-content/uploads/2020/02/AUD-Guideline.pdf. Accessed April 27, 2022.
Kahan M, Borgundvaag B, Midmer D, et al. Treatment variability and outcome differences in the emergency department management of alcohol withdrawal. CJEM. 2005;7:87–92. https://doi.org/10.1017/s1481803500013038.
D’Onofrio G, Rathley NK, Ulrich AS, et al. Lorazepam for the prevention of recurrent seizures related to alcohol. NEJM. 1999;340:915–9. https://doi.org/10.1056/NEJM199903253401203.
Rosenson J, Clements C, Simon B, et al. Phenobarbital for acute alcohol withdrawal a prospective randomized double-blind placebo-controlled study. J Emerg Med. 2013;44:592-98.e2. https://doi.org/10.1016/jemergmed.2012.07.056.
Hendey GW, Dery RA, Barnes RL, et al. A prospective, randomized, trial of phenobarbital versus benzodiazepines for acute alcohol withdrawal. Am J Emerg Med. 2011;29:382–5. https://doi.org/10.1016/j.ajem.2009.10.010.
Nelson AC, Kehoe J, Sankoff J, et al. Benzodiazepines vs barbiturates for alcohol withdrawal: analysis of 3 different treatment protocols. Am J Emerg Med. 2019;37:733–6. https://doi.org/10.1016/jajem.2019.01.002.
Scheuermeyer FX, Miles I, Lane DJ, et al. Lorazepam versus diazepam in the management of emergency department patients with alcohol withdrawal. Ann Emerg Med. 2020;76:774–81. https://doi.org/10.1016/j.annemergmed.2020.05.029.
Chan AH, Ho SF, Fook-Cong C, et al. Characteristics of patients who made a return visit within 72 hours to the emergency department of a Singapore tertiary hospital. Singapore Med J. 2016;57:301–6. https://doi.org/10.11622/smedj.2016104.
Verelst S, Pierloot S, Desruelles D, et al. Short-term unscheduled return visits of adult patients to the emergency department. J Emerg Med. 2014;47:131–9. https://doi.org/10.1016/j.jemermed.2014.01.016.
Safwenberg U, Terent A, Lind L. Increased long-term mortality in patients with repeated visits to the emergency department. Eur J Emerg Med. 2010;17:274–9. https://doi.org/10.1097/MEJ.0b013e3283104016.
Wu CL, Wang FT, Chiang YC, et al. Unplanned emergency department revisits within 72 hours to a secondary teaching hospital in Taiwan. J Emerg Med. 2010;38:512–7. https://doi.org/10.1016/j.jemermed.2008.03.039.
Meldon SW, Mion LC, Palmer RM, et al. A brief risk-stratification tool to predict repeat emergency department visits and hospitalization in older patients discharged from the emergency department. Acad Emerg Med. 2003;10:224–32. https://doi.org/10.1111/j.1553-2712.2003.tb01996.x.
LaMantia MA, Platts-Mills TF, Biese K, et al. Predicting hospital admission and returns to the emergency department for elderly patients. Acad Emerg Med. 2010;17:252–9. https://doi.org/10.1111/j.1553-2712.2009.00675.x.
Robinson K, Lam B. Early emergency department representations. Emerg Med Australas. 2013;25:140–6. https://doi.org/10.1111/1742-6723-12048.
Imsuwan I. Characteristics of unscheduled emergency department return visit patients within 48 hours in Thammasat University Hospital. J Med Assoc Thai. 2011;94:S73–80.
Martin-Gill C, Reiser RC. Risk factors for 72-hour admission to the ED. Am J Emerg Med. 2004;22:448–53. https://doi.org/10.1016/j.ajem.2004.07.023.
Rowe BH, Villa-Roel C, Sivilotti M, et al. Relapse after emergency department discharge for acute asthma. Acad Emerg Med. 2008;15:709–17. https://doi.org/10.1111/j.1553-2712-2008.00176.x.
Yan JW, Gushulak KM, Columbus MP, et al. Risk factors for recurrent emergency department visits for hyperglycemia in patients with diabetes mellitus. Int J Emerg Med. 2017. https://doi.org/10.1186/s12245-017-0150-7.
Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA—AR). Br J Addiction. 1989;84:1353–7. https://doi.org/10.1111/j.1360-00443.1989.tb00737.x.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke DP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Inter Med. 2007;147:573–7. https://doi.org/10.7326/0003-4819-147-8-200710160-00010.
Kaji AH, Schriger D, Green S. Looking through the retrospectoscope: reducing bias in emergency medicine chart review studies. Ann Emerg Med. 2014;64:292–8. https://doi.org/10.1016/j.annemergmed.2014.03.025.
Bull LM, Lunt M, Martin GP, et al. Harnessing repeated measurements of predictor variables for clinical risk prediction: a review of existing methods. Diagn Progn Res. 2021;4:9. https://doi.org/10.1186/s41512-020-0078-z.AccessedJanuary31.
Moe J, Wang YE, Schull MJ, et al. Characterizing people with frequent emergency department visits and substance use: a retrospective cohort study of linked administrative data in Ontario, Alberta, and BC Canada. BMC Emerg Med. 2022;22:127. https://doi.org/10.1186/s12873-022-00673-x.
McCormack RP, Hoffman LF, Norman M, et al. Voices of homeless alcoholics who frequent Bellevue Hospital: a qualitative study. Ann Emerg Med. 2015;65:178–86. https://doi.org/10.1016/j.annemergmed.2014.05.025.
Hawk K, D’Onofrio G. Emergency department screening and interventions for substance use disorders. Addict Sci Clin Pract. 2018. https://doi.org/10.11186/s13722-018-0117.1.
D’Onofrio G, Fiellin DA, Pantalon MV, et al. A brief intervention reduces hazardous and harmful drinking in emergency department patients. Ann Emerg Med. 2012;60:181–92. https://doi.org/10.1016/j.annemergmed.2012.02.006.
Havard A, Shakeshaft A, Sanson-Fisher R. Systematic review and meta-analysis of strategies targeting alcohol problems in the emergency department: interventions reduce alcohol-related injuries. Addiction. 2008;103:368–76. https://doi.org/10.1111/j.1360-0443.2011.03418.x.
D’Onofrio G, Degutis LC. Integrating Project ASSERT: a screening, intervention, and referral to treatment program for unhealthy alcohol and drug use into an urban emergency department. Acad Emerg Med. 2010;17:903–11. https://doi.org/10.1111/j.1553-2712.2010.00824.x.
Corace K, Willows M, Schubert N, et al. Alcohol medical intervention clinic: a rapid access addiction medicine model reduces emergency department visits. J Addict Med. 2020;14:163–71. https://doi.org/10.1097/ADM.0000000000000559.
Funding
None.
Author information
Authors and Affiliations
Contributions
FS conceived the study and designed it with assistance from DL, GI, and BG. EG provided the initial dataset. FS, IS, SD, AY, and IC collected data. DB and AK adjudicated seizure patients. BG and EG reviewed patients with concurrent issues. DL performed Bayesian analysis. SB and AK provided content information from an addictions viewpoint. FS drafted the manuscript and all authors approved. FS takes overall responsibility.
Corresponding author
Ethics declarations
Conflict of interest
None.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Scheuermeyer, F.X., Lane, D., Grunau, B. et al. Risk factors associated with 1-week revisit among emergency department patients with alcohol withdrawal. Can J Emerg Med 25, 150–156 (2023). https://doi.org/10.1007/s43678-022-00414-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-022-00414-w