
Abstract
Study design
Retrospective case-series.
Objectives
To evaluate the outcomes of bracing in skeletally immature patients with moderate–severe idiopathic scoliosis (IS) curves ≥ 40°.
Background
In contrast to prior beliefs, the recent studies have reported successful outcomes with brace treatment may occur in some patients with moderate–severe scoliosis ≥ 40°. Despite other encouraging case-series, non-operative treatment is rarely attempted and the efficacy of bracing large curves remains uncertain.
Methods
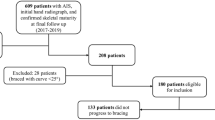
100 skeletally immature children (mean 11.8 ± 2.36 years; range 6.1–16.5) with IS ≥ 40° were identified. 80 were adolescent IS (80%) and 20 juvenile IS (20%). The Risser plus score was used to evaluate skeletal maturity. 66 children were Risser 0 (66%). SRS-SOSORT outcome guidelines were used: > 5° progression, stabilization between − 5° and 5° and, > 5° improvement.
Results
Mean initial Cobb was 45° ± 3.9° (range 40°–59°), with in-brace and % correction of 30° ± 8.7° (range 7°–48°) and 34 ± 17.5% (range 2–84%), respectively. 57 progressed (57%), 32 stabilized (32%), and 11 improved (11%) after a median of 1.8 years (IQR 1.2–2.9). Open triradiate cartilage at presentation (p = 0.005) and less in-brace correction (p = 0.009) were associated with progression. 58 children (58%) underwent surgery after a mean of 3.0 years (range 0.7–7.3). Surgical patients were younger (11.2 vs. 12.7 years; p = 0.003), more often Risser 0 (79% vs. 48%; p < 0.001); however, presented with similar curves (45° vs. 44°; p = 0.31). Open triradiate cartilage at presentation (OR 15.3; 95% CI 4.3–54.6; p < 0.001) and less in-brace correction (p = 0.03) increased the likelihood of surgery. All 20 JIS patients avoided temporary growth rods, with 18 (90%) eventually requiring surgery.
Conclusion
Non-operative treatment was successful in 42% of children. Risk factors for surgery were younger age, open triradiates, and less in-brace correction. Bracing can be effective in delaying surgery until skeletal maturity in patients with curves ≥ 40°. Patients should be counseled on the risks and benefits of bracing and surgery.
Level of evidence
Level IV.


Similar content being viewed by others

References
Asher MA, Burton DC (2006) Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis 1:2. https://doi.org/10.1186/1748-7161-1-2
Danielsson AJ (2013) Natural history of adolescent idiopathic scoliosis: a tool for guidance in decision of surgery of curves above 50 degrees. J Child Orthop 7:37–41. https://doi.org/10.1007/s11832-012-0462-7
Weinstein SL, Dolan LA, Wright JG, Dobbs MB (2013) Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 369:1512–1521. https://doi.org/10.1056/NEJMoa1307337
Maruyama T, Kitagawa T, Takeshita K, Mochizuki K, Nakamura K (2003) Conservative treatment for adolescent idiopathic scoliosis: can it reduce the incidence of surgical treatment? Pediatr Rehabil 6:215–219. https://doi.org/10.1080/13638490310001642748
Negrini S, Aulisa AG, Aulisa L, Circo AB, de Mauroy JC, Durmala J, Grivas TB, Knott P, Kotwicki T, Maruyama T, Minozzi S, O’Brien JP, Papadopoulos D, Rigo M, Rivard CH, Romano M, Wynne JH, Villagrasa M, Weiss HR, Zaina F (2012) 2011 SOSORT guidelines: orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 7:3. https://doi.org/10.1186/1748-7161-7-3
Carreon LY, Puno RM, Lenke LG, Richards BS, Sucato DJ, Emans JB, Erickson MA (2007) Non-neurologic complications following surgery for adolescent idiopathic scoliosis. J Bone Joint Surg Am 89:2427–2432. https://doi.org/10.2106/JBJS.F.00995
Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV (2003) Health and function of patients with untreated idiopathic scoliosis: a 50−year natural history study. JAMA 289:559–567
Dolan LA, Weinstein SL (2007) Surgical rates after observation and bracing for adolescent idiopathic scoliosis: an evidence-based review. Spine (Phila Pa 1976) 32:S91–S100. https://doi.org/10.1097/brs.0b013e318134ead9
Upasani VV, Hedequist DJ, Hresko MT, Karlin LI, Emans JB, Glotzbecker MP (2015) Spinal deformity progression after posterior segmental instrumentation and fusion for idiopathic scoliosis. J Child Orthop 9:29–37. https://doi.org/10.1007/s11832-015-0632-5
Emans JB, Kaelin A, Bancel P, Hall JE, Miller ME (1986) The Boston bracing system for idiopathic scoliosis. Follow-up results in 295 patients. Spine (Phila Pa 1976) 11:792–801
Vijvermans V, Fabry G, Nijs J (2004) Factors determining the final outcome of treatment of idiopathic scoliosis with the Boston brace: a longitudinal study. J Pediatr Orthop B 13:143–149
Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O’Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F (2018) 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord 13:3. https://doi.org/10.1186/s13013-017-0145-8
Richards BS, Bernstein RM, D’Amato CR, Thompson GH (2005) Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine (Phila Pa 1976) 30:2068–2075 (discussion 2076–2067)
Aulisa AG, Guzzanti V, Marzetti E, Giordano M, Falciglia F, Aulisa L (2014) Brace treatment in juvenile idiopathic scoliosis: a prospective study in accordance with the SRS criteria for bracing studies—SOSORT award 2013 winner. Scoliosis 9:3. https://doi.org/10.1186/1748-7161-9-3
Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB, Gardner-Bonneau D (1997) A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am 79:664–674. https://doi.org/10.2106/00004623-199705000-00005
Aulisa AG, Guzzanti V, Falciglia F, Giordano M, Galli M, Aulisa L (2019) Brace treatment of Idiopathic Scoliosis is effective for a curve over 40 degrees, but is the evaluation of Cobb angle the only parameter for the indication of treatment? Eur J Phys Rehabil Med 55:231–240. https://doi.org/10.23736/S1973-9087.18.04782-2
Lusini M, Donzelli S, Minnella S, Zaina F, Negrini S (2014) Brace treatment is effective in idiopathic scoliosis over 45 degrees: an observational prospective cohort controlled study. Spine J 14:1951–1956. https://doi.org/10.1016/j.spinee.2013.11.040
Negrini S, Negrini F, Fusco C, Zaina F (2011) Idiopathic scoliosis patients with curves more than 45 Cobb degrees refusing surgery can be effectively treated through bracing with curve improvements. Spine J 11:369–380. https://doi.org/10.1016/j.spinee.2010.12.001
Bettany-Saltikov J, Weiss HR, Chockalingam N, Taranu R, Srinivas S, Hogg J, Whittaker V, Kalyan RV, Arnell T (2015) Surgical versus non-surgical interventions in people with adolescent idiopathic scoliosis. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.cd010663.pub2
Katz DE, Durrani AA (2001) Factors that influence outcome in bracing large curves in patients with adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 26:2354–2361
Xu L, Yang X, Wang Y, Wu Z, Xia C, Qiu Y, Zhu Z (2019) Brace treatment in adolescent idiopathic scoliosis patients with curve between 40 degrees and 45 degrees: effectiveness and related factors. World Neurosurg. https://doi.org/10.1016/j.wneu.2019.03.008
de Mauroy J, Weiss H, Aulisa A, Aulisa L, Brox J, Durmala J, Fusco C, Grivas T, Hermus J, Kotwicki T, Le Blay G, Lebel A, Marcotte L, Negrini S, Neuhaus L, Neuhaus T, Pizzetti P, Revzina L, Torres B, Van Loon P, Vasiliadis E, Villagrasa M, Werkman M, Wernicka M, Wong M, Zaina F (2010) 7th SOSORT consensus paper: conservative treatment of idiopathic & Scheuermann’s kyphosis. Scoliosis 5:9. https://doi.org/10.1186/1748-7161-5-9
Troy MJ, Miller PE, Price N, Talwalkar V, Zaina F, Donzelli S, Negrini S, Hresko MT (2019) The “Risser + ” grade: a new grading system to classify skeletal maturity in idiopathic scoliosis. Eur Spine J 28:559–566. https://doi.org/10.1007/s00586-018-5821-8
De Mauroy JC (2013) Prospective study of 136 adolescent scoliosis of more than 40° treated with the Lyon brace. Scoliosis 8:O34. https://doi.org/10.1186/1748-7161-8-S1-O34
Aulisa AG, Guzzanti V, Giordano M, Falciglia F, Fuiano M, Aulisa L (2014) Conservative treatment in adolescent idiopathic scoliosis with curves over 45°: is the measurement in Cobb degrees the only parameter to be considered? Scoliosis 9:O23. https://doi.org/10.1186/1748-7161-9-S1-O23
Funding
No funding, grants, or financial compensation was received for this study.
Author information
Authors and Affiliations
Contributions
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work: BPV, ATW, MPG, PEM, LIK, DJH, JBE, MTH. Drafting the work or revising it critically for important intellectual content: BPV, ATW, MPG, PEM, LIK, DJH, JBE, MTH. Final approval of the version to be published: BPV, ATW, MPG, PEM, LIK, DJH, JBE, MTH.
Corresponding author
Ethics declarations
Institutional review board
Approval was gained for this study (IRB00013498).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Verhofste, B.P., Whitaker, A.T., Glotzbecker, M.P. et al. Efficacy of bracing in skeletally immature patients with moderate–severe idiopathic scoliosis curves between 40° and 60°. Spine Deform 8, 911–920 (2020). https://doi.org/10.1007/s43390-020-00131-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-020-00131-3