
Abstract
The SARS-CoV-2 infections continue unabated in Ghana and globally. The identification of country dynamics of the virus, its spread, and country-specific interventions in tackling the menace including the application of geospatial technologies. This research sought to highlight the use of geospatial technologies in the fight against COVID-19 in Ghana with best practices from China where the infections originated from; present the trends in Ghana and model near future trends of the virus. It was evident that just as other places, Ghana has employed geospatial technologies and continues to ply unchartered paths in solutions. The trend in Ghana is in line with a population concentration and tends to record higher figures in the southern parts. It is modeled that through incessant mobility patterns, infections will spread through to the middle parts and then the northern parts. The research, therefore, recommends the use of infrared scanners to augment testing practices and enhanced tracing of infected persons as well as the use of drones for the distribution of essential services.
Similar content being viewed by others

Introduction
Later part of 2019 saw the development of one of the world pandemics, COVID 19. The infection believed to have originated from a laboratory in the city of Wuhan in December 2019 (Wu et al. 2020; Shereen et al. 2020). A pathogen later identified as a novel beta-coronavirus (2019-nCoV) which was later renamed as SARS-CoV-2) affected thousands of people in China (provinces—Guangdong, Hubei, Henan, Zhejiang,among other towns and cities—Shanghai and Beijing) and traveled rampantly among other countries like Japan, Thailand, Germany, Republic of Korea, United States, Viet Nam, and Singapore. Although coronaviruses are not new (Sun et al. 2020), a comparison of situations surrounding SARS-CoV-2 and SARS-CoV of 2002/2003 and even MERS-CoV (Middle East Respiratory Syndrome-related coronavirus) of 2012/2014 indicates that the COVID-19 spread extraordinarily faster than expected(Gao et al. 2020). Indicatively, COVID-19 affected 1000 people in just 48 days as against times taken to affect the same figure by MERS (two and half years) and SARS (4 months) (Kamel Boulos and Geraghty 2020). Consequently, the outbreak of new SARS-CoV-2 coronavirus was declared by World Health Organization as constituting a Public Health Emergency of International Concern (PHEIC) on January 30, 2020 (Sohrabi et al. 2020; WHO 2020).
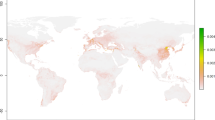
The rate of infection of COVID-19 is unprecedented and the world is on uncharted paths. The coronavirus world meter (https://www.worldometers.info/coronavirus/), as of May 20, 2020, 10:02 GMT, reported that confirmed cases stood at 5,003,500 with total global deaths and recoveries standing at 325,223 and 1,971,709 respectively. Active cases stood at 2,706,568 with, 98% and 2% being in mild and serious/critical conditions. Globally, it is the Americas that have been presently greatly affected (Fig. 1). Africa has had its share of the global pandemic though the rate of infection is believed to be slower than other regions (World Health Organization 2020). Nonetheless, Africa, as at 20/05/2020, 07:00 GMT, had recorded 90,943 cumulated cases (1.82% global share), 2885 deaths (0.89% global share) and 35, 257 recoveries (1.79% global share). More than half of the countries in Africa had been hit by the COVID-19, with South Africa being the most affected with 17,200 cases (The Economist 2020).

Regional Comparison of confirmed cases, rounded percentages based on WHO Coronavirus Disease (COVID-19) Dashboard. Accesses on 20/05/2020 08:10 GMT. https://covid19.who.int/?gclid=CjwKCAjwqpP2BRBTEiwAfpiD-8QcJb8DvFKF-Dv6CVodSoewRZ-nRlce-3ENCVpekI3zuFWJlSWOmhoCnSAQAvD_BwE
Since it recorded its first COVID-19 case on 12 March 2020 (UNDP Ghana 2020a, b), Ghana has seen a rise in confirmed cases from the country’s capital, Accra, and spread on wings of mobility to almost all parts of the country. Protocols such as the washing of hands, observing social/physical distancing, personal hygiene, and personal protective equipment have been subscribed to by the government and health services which, have been mainly observed by the general populace. With the incessant increase in the recorded cases, current and modeling of future trends are indispensable in understanding the concentration and the spread of the infection.
Application of GIS and Remote Sensing in Fighting COVID-19
The application of Geographic Information Systems and Remote Sensing in tracking and combating contagion has been long-standing in literature since the early days of 1694. Although it was done through conventional mapping, the phenomenon was applied in Italy for plague containment. Throughout the times to around 1918 various mapping methods were applied to track and understand the spread of many infectious diseases including cholera, fever, and even the 1981 influenza pandemic. Computerization of systems for geographic information in the 1960s contributed to the possibilities to analyze, visualize and detect patterns of diseases which have heightened its usage such that out of 865 papers published in health GIS literature, 248 (28.7%) focused on mapping infectious diseases in a review conducted in 2014 (Lyseen et al. 2014). Since then, applied health geography, through web-based tools, has seen many revolutions (Boulos et al. 2010; Gong et al. 2015; Tanser 2000). In recent times, the quest to protect lives in epidemic times necessitates the ingestion of data from sources into such tools and the display of results in interactive and real or near real-time dashboards, which have become very useful means by which many governments display spatial specific information on the COVID-19.
Kamel Boulos and Geraghty (2020) revealed that China, as of 22 January 2020, relied on a dashboard developed by the Johns Hopkins University’s Center for Systems Science and Engineering (JHU CSSE) based on Esri ArcGIS Online services and generated over 160 million views. This indicates people’s interest in tracking health threats which came quite handy for persons with internet access to have unfettered access to tremendous information about the COVID-19. Subsequently, China adopted a device to support informed personal decisions about seeking medical treatment and self-quarantine. It was named close contact detector’s platform/app co-launched by China Electronics Technology Group Corporation and China’s National Health Commission. This app coupled with WorldPop analyses aided in the mapping of mobility patterns and tracking of infected cases or pandemics, hence, giving credence to how powerful spatial analysis methods are in modeling the spread of disease, pattern detection, delineating and hotspots and determination of possible future occurrences (Gardner 2020). China has made various GIS and Remote sensing applications in the fight against COVID-19 (Kamel Boulos and Geraghty 2020). Notable among them is the use of drones for critical medical supplies (Huber 2020), detection of outbreak source (Yu et al. 2020), disinfection (Brickwood 2020), and selection of appropriate sites for construction of health facilities (BBC News 2020b).
Ghana, just like other African countries (e.g., Nigeria), has implemented various GIS and remote sensing methods to track, understand, and monitor COVID 19 cases. These measures and tools include dashboards, mobile app, and drones. First of all, Ghana has used dashboards to present information and to show the trends of COVID-19 in Ghana. Although there are many dashboards developed for the same purpose, two of these dashboards are paramount, and the other developers depend on these dashboards for data and figures based on which theirs is developed. These dashboards are that of the Ghana Statistical Service and the Ghana Health Service. The Ghana Statistical Service dashboard, indicated as the “Ghana COVID 19 Monitoring Dashboard” is made up of basically five panes. The Cases pane presents data on the cumulative case count, the map pane indicating the spatial distribution of the cases on a map, the Trend pane which presents trend analyses of cases (cumulated, active, recovered, and death), the News pane provides explanatory information of the cases reported and the Health pane with information of health spot in the country (Fig. 2).

Ghana COVID-19 Dashboard showing COVID 19 information within different panes. Accessed 20/05/2020, 8:10 GMT. https://statsghana.maps.arcgis.com/apps/opsdashboard/index.html#/aacf5ceb5ccc493f879b9fba19fe898e
The second dashboard is that of the Ghana Health Service. The dashboard, powered by Sanbus Geospatial Limited, has four parts. The first part gives a regional breakdown of confirmed cases. The second part presents the aggregated figures for confirmed, recoveries, and death cases at the time of publication. The third part presents the spatial distribution of the confirmed cases on a choropleth map with data symbolized per category and given in proportional circles indicating the intensity of the phenomenon per each region. The fourth part gives information on COVID-19 segregated into gender distribution (Fig. 3).

COVID-19 dashboard of Ghana Health Service. Accessed on 20/05/2020, 08:10 GMT. https://ghanahealthservice.org/covid19/
From the two dashboards, it can be teased out that, Ghana’s case of COVID-19 stood at 6096 persons with 1773 recoveries and 31 deaths. The confirmed cases consist of 61% of males and 39%. The gender disparity is in line with happenings globally and corroborates studies are done, suggesting that men are susceptible to COVID-19 pandemics (Ducharme 2020; Jin et al. 2020).
Mobile App
On the 13th of April, through the Ministry of Communication, Ghana launched a mobile app called GH COVID 19 Tracker (BBC News 2020a). According to the Ministry, the free to download mobile app intended to provide assistance and to varyingly augment the state’s efforts to identify and trace persons who have come into contact with infected persons (Ministry of Communications 2020). It offered a platform for a personal assessment of conditions and gives results that influence decisions to seek medical care should the person be at a higher risk. The app was fashioned to aid early detection of the infection and had GPS fitted into it to track movement and cases(Yakubu 2020).
Drone
Drone technology and its remote sensing abilities make it useful in the areas of limited human interactions, appropriateness, and less time consuming (Huber 2020). Drone technology has been adopted as part of measures Ghana has put in place in the COVID-19 fight. Knott (2020) reports that, Ghana was the first country in West Africa to use Drone technology in the fight against the pandemic. Aside from Drone's use for disinfection exercises at public places and institutions, the technology has been leveraged for rapid transport of critical items, personal protective equipment, and even the transportation of COVID-19 samples to the testing centers (Nunoo 2020; REUTERS 2020). This has aided in the rapid testing of cases, tracing, and management of the situation and among the four top countries that have done more tests per population in Africa (Myjoyonline.com 2020).
Although the use of Geospatial Technologies and measures has resulted in many good outcomes, more spatial analyses can be put in place to present the COVID-19 pandemic spatially, hence indicating its distribution in the determination of future outcomes. This is the focus of the research.
Data Source and Methods
Data used for this study are population and COVID-19 data of Ghana. Population statistics Population data, synthesized into Regions, was derived from Ghana Statistical Service (GSS) as of 2019 c. Regional outlines in shapefile were extracted Land-Use Planning and Management Information System of Land Use and Spatial Planning Authority. COVID-19 data was added to the regional boundaries (in Universal Traverse Mercator Zone 30 N) with the join table algorithm. COVID-19 data presented and used for this paper was derived from many sources, including Ghana Health Service, Ghana Statistical Service, and the World Health Organization dashboards. This was to establish the consistencies in the data used.
Geospatial Technologies presents varying means by which phenomenon is interpolated and presented for better understanding (Bagyaraj et al. 2020; Balamurugan et al. 2020; Shankar and Kawo 2019). Its application is in various fields and many human endeavors. Although many interpolation options exist, in forecasting the possible trends in Ghana situation, the Universal Kriging (linear with Quadratic drift semivariogram model) and Inverse Distance Weighted (IDW) interpolation algorithm were used. Childs (2004) and Kawo and shankar (2018) reveals that Kriging applies statistical interpolation, which makes it a powerful and effective option for diverse applications, including pollution modeling, geochemistry, and health. It works with the assumption that the direction and distance between sample points reflect spatial correlation, which is useful in the explanation of variation in the surface (Shankar et al. 2011).
There is a derivation of predictive values from the measure of relationships in samples using sophisticated weighted average techniques. Using the Universal Kriging (linear with Quadratic drift semivariogram model) enables the modeling of trends in data. The only possible shortfall with the use of Kriging models is that point values are not specifically considered which will plausibly cause interpolated values to be lower or higher than real values. On the other hand, the Inverse Distance Weighted interpolation algorithm assumes that for each input point, there exists a local influence that diminishes with distance. Inferable, this method is applicable when there is an assumption that the data been modeled or phenomenon being studied and mapped decreases in influence as the distance from the core increases. Specifically to the COVID-19, although inconclusive, many writers (e.g., Loayza 2020) have identified a possible association of its spread to population densities and distribution. These characteristics identified the two interpolation techniques hence, make them appropriate for health modeling and its use in modeling COVID-19 trends in Ghana.
Results and Discussions
The following sections present a picture of the pandemic situation in Ghana, which has placed the debate on COVID-19 within the context of the global and regional outlook, as well as data sources and methods. The ensuing section seeks to present three basic things; thus, the geographical context, current situation, and infection patterns and modeling of future occurrences and spatial dynamics.
Geographic Context
This study was carried out in Ghana. Ghana is part of the Africa Continent (West Africa) and has a land area of 238,540 sq. Kilometers (Condit et al. 2014). Ghana is surrounded by Togo, Burkina Faso, Ivory Coast, and the Gulf of Guinea with a heterogeneous population of about 30 million as of 2019. There are 16 administrative regions in Ghana, with the capital town being Accra. Accra and Ashanti are the most populous regions due to the concentration of activities and infrastructure, while Kumasi and Accra enjoy urban primacy. Immigration issues are on the rise, given the porous nature of the borders, the bilateral arrangements with neighboring countries, and the liberalization of trade. As a result, there has been an over-concentration of people, especially in the southern part of the country, resulting in high density and higher occupancy rates. Due to this, Greater Accra and Ashanti are the most populous regions, with two big cities (Kumasi and Accra) enjoying urban primacy (Fig. 4).

Contextual map of Ghana
COVID-19 in Ghana
Since Ghana recorded its first case in early March, the rate and tempo of infection and transmission have been varying and moderate as compared to the global trend. In the early times of mass testing, periods between the first recorded case to 31st of March saw the number of infected cases rising from 21 to 161 (about 666.7% increase). Subsequently, the rate of release of information on infection affects the rate of infection. Based on that, the rate has been erratic as, Table 1 reveals. Nonetheless, the aggregate infection rate per the number of tests (general surveillance, enhanced contact tracing, and quarantined cases at Tamale and Accra) carried out from March to May 2020 totaling 186,948 persons, was 3.34% (Ghana Statistical Service 2020). Comparing Ghana’s population and confirmed cases, it can be deduced that, 0.021% of the Ghana’s population has been affected by the COVID-19.
COVID-19 induced deaths in Ghana and rate is very low as compared to other regions. From 11th March to 20th May 2020, Ghana had recorded 31 deaths attributed to COVID-19. The rate of increase for cases has been varying over the period and it is based on the release of information on infection by the appropriate ministries. Nonetheless, the aggregate deaths are about 0.5% of the reported cases, which is far less than that of China (5.49%), USA (6.01%), and the globe, which stands at 6.64%. This in a wider array corroborates the mild impact of COVID-19 in Africa. as asserted by some studies (The Economist 2020). Explanatorily, recorded cases were as a result of underlying health and comorbidity conditions (such as hypertension, anemia, tuberculosis, diabetes mellitus, etc.) with about 10% being a person without any underlying health conditions. A major proportion is aged with few accounts of younger age as low as 9 years and the highest being 81 years (Ghana Health Service 2020). Recoveries increase astronomically hovering around 1898 persons as of 20th May.
Geographically, the spread of the pandemic in Ghana has spatial connotations. From the Table 2 two major urban areas, Kumasi and Accra, and by far, Ashanti and Greater Accra Regions, have greatly affected and recorded higher figures. Ashanti and Greater Accra regions have accumulated 88.94% (Greater Accra—74.41%, Ashanti—14.53%) of the reported cases The third highest hit region makes up just 4.23% of the confirmed cases. Comparing population distribution and COVID-19 cases (Fig. 5), there is seemingly a link in infection trends and the regional level of Ghana's population distribution.. Ghana is populous in the southern part of the Country owing to the trend of development. On aggregate, areas such as Greater Accra, Ashanti, and Northern regions are the most populous. Also, Western, Central, Eastern, Volta, and the upper east are second-most populous regions. These are followed by Ahafo, Oti, and Upper West regions. The least populous regions are Bono East, Savannah, and North East.

COVID-19 cases reveal a similar trend. It can be deduced from Fig. 5, that the impact of the infection is felt at populous areas in the Country. At a glance, the Greater Accra and Ashanti region has recorded many cases, which have transcended to the Central and Eastern Regions. Again, relatively fewer cases have been recorded in the other regions except for Bono East, Ahafo, and Savannah regions with no cases as of 20th May 2020. The situation and trends of infection can be associated with high dense, intense market activities and population concertation in these areas which makes observing social/physical distancing and other health protocols problematic. At large, corroborates the findings of many studies with evidence from China ( see Barr and Tassier 2020; Fang and Wahba 2020; Florida 2020) such that population concentration areas contribute to the spread and intensity of COVID-19.
Future Trend of COVID-19 in Ghana
Prediction of possible trends and outcomes is indispensable for planning and to influence policy direction. Therefore, the research seeks to use geospatial technology as a tool to predict possible spatial spread based on available data. The modeling was based on current COVID-19 cases, population dynamics, mobility dynamics, and the attack rate. It is envisaged that Greater Accra and Ashanti Regions with higher attack rates will record higher numbers as compared to the other regions, all things being equal.
As indicated in the previous section, the over 30 million population of Ghana is not evenly distributed. The distribution seen spatially to be clumped rather than random and influenced by migration issues, causing population concentration and higher densities in the southern part. The concentration will lead to further infections and transmission in the populous regions and be transmitted to other abutted regions (Table 3).
Available data collected by Vodafone Ghana (based on origin–destination matrix -ODM) on mobility patterns in Ghana portrayed a relatively low movement of people between regions (Fig. 6). Data collected from April to May 2020 based on anonymized, aggregated data structure and produced by the count of subscribers’ trips between any two localities indicated a negative trend implying a reduction in trips made during this period. The duration of data collected spanned from before COVID-19 induced restriction was imposed in Ghana, during the imposition and some few moments after the imposition. Although these are data on movement, it is invariably associated with the possible movement of infected persons and inter-regional and community spread. Vodafone subscribers constitute about 19% of telecommunication users in Ghana as of 2019 (Kuuire 2019). The data was used based on its availability and the assumption that mobility patterns will not differ for other telecommunication networks in Ghana, hence, it will not affect the outcome of the modeling.

As indicated by Fig. 7 areas, travelers from Accra (Greater Accra region), the first order and populous region disproportionately moved to central and eastern region. These are followed by regions such as Ashanti, Upper West, and Western Regions. Relatively, lesser trips and movements were recorded in the Savannah, Oti, and Northern Regions.

The trend for the Ashanti region presents a no different scenario. People’s movement was relatively low in the lockdown moment and during the lockdown but relatively increased times after the lockdown. There was a comparatively fair distribution of movement from the Ashanti Region to other regions. Indicatively, from Fig. 8, the majority of trips were made to the Greater Accra and Central Regions after the lockdown. These are followed by Bono East, Eastern, and Ahafo Regions. Regions recording the least movement of people after the lockdown included Volta, Savannah, and Northern Regions. Overall, aggregate data on mobility (Fig. 9) shows a concentrated movement in the southern part of the country with intensity spreading to the other regions. The trend will be influenced by migration issues to and from the infected regions.

Proportion of travelers from Ashanti that travel to each Region

From the above-mentioned, the trend of the infections can be modeled in Ghana. From Fig. 10, the Inverse Distance Weighted interpolation reveals a much concentration of cases in the southern part of Ghana. Greater Accra and Ashanti Regions remain hot spots for the COVID-19 Cases, which will gradually extend to Eastern, Central, and Volta Regions as well as the upper part of the country. Additionally, a modeled trend with the Universal Kriging Interpolation reveals future occurrences in the COVID-19 cases of Ghana categorized into mainly into five. These are the highest risk areas, higher risk, high risk, low risk, and lower risk areas. Greater Accra, Volta, Central, Eastern regions, and some part of Western region lies in the highest risk zone. The higher risk areas comprise Oti, Ashanti, Western, and some part of Bono East regions. Also, the high-risk areas include Western North, Bono, Ahafo, Bono East, and some parts of Northern Regions. Savannah and Northern regions constitute the low-risk areas with the lower risk areas being North East, Upper West, and Upper East regions.

Future trends in COVID-19 cases on Ghana
Conclusion and Recommendations
The study was set to tackle three primary objectives, thus, highlighting the application of geospatial technologies in the fight against COVID-19, present data and trends, and modeling of the possible future trend in the COVID-19 cases in Ghana. The study revealed that geospatial technologies are applicable in the fight against the global pandemic. Many GIS and Remote Sensing tools have been used in various endeavors, all of which contribute to efforts put in place to tackle the pandemic. Moving from manually tracking cases, many countries, including Ghana, have resulted in the use of dashboards, tracker apps, and uncrewed aerial vehicles to distribute personal protective equipment (PPEs) and to enhance testing and trace and treatment of the COVID-19.Since Ghana recorded its first case in March, the trend and rate of infection have been moderate as compared to other African countries. The distribution of cases per region is disproportional. The Greater Accra region constitutes about 75% share of the reported cases, with the Ashanti Region being second with about 15%. The rest of the Regions have varying percentages of reported cases with Savannah, Bono East, and Ahafo regions not recording any case as of 21st May 2020. The trend of infection has been likened to population concentration corroborating the assertion made by many writers.
The tempo and trend of COVID-19 were modeled using Universal Kriging and Inverse Distance Weighted Interpolation algorithms. The modeling was based on mobility dynamics, current COVID-19 cases, population dynamics, and the rate of SARS-CoV2 infection in Ghana. It was revealed that the COVID-19 situation will be concentrated in the southern part of Ghana and will extend from Greater Accra and Ashanti regions to Eastern, Western, Central, and Volta regions. Through issues of mobility patterns, the infections will extend to the middle belt of Ghana then gradually to the Northern part of the Country. This finding is very instrumental and forms the basis for the allocation of resources to affected areas and devising of containment measures to reduce the rate of spread to the yet to be affected regions and possibly prevent spread.
Based on the aforementioned, the study advocates of continuous and innovative use of Geospatial technologies in the fight against COVID-19. Additional to the app and drones currently being used, the Country can consider the use of infrared scanners of quick detection of infected persons in motion and even contact tracing. Security agencies maintaining order in the communities can have these scanners as part of their gears or worn like spectacles. These can be done amidst the observance of the health protocols and adequate physical/social distancing to prevent infections from asymptomatic patients. Detection of COVID-19 cases early will enable prompt treatment, hence, averting fatalities. Secondly, there should be readily available data in varying forms for further geospatial analyses to inform policy formulation and interventions.
References
Barr J, Tassier T (2020) Are crowded cities the reason for the COVID-19 pandemic?. Scientific American Blog Network. https://blogs.scientificamerican.com/observations/are-crowded-cities-the-reason-for-the-covid-19-pandemic/. Accessed 31 May 2020
Balamurugan P, Kumar PS, Shankar K (2020) Dataset on the suitability of groundwater for drinking and irrigation purposes in the Sarabanga River region, Tamil Nadu, India. Data Brief 29:105255. https://doi.org/10.1016/j.dib.2020.105255
Bagyaraj M, Shankar K, Alemayehu T, Muthukumarasamy R, Gnanachandrasamy G (2020) Distribution and trend analysis of COVID-19 in India: geospatial approach. J Geogr Stud 4(1):1–9. https://doi.org/10.21523/gcj5.20040101
BBC News (2020a) Coronavirus: Ghana govment COVID-19 tracker mobile app be solid tech intervention or needless app?—BBC News Pidgin. https://www.bbc.com/pidgin/tori-52267513. Accessed 19 May 2020
BBC News (2020b) Coronavirus:10 days of hospital building in 60 seconds—BBC News. Coronavirus:10 days of hospital building in 60 seconds. https://www.bbc.com/news/av/world-asia-china-51348297/coronavirus10-days-of-hospital-building-in-60-seconds. Accessed 19 May 2020
Boulos M, Warren J, Gong J, Yue P (2010) Web GIS in practice VIII: HTML5 and the canvas element for interactive online mapping. Int J Health Geogr 9(1):14. https://doi.org/10.1186/1476-072X-9-14
Brickwood B (2020) XAG introduces drone disinfection operation to fight coronavirus outbreak. XAG introduces drone disinfection operation to fight coronavirus outbreak. https://www.healtheuropa.eu/xag-introduces-drone-disinfection-operation-to-fight-the-coronavirus-outbreak/97265/. Accessed 19 May 2020
Childs C (2004) Interpolating Surfaces in ArcGIS Spatial Analyst. ESRI. www.esri.com. Accessed 20 May 2020
Condit R, Sukumar R, Hubbell SP, Foster RB, Helm CV, Witkowski ETFF, Cousins SR, Witkowski ETFF, Pfab MF, Duvall CS, Duvall CS, Torello-raventos M, Feldpausch TR, Veenendaal E, Saiz G, Domingues TF, Djagbletey G, Kemp J, Marimon BS et al (2014) Animal movement in heterogeneous landscapes: an experiment with eleodes beetles in shortgrass prairie. S Afr J Bot 3(4):536–544. https://doi.org/10.4172/2155-6180.1000106
Ducharme J (2020) Why is COVID-19 striking men harder than women?|Time. https://time.com/5829202/covid-19-gender-differences/. Accessed 19 May 2020
Fang W, Wahba S (2020) Urban density is not an enemy in the coronavirus fight: evidence from China. Sustainable Cities. https://blogs.worldbank.org/sustainablecities/urban-density-not-enemy-coronavirus-fight-evidence-china. Accessed 31 May 2020
Florida R (2020) What we know about density and covid-19’s spread. CITYLAB. https://www.citylab.com/equity/2020/04/coronavirus-spread-map-city-urban-density-suburbs-rural-data/609394/. Accessed 21 May 2020
Gao J, Tian Z, Yang X (2020) Breakthrough: chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. BioSci Trends. https://doi.org/10.5582/BST.2020.01047
Gardner L (2020) Modeling the spreading risk of 2019-nCoV. Center for System Science and Engineering, Johns Hopkins University
Ghana Health Service (2020) COVID-19 Updates. COVID-19 dashboard. https://ghanahealthservice.org/covid19/archive.php. Accessed 21 May 2020
Ghana Statistical Service (2020) COVID-19 Updates|Ghana. https://ghanahealthservice.org/covid19/archive.php. Accessed 21 May 2020
Gong J, Geng J, Chen Z (2015) Real-time GIS data model and sensor web service platform for environmental data management. Int J Health Geogr 14(1):2. https://doi.org/10.1186/1476-072X-14-2
Huber M (2020) Drones enlisted to fight corona virus in China. General aviation news: aviation international news. https://www.ainonline.com/aviation-news/general-aviation/2020-02-07/drones-enlisted-fight-corona-virus-china. Accessed 19 May 2020
Jin J-M, Bai P, He W, Wu F, Liu X-F, Han D-M, Liu S, Yang J-K (2020) Gender differences in patients with covid-19: focus on severity and mortality. Front Public Health 8:152. https://doi.org/10.3389/fpubh.2020.00152
Kamel Boulos MN, Geraghty EM (2020) Geographical tracking and mapping of coronavirus disease COVID-19/severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: how 21st century GIS technologies are supporting the global fight against outbr. Int J Health Geogr. https://doi.org/10.1186/s12942-020-00202-8
Kawo NS, Shankar K (2018) Groundwater quality assessment using water quality index and GIS technique in Modjo River Basin, Central Ethiopia. J Afr Earth Sc 147:300–311. https://doi.org/10.1016/j.jafrearsci.2018.06.034
Knott S (2020) In Ghana, Drones Help Combat COVID-19. Voice of America—English. https://www.voanews.com/covid-19-pandemic/ghana-drones-help-combat-covid-19. Accessed 20 May 2020
Kuuire J-A (2019) Timeline: battle of the ghana telecommunication companies—Tech Nova. Tech Nova. https://technovagh.com/2019/01/07/timeline-battle-of-the-ghana-telecommunication-companies/. Accessed 18 June 2020
Loayza N (2020) Smart containment and mitigation measures to confront the COVID-19 pandemic: tailoring the pandemic response to the realities of developing countries. World Bank Blogs. https://blogs.worldbank.org/developmenttalk/smart-containment-and-mitigation-measures-confront-covid-19-pandemic-tailoring. Accessed 12 June 2020
Lyseen AK, Nøhr C, Sørensen EM, Gudes O, Geraghty EM, Shaw NT, Bivona-Tellez C (2014) A review and framework for categorizing current research and development in health related geographical information systems (GIS) studies. Yearb Med Inform 23(01):110–124. https://doi.org/10.15265/IY-2014-0008
Ministry of Communications (2020) Launch of GH COVID-19 Tracker APP and Virtual Concert. https://moc.gov.gh/launch-gh-covid-19-tracker-app-and-virtual-concert. Accessed 19 May 2020
Myjoyonline.com (2020) Akufo-Addo’s claim that Ghana leads Covid-19 testing in Africa is false.—French News Agency (AFP)—MyJoyOnline.Com. https://www.myjoyonline.com/news/national/akufo-addos-claim-that-ghana-leads-covid-19-testing-in-africa-is-false-french-news-agency-afp/. Accessed 20 May 2020
Nunoo F (2020) Coronavirus tips: How Ghana dey use drone technology fight Covid-19 pandemic—BBC News Pidgin. BBC News. https://www.bbc.com/pidgin/tori-52372336. Accessed 20 May 2020
REUTERS (2020) Ghana turns to drones to enable faster coronavirus testing—Reuters. https://www.reuters.com/article/us-health-coronavirus-ghana-drones/ghana-turns-to-drones-to-enable-faster-coronavirus-testing-idUSKBN2220H7. Accessed 20 May 2020
Shankar K, Aravindan S, Rajendran S (2011) Hydrogeochemistry of the paravanar river sub-basin, Cuddalore District, Tamilnadu India. E-J Chem 8(2):835–845. https://doi.org/10.1155/2011/107261
Shankar K, Kawo NS (2019) Groundwater quality assessment using geospatial techniques and WQI in North East of Adama Town, Oromia Region Ethiopia. Hydrospatial Anal 3(1):22–36. https://doi.org/10.21523/gcj3.19030103
Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R (2020) COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res. https://doi.org/10.1016/j.jare.2020.03.005
Sohrabi C, Alsafi Z, O’Neill N, Khan M, Kerwan A, Al-Jabir A, Iosifidis C, Agha R (2020) World health organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg 76:71–76. https://doi.org/10.1016/j.ijsu.2020.02.034
Sun P, Lu X, Xu C, Sun W, Pan B (2020) Understanding of COVID-19 based on current evidence. J Med Virol 92(6):548–551. https://doi.org/10.1002/jmv.25722
Tanser FC (2000) The application of geographical information systems to infectious diseases and health systems in Africa. Int J Health Geogr 2002 9:1–9. https://www.ij-healthgeographics.com/content/1/1/4. Accessed 20 May 2020
The Economist (2020) The smouldering pandemic—why covid-19 seems to spread more slowly in Africa|Middle East & Africa|The Economist. https://www.economist.com/middle-east-and-africa/2020/05/16/why-covid-19-seems-to-spread-more-slowly-in-africa. Accessed 20 May 2020
UNDP Ghana (2020) UNDP’s Programmatic Offer for COVID-19 response in Ghana. https://www.undp.org/content/dam/rba/docs/COVID-19-CO-Response/undp-rba-covid-ghana-apr2020.pdf
Vodafone Ghana (2020) Mobility analysis to support the Government of Ghana in responding to the COVID-19 outbreak Insights into the effect of mobility restrictions in Ghana using anonymised and aggregated mobile phone data Overview. https://statsghana.gov.gh/. Accessed 21 May 2020
WHO (2020) No Title. COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum. https://www.who.int/who-documents-detail/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum. Accessed 31 May 2020
World Health Organization (2020) African countries move from COVID-19 readiness to response as many confirm cases. Regional Office for Africa. https://www.afro.who.int/health-topics/coronavirus-covid-19. Accessed 20 May 2020
Wu Y-C, Chen C-S, Chan Y-J (2020) The outbreak of COVID-19. J Chin Med Assoc 83(3):217–220. https://doi.org/10.1097/JCMA.0000000000000270
Yakubu M (2020) Gov’t officially launches GH COVID-19 Tracker App. https://www.primenewsghana.com/general-news/gov-t-officially-launches-gh-covid-19-tracker-app.html. Accessed 19 May 2020
Yu W-B, Tang G-D, Zhang L, Corlett RT (2020) Decoding the evolution and transmissions of the novel pneumonia coronavirus (SARS-CoV-2/HCoV-19) using whole genomic data. Zool Res 41(3):247–257. https://doi.org/10.24272/j.issn.2095-8137.2020.022
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sarfo, A.K., Karuppannan, S. Application of Geospatial Technologies in the COVID-19 Fight of Ghana. Trans Indian Natl. Acad. Eng. 5, 193–204 (2020). https://doi.org/10.1007/s41403-020-00145-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41403-020-00145-3