
Abstract
Purpose of Review
To update the clinical value of a patient self-report multidimensional health assessment questionnaire (MDHAQ).
Recent Findings
The MDHAQ includes 10 individual quantitative scores for physical function, pain, patient global assessment, fatigue, sleep, anxiety, depression, morning stiffness, change in status, and exercise status, and 5 indices, RAPID3 (routine assessment of patient index data) to assess clinical status in all diseases studied, FAST3 (fibromyalgia assessment screening tool) and MDHAQ-Dep (depression) to screen for fibromyalgia and/or depression, RADAI self-report of specific painful joints and joint count, and a symptom checklist for review of systems, and recognition of flares and medication adverse events. The MDHAQ also uniquely queries traditional “medical” information concerning comorbidities, falls, trauma, new symptoms, illnesses, surgeries, hospitalizations, emergencies, medication changes, and medication side effects. Three MDHAQ versions include long for new patients, short for new and return patients, and telemedicine. An electronic MDHAQ (eMDHAQ) has been developed with software that can interface with any electronic medical record (EMR) through the HL7 FHIR standard. However, EMR collaboration and implementation have proven difficult.
Summary
An MDHAQ provides a quantitative overview of patient status with far more information and documentation than an interview, involving minimal extra work for the physician.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
A self-report multidimensional health assessment questionnaire (MDHAQ) (Figs. 1, 2, and 3) [1, 2] collects 10 individual quantitative scores for physical function, pain, global status, fatigue, anxiety, depression, sleep quality, morning stiffness, exercise status, and change in status; 5 indices for a RADAI (rheumatoid arthritis disease activity index self-report painful joint count), symptom checklist, clinical severity, fibromyalgia, and depression; and traditional “medical” history information, a unique feature among quantitative patient questionnaires, concerning illnesses, surgery, falls, medication changes, adverse events, etc.

Long MDHAQ


Short MDHAQ

Telemedicine MDHAQ
The MDHAQ was developed initially to assess and monitor rheumatoid arthritis (RA) but has been found informative to assess clinical status in patients with all rheumatic diseases studied [3, 4]. Development was performed in routine clinical care over 25 years as a continuous quality improvement (CQI) “plan-do-study-act“ program [5], with changes based on patient feedback, clinical relevance, and prognostic value [6], rather than initially according to psychometric criteria, although quantitative MDHAQ scores and indices meet psychometric criteria [1, 2, 6,7,8,9,10,10, 11••, 12,13,14,15, 16•, 17]. The MDHAQ provides more extensive information than a traditional interview in most patients, while saving 2–5 min for the physician and providing a more complete record.
Several versions of the MDHAQ have been developed for face-to-face and/or telemedicine encounters: a long MDHAQ for new patients, similar to a clinical “intake” questionnaire (Fig. 1), a short MDHAQ for new or return patients (Fig. 2), and a telemedicine MDHAQ, for remote completion as an attachment without protected health information (name, date of birth, medical record number), but requiring an identification number assigned by the treatment site (Fig. 3).
A secure, Health Insurance Portability and Accountability Act (HIPAA)-compliant digital electronic MDHAQ (eMDHAQ) has been developed, which incorporates HL 7 FHIR (Fast Healthcare Interoperability Resources) to interface with any electronic medical record (EMR). However, collaboration with EMR vendors has proven difficult, and independent MDHAQ databases have been found feasible and clinically informative. Further details concerning the MDHAQ are found in original reports and previous reviews [1, 2, 6,7,8,9,10,10, 11••, 12,13,14,15, 16•, 17].
Content of the MDHAQ as quantitative patient medical history scores
The MDHAQ includes scores for physical function, pain, and patient global assessment, the 3 patient self-report measures among the 7-item RA core data set [18] (Figs. 1, 2, 3). The physical function score is based on 10 activities, 8 verbatim from each of the 8 categories of 2 or 3 items on the standard HAQ reported in 1980 [19], and 2 “advanced” activities to “walk 2 miles or 3 kilometers” and “participate in recreational activities and sports as you wish” [1, 2]. The 10 activities are each scored 0–3, for a total of 0–30, which is divided by 3 for an adjusted total of 0–10, using a template on a paper MDHAQ (Figs. 1, 2, and 3).
Three “psychological” items for sleep quality, anxiety, and depression are queried in the patient-friendly HAQ format, scored 0–3.3 for a total of 0–9.9 as a “psychological index” [1, 2], which has not been widely adopted and is not included among the 5 MDHAQ indices in this review. It has been reported recently that the depression query can contribute to a screening index (see below) [16•].
Pain and patient global assessment are assessed according to 0–10 visual numeric scales (VNS), with 21 circles numbered at intervals of 0.5, rather than a traditional visual analog scale (VAS) line from 0 to 10 or 0–100. Advantages of the VNS include patient preference, ease of scoring by professionals, and absence of a need for an exact 10 cm line when printing or photocopying [20]. A 0–10, 21 circle fatigue VNS similar to the pain and global VNS is found on the MDHAQ (but not on the HAQ) [21]. Queries concerning morning stiffness [22], change in status, and exercise status [23, 24•, 25] may contribute to clinical decisions in many patients but are not included in the telemedicine MDHAQ (Fig. 3).
The MDHAQ is unique among quantitative patient questionnaires in querying traditional “medical” history information concerning recent surgeries, illnesses, medical emergencies, falls, hospitalization, new symptoms, medication changes and side effects, and changes in work duties or physician [6, 8, 26] (Figs. 1–3).
A long 2-page (four-sided) “new patient” MDHAQ queries a “past medical history,” similar to clinical “intake” questionnaires to record past illnesses, surgeries, family history, allergies, social history, and medications (Fig. 1). Patient self-report has been used for many decades [27] to collect a “subjective” medical history [28], which is entered by the physician into an encounter note, but without quantitative scores or indices. By contrast, most quantitative assessments of function, pain, fatigue, and other constructs by an observer or self-report, including the HAQ [19], Short-Form 36 (SF-36) [29], and PROMIS [30], do not query traditional “medical” history information [29, 30] (Table 1). The MDHAQ queries both traditional “medical” information and more recently developed quantitative self-report scores.
Patient questionnaire scores are quantitative, protocol-driven, reproducible components of a patient medical history, which meet the criteria of the “scientific method” [14, 31]. Patient self-report scores are as reproducible as formal joint counts or serology laboratory tests [7] and are correlated significantly with these measures [32]. Self-report patient questionnaire scores are more significant than traditional joint count or laboratory measures to distinguish active from control treatments in RA clinical trials [33]. Physical function scores are more significant than laboratory tests or radiographs to predict severe long-term outcomes of RA such as work disability, costs, joint replacement surgery, and premature death [24•, 34,35,36,37,38,39,40,41,42].
Five MDHAQ indices: RAPID3 (routine assessment of patient index data) to assess clinical status, FAST3 (fibromyalgia assessment screening tool), MDHAQ-Dep (depression), RADAI self-report painful joint count, and symptom checklist for review of systems, early recognition of disease flares and comorbidities, and adverse events of medications
MDHAQ scores may be compiled into 5 indices (Fig. 4), all based on individual measures within a 2-page MDHAQ:
-
1.
RAPID3 (routine assessment of patient index data) includes physical function, pain, and patient global assessment, each scored 0–10 for a total of 0–30 [43, 44•]. Early reports indicated scoring of 0–10 for RAPID3 [45, 46]. These reports presented studies to compare RAPID3 to “RAPID4” and “RAPID5,” which also included a patient self-report or physician-performed joint count and/or physician global assessment. Since indices under study included different numbers of measures, division by the number of measures was performed to give similar 0–10 scores for comparison [45, 46]. The other RAPID indices added little to RAPID3, and RAPID3 with scoring of 0–30 was recommended in all subsequent reports since 2009.
Fig. 4 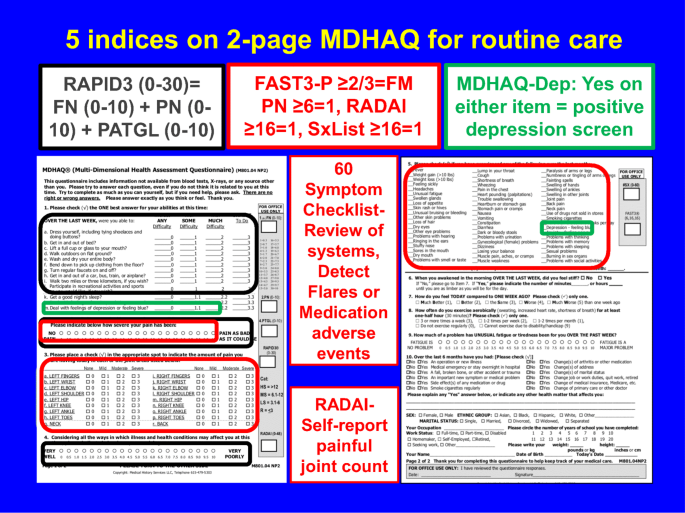
Five MDHAQ indices
RAPID3 provides similar results in RA clinical trials and clinical care to DAS28 (Disease Activity Score 28) [47] and CDAI (Clinical Disease Activity Index) [48] [33, 44•, 49,50,51,52], which include formal joint counts. RAPID3 is more likely to be abnormal in new RA patients than ESR, and more likely than ESR to document incomplete responses to methotrexate [53•]. RAPID3 is informative in osteoarthritis (OA) [9, 10, 54, 55], systemic lupus erythematosus (SLE) [54,55,56,57], ankylosing spondylitis (AS) [54, 58,58,59,60], psoriatic arthritis (PsA) [54, 61], gout [54], vasculitis [62], polymyalgia rheumatica (PMR) [4, 63], and others [4, 8, 54, 64, 65•] and even in non-rheumatic diagnoses [11••].
RAPID3 severity categories are > 12 = severe, 6.1–12 = moderate, 3.1–6 = low, and 0–3 = remission. In clinical trials, patients are selected for high disease activity; high RAPID3, DAS28, and CDAI scores generally indicate high inflammatory activity. In routine clinical care, high index scores may be based not only on inflammatory activity but also on joint damage and/or fibromyalgia [66•, 67•, 68••, 69•], just as an elevated ESR may be based on inflammatory activity, infection, and/or a lymphoma.
Similar considerations pertain to DAS28 and CDAI; patients who have no swollen joints and a normal ESR of 20 mm/h, but high tender joint counts and/or patient global assessment, may have moderate or high DAS28, CDAI, and RAPID3 (Table 2). Most routine clinical care databases indicate that fewer than 50% of patients are classified as in remission or even low activity according to an RA index, although many patients may have minimal inflammation, as high index scores may result from joint damage [66•, 67•], fibromyalgia [67•, 68••], and/or other comorbidities or distress [67•, 69•].
-
2.
FAST (fibromyalgia assessment screening tool) are cumulative indices to screen for fibromyalgia on the same MDHAQ used to score RAPID3 (Figs. 1–3) [12, 13•]; 1 point each is scored for a pain VNS ≥ 6, fatigue VNS ≥ 6, painful RADAI joint count ≥ 16, and symptom checklist ≥ 16. FAST3-P includes pain, RADAI, and symptoms, each scored 0 or 1, for a total of 0–3. FAST3-F includes fatigue, RADAI, and symptoms, again each scored 0 or 1 for a 0–3 total. FAST4 includes pain, fatigue, RADAI, and symptom checklist for a 0–4 total score [12, 13•]. Scores of 2/3 on FAST3-P or FAST3-F or 3/4 on FAST4 indicate a positive screen for fibromyalgia, which agree 89.4–91.7% with formal 2011 revised fibromyalgia criteria [12, 13•, 70]. The three versions of FAST indices have similar sensitivity and specificity to screen for fibromyalgia; FAST4 may provide greater specificity and generally is used by the authors in routine care. Longitudinal studies in progress may provide new information concerning an optimal choice. A diagnosis of fibromyalgia is made by a physician, but positive screening may be helpful and explain in part poor treatment responses according to a “treat to target” directive [71] in certain RA patients.
-
3.
MDHAQ-Dep (depression) indicates positive screening on the same MDHAQ if either of 2 depression items on the MDHAQ are present, either a score of ≥ 2.2 on the four-point scale or a check on the 60-symptom depression item [16•]. A positive screen for MDHAQ-Dep agrees 83.3% with Patient Health Questionnaire-9 (PHQ-9) [72] and 81.7% with the depression scale on the Hospital Anxiety and Depression Scale (HADS-D) [73], comparable to 82.2% agreement of these 2 reference screening scales for depression with one another [16•]. Again, a definitive diagnosis of depression is made by a physician, but a screening tool without requiring an additional questionnaire may be clinically useful and may explain poor responses to therapies in some patients.
-
4.
A self-report painful joint count on a rheumatoid arthritis disease activity index (RADAI) [74] is correlated significantly with a physician-performed tender joint count and at lesser levels with a swollen joint count. The RADAI painful joint count is informative in patients with many rheumatic diseases [75] and is included in the FAST indices [12, 13•].
-
5.
A 60-symptom checklist can serve as a review of systems and to screen for early detection of disease flares, comorbidities, and adverse effects of medications [11••]. This checklist is included in FAST and MDHAQ-Dep indices and has been reported to be of considerable value for early recognition of adverse events of medications and documentation of their resolution [11••].
Table 2 Indices to assess patients with rheumatoid arthritis who have no swollen joints and erythrocyte sedimentation rate of 20 mm/h

The MDHAQ provides quantitative data concerning fatigue [21] and 5 indices, which are not available on the HAQ, DAS28, or CDAI. MDHAQ scores and indices provide “multidimensional” information such as found on other comprehensive “generic” questionnaires, such as the SF-36 [29] and PROMIS [30] (see [14]) (Table 1).
A non-electronic, telemedicine MDHAQ is designed for the rheumatologist to send as a paper MDHAQ attachment to an Email (Fig. 3). The telemedicine MDHAQ specifically excludes personal health identifiers such as name, medical record number, or date of birth (although it does include year of birth to calculate age, which is often a confounder of variable scores). The patient prints the attachment, completes it in pencil, and returns it to the clinical site through an email or can bring it to the clinic for a face-to-face encounter. This version does require that the site which sends the telemedicine MDHAQ to a patient has some type of identifier, usually just a serial number. An electronic version is currently under development.
A digital eMDHAQ
Digital eMDHAQ versions have been developed for patient completion at home, any clinical setting, or anywhere the internet is available to report current clinical status and possible intercurrent problems such as disease flares, adverse effects of medications, or new comorbidities [15, 76]. Analyses of the eMDHAQ versus a paper version in 98 patients indicated that mean levels of 4 individual scores and 3 indices were all within 2%, with intraclass correlation coefficients of 0.86–0.98 (Table 3) [15]. Among 98 patients, 72% expressed a preference for an eMDHAQ, compared to 7% for the paper version, while 21% expressed no preference [15]. The eMDHAQ is secure and HIPAA-compliant [15] and includes the capacity to interface with any EMR through the HL 7 FHIR standard [77], but implementation into routine care has not been possible to date, as discussed in further detail below.
Patient questionnaires generally are not included in most EMRs as of February 2021, other than “intake” questionnaires to provide a medical history. This information generally is entered into the EMR by a physician, scribe, or other health professional. A wide range of administrative, logistic, financial, regulatory, design, workflow, and other problems contribute to barriers to integrate patient questionnaires into the EMR, discussed in further detail below.
Barriers to integration of patient questionnaires into an EMR resulting from limitations of the EMR in management of chronic diseases
The EMR was introduced in the early 2000s with extensive optimism that doctors and patients would enjoy improved convenience and outcomes [78,79,80]. The “P” in HIPAA stands for “portability,” suggesting easy transfer of medical information from one facility to another. The EMR was projected to increase revenue by capturing information that previously had been omitted from reimbursement [78,79,80].
An electronic format for an EMR does provide advantages in legibility compared to handwriting, accessibility across medical settings that use the same EMR, storage, and prevention of data loss with appropriate back-up. The EMR provides convenience of templates for review of systems, physical examination, joint count, medications, etc. However, many anticipated advances of the EMR remain unmet, and many unanticipated problems have emerged in EMR implementation, particularly in the management of chronic diseases [78,79,80].
A majority of physicians report that the EMR does not improve efficiency [81], with excessive clerical tasks [81] and interference with face-to-face patient care [82]. Several reports document that physicians spend at least as much time on their EMR tasks as in face-to-face clinical care [82,83,84]. Many physicians work after hours to complete their EMR tasks [82].
In 2020, most patients continue to complete different intake paper or electronic questionnaires at different care settings despite the similarity of much (often most) of the queried information. Portability is hardly more available than in the paper record era and often even less available [78]. Composition of EMR encounter notes often requires considerably more time than a pen-and-paper format, but many physicians find EMR notes less informative. The EMR is regarded by many, if not most, physicians as a source of stress [78,79,80, 85], which is reported to be rising [86].
The proposed goal of increased revenue through thorough documentation in an EMR may be met in acute inpatient settings but generally is not met in outpatient management of chronic diseases. Although revenue per encounter may be higher through capture of more information by the EMR, fewer encounters occur, leaving a net decrease in overall revenue in most settings.
Barriers to integration of a patient questionnaire into an EMR: design of the EMR according to a “biomedical model” for acute inpatient care with limited attention to a complementary “biopsychosocial model” for outpatient chronic disease management
One matter that is not addressed in a growing literature concerning limitations of the EMR is the design of the EMR according to a “biomedical model” [87, 88, 89••, 90, 91], the overarching paradigm of twentieth century medicine. In a biomedical model, “objective” data from a laboratory or imaging source are regarded as superior to “subjective” patient medical history narrative information [28] to inform clinical decisions. Patient self-report questionnaires are rarely included, other than as “intake” forms for new patients, from which selected information is entered into the EMR by a physician, scribe, or other health professional, as noted above.
In a biomedical model, information elicited in an interview with a health professional is regarded as more accurate and relevant to clinical decisions than patient self-report questionnaire data. Outcomes of diseases are regarded as resulting primarily from actions of health professionals; actions and attitudes of patients are regarded as of little importance [87, 88, 89••, 90, 91].
A biomedical model characterizes accurately many spectacular advances in medicine over the last 150 years [92] and remains the dominant paradigm of medical care. However, this model is most relevant to acute inpatient medical activities and is limited to characterize management and outcomes of chronic diseases. Nonetheless, dramatic acute medical events remain a staple of perceptions of “health care” of the public (e.g., television shows) and even many health professionals, with limited (or no) attention to matters such as shared decisions for chronic diseases such as rheumatoid arthritis. Furthermore, the acute care hospital remains the setting of most medical education and training, reinforcing the dominance of the biomedical model.
Many aspects of outpatient management of chronic rheumatic diseases (and chronic diseases in general) over long periods may involve a complementary “biopsychosocial model” in addition to a traditional biomedical model [87, 92, 93]. In a biopsychosocial model, information from a patient medical history, rather than laboratory tests or ancillary studies, accounts for more than 50% of clinical decisions in diagnosis and management of RA, unlike many chronic diseases such as hypertension or diabetes [94••]. Scores for physical function on a quantitative patient questionnaire and patient socioeconomic status generally are (far) more significant in the prognosis of long-term RA clinical outcomes such as work disability [34, 35, 95, 96] and premature mortality [35, 97,98,99,100] than laboratory tests or imaging. Physical function and exercise responses on a patient questionnaire are more significant to predict mortality in the general population than smoking [24•]. Patient attitudes and behaviors may be as important in outcomes of chronic rheumatic diseases as the actions of health professionals and medications [87, 92].
The design of an EMR according to a biomedical model oriented to acute medical care has left patient questionnaires generally not only excluded but also difficult to introduce into routine care [87, 92, 93]. Differences in workflow in management of acute inpatient medical problems versus outpatient management of chronic diseases may not have been recognized as problematic when traditional paper records were used, but may explain some of the problems of rheumatologists in using patient questionnaires in the EMR era [35, 42, 100].
The dominance of a biomedical model in medical education and training leaves patient questionnaires regarded as “adjuncts” to patient care, not central to clinical decisions by many rheumatologists. Patient questionnaires generally are not included in most medical school curricula and rheumatology fellowship training programs (35 years after physical function was documented to be more significant to predict mortality than laboratory tests or imaging [35]). Therefore, development of the EMR according to a biomedical model may explain in part structural features of EMRs which limit the introduction of patient self-report questionnaires.
Barriers to integration of a patient questionnaire into an EMR: some physician concerns about the possible value of patient questionnaires for clinical decisions
Many physicians, including rheumatologists, continue to believe that information collected by a health professional is invariably more accurate than information provided by a patient on a self-report questionnaire, despite recognition of the accuracy of patient self-report medical history information over many decades [27]. Of course, health professionals know more than patients about pathophysiology, diagnosis, and treatment. Nonetheless, 80% of patients know more about their details of family history, surgeries, symptoms, medication compliance, levels of pain or fatigue, and other matters. A reader of this article likely can provide more accurate medical information concerning past medical history through self-report than through an interview by a health professional (do you agree?).
Another concern of some physicians is that a patient questionnaire such as an MDHAQ is designed to replace conversation with the patient. On the contrary, the questionnaire serves to enhance the conversation through emphasis on the primary concerns of both patient and doctor to improve doctor-patient communication. Self-report of medical history information always requires interpretation by a knowledgeable and caring health professional based on information elicited in doctor-patient communication, just as data from a laboratory, imaging, or any source. For example, a high score for pain may be based on inflammatory activity, joint damage, and/or fibromyalgia, just as a high ESR may be based on inflammatory activity, infection, and/or a lymphoma.
A further concern is that collection of more data invariably leads to more work on the part of the physician. However, almost all the additional work in completion of patient questionnaires is performed by the patient rather than the physician; availability of the data at the encounter generally saves time for the doctor, provided that guidelines to workflow are observed. The opportunity to save time while having more thorough and accurate information may be even greater with electronic versions of patient questionnaires, again requiring attention and adjustments to workflow.
“Workarounds” to address limitations of EMRs to incorporate patient questionnaires: use of only RAPID3 in contrast to the full MDHAQ
Limitations to link patient questionnaires into EMRs [15, 76, 101•] have led to various “workarounds.” The most widely used involves continued use of paper questionnaires, 12 years after widespread introduction of EMRs, which are then scanned into the EMR as PDFs. A second involves stand-alone Web-based tools that interact with the EMR [101•], as proposed in this article. A third involves inclusion of only limited data, such as only RAPID3 from the MDAHQ, discussed in greater detail below.
RAPID3 is the most widely used RA index among US rheumatologists [102] and provides similar results to disease-specific questionnaires in all rheumatic diseases studied [3, 4, 43, 54, 56, 65•], and even in non-rheumatic diagnoses [65•]. RAPID3 includes only about 30% of the full MDHAQ and omits scores for fatigue, exercise, morning stiffness, change in status, FAST3, MDHAQ-Dep, patient self-report painful joint count, 60-symptom checklist, and medical history information. All published reports concerning the development of RAPID3 have presented the index as a component of the full MDHAQ (see [9, 15, 103••]. The full MDHAQ requires 5–10 min versus 2–3 min for RAPID3 — the additional time is that of the patient. The authors suggest that any possible advantage to collection of only RAPID3 appears outweighed considerably by the absence of much relevant information that requires no more work on the part of the physician.
Encounter workflow to optimize the use of MDHAQ and eMDHAQ
It is critical to collect the MDHAQ before the doctor sees the patient. Traditionally, the clinic receptionist presents a paper MDHAQ to each patient upon registration for the visit. The same MDHAQ (albeit in different versions — Figs. 1–3) is used for patients with all diagnoses at all visits. An eMDHAQ (Fig. 3) can be completed at home, including for telemedicine visits.
Most patients require no instructions to complete an MDHAQ. Reproducibility of responses is highest when responses are from only a single observer (the patient) without any input from a health professional or family member [19]. Any query from a patient that “I am not sure how to fill this out,” should elicit a response from office staff that “whatever you say is correct.” Sometimes help from a family member or staff professional is needed and should be willingly offered, but with as little “help” as possible to respond to a query — “whatever you say is correct.” It is a good practice for the treating physician to review the MDHAQ report briefly before engaging in conversation with patient.
Conclusion
The MDHAQ provides clinically important quantitative patient data to assist the clinician in their assessment and management in all rheumatic diseases studied. When appropriately integrated into the clinical workflow, the MDHAQ can save time for the doctor and patient, while increasing available medical history information. Although an electronic version of the MDHAQ is available with capacity for EMR integration, implementation has proven difficult to date. A separate electronic MDHAQ database and/or scanning of questionnaires into an EMR are feasible alternatives, and the absence of EMR integration should not be a barrier to the collection of an MDHAQ from each patient in routine care. It is recommended that the use of the entire MDHAQ provides significant incremental information beyond a RAPID3 score, while requiring 5–10 min versus 2–5 min of patient time and providing considerably more medical history information to the clinician. Considerable further details concerning the paper and eMDHAQ can be found in previous review articles [6, 8, 15, 65•, 76]. The authors welcome queries from health professionals, administrators, EMR vendors, and patients.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Pincus T, Swearingen C, Wolfe F. Toward a multidimensional Health Assessment Questionnaire (MDHAQ): assessment of advanced activities of daily living and psychological status in the patient-friendly health assessment questionnaire format. Arthritis Rheum. 1999;42(10):2220–30.
Pincus T, Sokka T, Kautiainen H. Further development of a physical function scale on a MDHAQ for standard care of patients with rheumatic diseases. J Rheumatol. 2005;32(8):1432–9.
Pincus T, Askanase AD, Swearingen CJ. A multi-dimensional health assessment questionnaire (MDHAQ) and routine assessment of patient index data (RAPID3) scores are informative in patients with all rheumatic diseases. Rheum Dis Clin North Am. 2009;35(4):819–27 x.
Castrejon I. The use of MDHAQ/RAPID3 in different rheumatic diseases a review of the literature. Bull Hosp Jt Dis. 2017;75(2):93–100.
Berwick DM. Continuous improvement as an ideal in health care. N Engl J Med. 1989;320(1):53–6.
Pincus T, Maclean R, Yazici Y, Harrington JT. Quantitative measurement of patient status in the regular care of patients with rheumatic diseases over 25 years as a continuous quality improvement activity, rather than traditional research. Clin Exp Rheumatol. 2007;25(6 Suppl 47):69–81.
Uhlig T, Kvien TK, Pincus T. Test-retest reliability of disease activity core set measures and indices in rheumatoid arthritis. Ann Rheum Dis. 2009;68(6):972–5.
Pincus T, Castrejon I. Are patient self-report questionnaires as "scientific" as biomarkers in "treat-to-target" and prognosis in rheumatoid arthritis? Curr Pharm Des. 2015;21(2):241–56.
el-Haddad C, Castrejon I, Gibson KA, Yazici Y, Bergman M, Pincus T. MDHAQ/RAPID3 scores in patients with osteoarthritis are similar to or higher than in patients with rheumatoid arthritis: a cross-sectional study from current routine rheumatology care at 4 sites. RMD Open. 2017;3:e000391.
Chua JR, Jamal S, Riad M, Castrejon I, Malfait AM, Block JA, et al. Disease burden in osteoarthritis is similar to that of rheumatoid arthritis at initial rheumatology visit and significantly greater six months later. Arthritis Rheumatol. 2019;71(8):1276–84.
•• Schmukler J, Pincus T. New applications of the MDHAQ: Can remote use improve detection of adverse events due to high-risk medications? The Rheumatologist [Internet]. 2019. Available from: https://www.the-rheumatologist.org/article/remote-use-of-the-multidimensional-health-assessment-questionnaire-mdhaq. The value of MDHAQ/RAPID3 to monitor a patient with pulmonary fibrosis and no joint disease, to screen for adverse events of medications, and to use in telemedicine is described.
Schmukler J, Jamal S, Castrejon I, Block JA, Pincus T. Fibromyalgia Assessment Screening Tools (FAST) Based on Only Multidimensional Health Assessment Questionnaire (MDHAQ) scores as clues to fibromyalgia. ACR Open Rheumatol. 2019;1(8):516–25.
• Gibson KA, Castrejon I, Descallar J, Pincus T. Fibromyalgia Assessment Screening Tool (FAST): clues to fibromyalgia on a multidimensional health assessment questionnaire (MDHAQ) for routine care. J Rheumatol. 2019. FAST (Fibromyalgia Assessment Screening Tool) indices within the MDHAQ agree 89.4-91.7% with reference formal 2011 revised fibromyalgia criteria, without a need for an additional questionnaire.
Gibson KA, Pincus T. Patient physical function in rheumatoid arthritis. In: Scott DG, editor. Rheumatoid arthritis: Oxford University Press; 2020. p. 287–98.
Pincus T, Castrejon I, Riad M, Obreja E, Lewis C, Krogh NS. Reliability, feasibility, and patient acceptance of an electronic version of a multidimensional health assessment questionnaire for routine rheumatology care: validation and patient preference study. JMIR Form Res. 2020;4(5):e15815.
• Morla RM, Li T, Castrejon I, Luta G, Pincus T. multidimensional health assessment questionnaire as an effective tool to screen for depression in routine rheumatology care. Arthritis Care Res. 2021;73(1):120-129. An index to screen for depression within the MDHAQ agrees 81.7-83.3% with reference PHQ9 (patient health questionnaire 9) and HADS-D (hospital anxiety and depression scale), similar to 82% agreement of these scales with one another (29) in patients with RA, SpA or psoriatic arthritis, without a need for an additional questionnaire.
Pincus T, Yazici Y, Bergman MJ. Patient questionnaires in rheumatoid arthritis: advantages and limitations as a quantitative, standardized scientific medical history. Rheum Dis Clin North Am. 2009;35(4):735–43 vii.
Boers M, Tugwell P, Felson DT, van Riel PL, Kirwan JR, Edmonds JP, et al. World Health Organization and International League of Associations for Rheumatology core endpoints for symptom modifying antirheumatic drugs in rheumatoid arthritis clinical trials. The J Rheumatol Suppl. 1994;41:86–9.
Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis and Rheum. 1980;23(2):137–45.
Pincus T, Bergman M, Sokka T, Roth J, Swearingen C, Yazici Y. Visual analog scales in formats other than a 10 centimeter horizontal line to assess pain and other clinical data. J Rheumatol. 2008;35(8):1550–8.
Castrejon I, Nikiphorou E, Jain R, Huang A, Block JA, Pincus T. Assessment of fatigue in routine care on a Multidimensional Health Assessment Questionnaire (MDHAQ): a cross-sectional study of associations with RAPID3 and other variables in different rheumatic diseases. Clin Exp Rheumatol. 2016.
Yazici Y, Pincus T, Kautiainen H, Sokka T. Morning stiffness in patients with early rheumatoid arthritis is associated more strongly with functional disability than with joint swelling and erythrocyte sedimentation rate. J Rheumatol. 2004;31(9):1723–6.
Sokka T, Hakkinen A, Kautiainen H, Maillefert JF, Toloza S, Mork Hansen T, et al. Physical inactivity in patients with rheumatoid arthritis: data from twenty-one countries in a cross-sectional, international study. Arthritis Rheum. 2008;59(1):42–50.
•• Sokka T, Pincus T. Poor physical function, pain and limited exercise: risk factors for premature mortality in the range of smoking or hypertension, identified on a simple patient self-report questionnaire for usual care. BMJ Open. 2011;1(1):e000070. Poor physical function on a self-report questionnaire identifies the risk for mortality over the subsequent 5 years in a general elderly poplulation free of severe disease, in the range of smoking or hypertension, suggesting that self-reported functional disability is a likely risk factor for mortality in many diseases, as is recognized in rheumatoid arthritis.
Castrejon I, Yazici Y, Celik S, Pincus T. Pragmatic assessment of exercise in routine care using an MDHAQ: associations with changes in RAPID3 and other clinical variables. Arthritis Res Ther. 2016;18:199.
Pincus T, Yazici Y, Castrejon I. pragmatic and scientific advantages of MDHAQ/ RAPID3 completion by all patients at all visits in routine clinical care. Bull NYU Hosp Jt Dis. 2012;70(Suppl 1):30–6.
Gumpel JM, Mason AM. Self-administered clinical questionnaire for outpatients. Br Med J. 1974;2(5912):209–12.
Weed LL. Medical records that guide and teahc. N Engl J Med. 1968;278(12):652–7 concl.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–83.
Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol. 2010;63(11):1179–94.
Pincus T, Castrejon I. MDHAQ/RAPID3 scores: quantitative patient history data in a standardized "scientific" format for optimal assessment of patient status and quality of care in rheumatic diseases. Bull NYU Hosp Jt Dis. 2011;69(3):201–14.
Pincus T, Callahan LF, Brooks RH, Fuchs HA, Olsen NJ, Kaye JJ. Self-report questionnaire scores in rheumatoid arthritis compared with traditional physical, radiographic, and laboratory measures. Ann Intern Med. 1989;110(4):259–66.
Pincus T, Richardson B, Strand V, Bergman MJ. Relative efficiencies of the 7 rheumatoid arthritis Core Data Set measures to distinguish active from control treatments in 9 comparisons from clinical trials of 5 agents. Clin Exp Rheumatol. 2014;32 Suppl 85(5):47–54.
Yelin E, Meenan R, Nevitt M, Epstein W. Work disability in rheumatoid arthritis: effects of disease, social, and work factors. Ann Intern Med. 1980;93(4):551–6.
Pincus T, Callahan LF, Sale WG, Brooks AL, Payne LE, Vaughn WK. Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum. 1984;27(8):864–72.
Lubeck DP, Spitz PW, Fries JF, Wolfe F, Mitchell DM, Roth SH. A multicenter study of annual health service utilization and costs in rheumatoid arthritis. Arthritis Rheum. 1986;29(4):488–93.
Wolfe F, Hawley DJ. The longterm outcomes of rheumatoid arthritis: Work disability: a prospective 18 year study of 823 patients. J Rheumatol. 1998;25(11):2108–17.
Wolfe F, Zwillich SH. The long-term outcomes of rheumatoid arthritis: a 23-year prospective, longitudinal study of total joint replacement and its predictors in 1,600 patients with rheumatoid arthritis. Arthritis Rheum. 1998;41(6):1072–82.
Soderlin MK, Nieminen P, Hakala M. Functional status predicts mortality in a community based rheumatoid arthritis population. J Rheumatol. 1998;25(10):1895–9.
Michaud K, Messer J, Choi HK, Wolfe F. Direct medical costs and their predictors in patients with rheumatoid arthritis: a three-year study of 7,527 patients. Arthritis Rheum. 2003;48(10):2750–62.
Farragher TM, Lunt M, Bunn DK, Silman AJ, Symmons DP. Early functional disability predicts both all-cause and cardiovascular mortality in people with inflammatory polyarthritis: results from the Norfolk Arthritis Register. Ann Rheum Dis. 2007;66(4):486–92.
Sokka T, Abelson B, Pincus T. Mortality in rheumatoid arthritis: 2008 update. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S35–61.
Pincus T, Swearingen CJ, Bergman MJ, Colglazier CL, Kaell AT, Kunath AM, et al. RAPID3 (Routine Assessment of Patient Index Data) on an MDHAQ (Multidimensional Health Assessment Questionnaire): agreement with DAS28 (Disease Activity Score) and CDAI (Clinical Disease Activity Index) activity categories, scored in five versus more than ninety seconds. Arthritis Care Res. 2010;62(2):181–9.
• Pincus T, Yazici Y, Bergman MJ. RAPID3, an index to assess and monitor patients with rheumatoid arthritis, without formal joint counts: similar results to DAS28 and CDAI in clinical trials and clinical care. Rheum Dis Clin North Am. 2009;35(4):773–778, viii. RAPID3 provides similar results to DAS28 and CDAI in clinical trials and clinical care to assess and monitor patients with rheumatoid arthritis, with patients performing most of the work.
Pincus T, Swearingen CJ, Bergman M, Yazici Y. RAPID3 (Routine Assessment of Patient Index Data 3), a rheumatoid arthritis index without formal joint counts for routine care: proposed severity categories compared to disease activity score and clinical disease activity index categories. J Rheumatol. 2008;35(11):2136–47.
Pincus T, Bergman MJ, Yazici Y, Hines P, Raghupathi K, Maclean R. An index of only patient-reported outcome measures, routine assessment of patient index data 3 (RAPID3), in two abatacept clinical trials: similar results to disease activity score (DAS28) and other RAPID indices that include physician-reported measures. Rheumatology (Oxford). 2008;47(3):345–9.
Prevoo ML. van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44–8.
Aletaha D, Smolen J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S100–8.
Pincus T, Amara I, Koch GG. Continuous indices of core data set measures in rheumatoid arthritis clinical trials: lower responses to placebo than seen with categorical responses with the American College of Rheumatology 20% criteria. Arthritis Rheum. 2005;52(4):1031–6.
Pincus T, Hines P, Bergman MJ, Yazici Y, Rosenblatt LC, MacLean R. Proposed severity and response criteria for Routine Assessment of Patient Index Data (RAPID3): results for categories of disease activity and response criteria in abatacept clinical trials. J Rheumatol. 2011;38(12):2565–71.
Pincus T, Amara I, Segurado OG, Bergman M, Koch GG. Relative efficiencies of physician/assessor global estimates and patient questionnaire measures are similar to or greater than joint counts to distinguish adalimumab from control treatments in rheumatoid arthritis clinical trials. J Rheumatol. 2008;35(2):201–5.
Strand V, Cohen S, Crawford B, Smolen JS, Scott DL, Leflunomide IG. Patient-reported outcomes better discriminate active treatment from placebo in randomized controlled trials in rheumatoid arthritis. Rheumatology (Oxford). 2004;43(5):640–7.
• Pincus T. RAPID3, an index of only 3 patient self-report core data set measures, but not ESR, recognizes incomplete responses to methotrexate in usual care of patients with rheumatoid arthritis. Bull Hosp Jt Dis (2013). 2013;71(2):117–20. Incomplete responses to methotrexate (MTX) in patients with rheumatoid arthritis are documented far more effectively by RAPID3 than by ESR (erythrocyte sedimemanation rate), as ESR generally normalizes with MTX treatment, regardless of clinical responses.
Castrejon I, Bergman MJ, Pincus T. MDHAQ/RAPID3 to recognize improvement over 2 months in usual care of patients with osteoarthritis, systemic lupus erythematosus, spondyloarthropathy, and gout, as well as rheumatoid arthritis. J Clin Rheumatol: practical reports on rheumatic & musculoskeletal diseases. 2013;19(4):169–74.
Pincus T, Castrejon I, Yazici Y, Gibson KA, Bergman MJ, Block JA. Osteoarthritis is as severe as rheumatoid arthritis: evidence over 40 years according to the same measure in each disease. Clin Exp Rheumatol. 2019;37 Suppl 120(5):7–17.
Askanase AD, Castrejon I, Pincus T. Quantitative data for care of patients with systemic lupus erythematosus in usual clinical settings: a patient Multidimensional Health Assessment Questionnaire and physician estimate of noninflammatory symptoms. J Rheumatol. 2011;38(7):1309–16.
Annapureddy N, Giangreco D, Devilliers H, Block JA, Jolly M. Psychometric properties of MDHAQ/RAPID3 in patients with systemic lupus erythematosus. Lupus. 2018:961203318758503.
Danve A, Reddy A, Vakil-Gilani K, Garg N, Dinno A, Deodhar A. Routine Assessment of Patient Index Data 3 score (RAPID3) correlates well with Bath Ankylosing Spondylitis Disease Activity index (BASDAI) in the assessment of disease activity and monitoring progression of axial spondyloarthritis. Clin Rheumatol. 2015;34(1):117–24.
Cinar M, Yilmaz S, Cinar FI, Koca SS, Erdem H, Pay S, et al. A patient-reported outcome measures-based composite index (RAPID3) for the assessment of disease activity in ankylosing spondylitis. Rheumatol Int. 2015.
Park SH, Choe JY, Kim SK, Lee H, Castrejon I, Pincus T. Routine Assessment of Patient Index Data (RAPID3) and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores yield similar information in 85 Korean patients with ankylosing spondylitis seen in usual clinical care. J Clin Rheumatol : Practical Reports on Rheumatic & Musculoskeletal Diseases. 2015;21(6):300–4.
Coates LC, Tillett W, Shaddick G, Pincus T, Kavanaugh A, Helliwell PS. Value of the routine assessment of patient index data 3 in patients with psoriatic arthritis: results from a tight-control clinical trial and an observational cohort. Arthritis Care Res. 2018;70(8):1198–205.
Annapureddy N, ElsallabiO, Baker J, Sreih AG. Patient-reported outcomes in ANCA-associated vasculitis. A comparison between Birmingham Vasculitis Activity Score and routine assessment of patient index data 3. Clin Rheumatol. 2015.
Castrejon I, Huang A, Everakes SL, Nika A, Sequeira W. Clinical Improvement According to RAPID3 in Patients With Polymyalgia Rheumatica: A Longitudinal Analysis From Routine Care. Journal of clinical rheumatology : practical reports on rheumatic & musculoskeletal diseases. 2018;24(7):390–2.
Pincus T, Swearingen CJ. The HAQ compared with the MDHAQ: "keep it simple, stupid" (KISS), with feasibility and clinical value as primary criteria for patient questionnaires in usual clinical care. Rheum Dis Clin North Am. 2009;35(4):787–98 ix.
• Pincus T, Mandelin AM 2nd, Swearingen CJ. Flowsheets that include MDHAQ physical function, pain, global, and RAPID3 scores, laboratory tests, and medications to monitor patients with all rheumatic diseases: an electronic database for an electronic medical record. Rheum Dis Clin North Am. 2009;35(4):829–42, x-xi. MDHAQ/RAPID3 is informative in all rheumatic diseases.
• Ruiz-Medrano E, Espinosa-Ortega HF, Arce-Salinas CA. The effect of concomitant hand osteoarthritis on pain and disease activity in patients with rheumatoid arthritis. Clin Rheumatol. h;38(10)):2709–16. A cross-sectional study documents higher rheumatoid arthritis index scores in patients who have secondary osteoarthritis of the hand compared to those who do not have secondary osteoarthritis according to DAS28 (Disease Activity Score 28), SDAI (Simplified Disease Activity Index, CDAI (Clinical Disease Activity Index) and PASS (Patient Acceptable Symptom State).
• Castrejon I, Gibson KA, Block JA, Everakes SL, Jain R, Pincus T, et al. Bull Hosp Jt Dis (2013). 2015;73(3):178–84. A short physician questionnaire completed in less than a minute to depict levels of inflammation, damage and distress as quantitative 0–10 scores rather than narrative descriptions, to help support clinical decisions and monitor patient status over time.
•• Duffield SJ, Miller N, Zhao S, Goodson NJ. Concomitant fibromyalgia complicating chronic inflammatory arthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2018;57((8):1453–60. An elegant meta-analysis which documents that patients with who have concomitant fibromyalgia have significantly higher DAS28 in rheumatoid arthritis and BASDAI in axial spondyloarthropathies compared to patients who do not have fibromyalgia.
• Tymms K, Zochling J, Scott J, Bird P, Burnet S, de Jager J, et al. Barriers to optimal disease control for rheumatoid arthritis patients with moderate and high disease activity. Arthritis Care Res. 2014;66(2):190–6. Early documentation of barriers to implementation of the “treat to target” directive for the treatment of rheumatoid arthritis due to fibromyalgia, secondary osteoarthritis, patient and/or physician preferences, and other reasons.
Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Hauser W, Katz RS, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol. 2011;38(6):1113–22.
Smolen JS, Aletaha D, Bijlsma JW, Breedveld FC, Boumpas D, Burmester G, et al. Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2010;69(4):631–7.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Stucki G, Liang MH, Stucki S, Bruhlmann P, Michel BA. A self-administered rheumatoid arthritis disease activity index (RADAI) for epidemiologic research. Psychometric properties and correlation with parameters of disease activity. Arthritis Rheum. 1995;38(6):795–8.
Castrejon I, Yazici Y, Pincus T. Patient self-report RADAI (Rheumatoid Arthritis Disease Activity Index) joint counts on an MDHAQ (Multidimensional Health Assessment Questionnaire) in usual care of consecutive patients with rheumatic diseases other than rheumatoid arthritis. Arthritis Care Res. 2013;65(2):288–93.
Pincus T. Electronic multidimensional health assessment questionnaire (eMDHAQ): past, present and future of a proposed single data management system for clinical care, research, quality improvement, and monitoring of long-term outcomes. Clin Exp Rheumatol. 2016;34(5 Suppl 101):S17–33.
Saripalle R, Runyan C, Russell M. Using HL7 FHIR to achieve interoperability in patient health record. J Biomed Inform. 2019;94:103188.
Wachter RM. The digital doctor : hope, hype, and harm at the dawn of medicine's computer age. New York: McGraw-Hill Education; 2015. xv, 330 pages p.
Gawande A. Why Doctors hate their computers. The New Yorker [Internet]. 2018; Available from: https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers.
Schulte F, Fry E. Death by 1,000 clicks: where electronic health records went wrong. Fortune, Kaiser Health News [Internet]. 2019; Available from: https://khn.org/news/death-by-a-thousand-clicks/.
Shanafelt TD, Dyrbye LN, Sinsky C, Hasan O, Satele D, Sloan J, et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(7):836–48.
Arndt BG, Beasley JW, Watkinson MD, Temte JL, Tuan WJ, Sinsky CA, et al. Tethered to the EHR: primary care physician workload assessment using EHR event log data and time-motion observations. Ann Fam Med. 2017;15(5):419–26.
Sinsky C, Colligan L, Li L, Prgomet M, Reynolds S, Goeders L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753–60.
Tai-Seale M, Olson CW, Li J, Chan AS, Morikawa C, Durbin M, et al. Electronic health record logs indicate that physicians split time evenly between seeing patients and desktop medicine. Health Aff (Millwood). 2017;36(4):655–62.
Armstrong-Coben A. The computer will see you now. New York Times [Internet]. 2009. Available from: https://www.nytimes.com/2009/03/06/opinion/06coben.html.
Heponiemi T, Hypponen H, Vehko T, Kujala S, Aalto AM, Vanska J, et al. Finnish physicians' stress related to information systems keeps increasing: a longitudinal three-wave survey study. BMC Med Inform Decis Mak. 2017;17(1):147.
Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–36.
Callahan LF, Pincus T. Education, self-care, and outcomes of rheumatic diseases: further challenges to the "biomedical model" paradigm. Arthritis Care Res. 1997;10(5):283–8.
•• Pincus T, Esther R, DeWalt DA, Callahan LF, et al. Annals of internal medicine. 1998;129(5):406–11. A summary of evidence that patient socioeconomic status, living conditions, self-management, and other “non-medical” variables are powerful determinants of the incidence, prevalence, morbidity and mortality of most chronic diseases.
Abelson B, Rupel A, Pincus T. Limitations of a biomedical model to explain socioeconomic disparities in mortality of rheumatic and cardiovascular diseases. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S25–34.
Pincus T, Castrejon I. Low socioeconomic status and patient questionnaires in osteoarthritis: challenges to a "biomedical model" and value of a complementary "biopsychosocial model". Clin Exp Rheumatol. 2019;37 Suppl 120(5):18–23.
McCollum L, Pincus T. A biopsychosocial model to complement a biomedical model: patient questionnaire data and socioeconomic status usually are more significant than laboratory tests and imaging studies in prognosis of rheumatoid arthritis. Rheum Dis Clin North Am. 2009;35(4):699–712 v.
Pincus TCJ, Gibson KA. Evidence from a Multidimensional Health Assessment Questionnaire (MDHAQ) of the value of a biopsychosocial model to complement a traditional biomedical model in care of patients with rheumatoid arthritis. J Rheum Dis. 2016;23(4):212–33.
•• Castrejon I, McCollum L, Tanriover MD, Pincus T. Importance of patient history and physical examination in rheumatoid arthritis compared to other chronic diseases: Results of a physician survey. Arthritis Care Res. 2012;64(8):1250–5. The patient history is far more important in diagnosis and management of rheumatoid arthritis than most chronic diseases, such as hypertension or diabetes, in which the approach is dominated by a “gold standard” biomarker; a patient self-report questionnaire may be regarded as providing patient history information as quantitative scores for monitoring over time rather than “subjective” narrative descriptions.
Yelin E, Callahan LF. The economic cost and social and psychological impact of musculoskeletal conditions. National Arthritis Data Work Groups. Arthritis Rheum. 1995;38(10):1351–62.
Mitchell JM, Burkhauser RV, Pincus T. The importance of age, education, and comorbidity in the substantial earnings losses of individuals with symmetric polyarthritis. Arthritis Rheum. 1988;31(3):348–57.
Pincus T, Callahan LF. Prognostic markers of activity and damage in rheumatoid arthritis: why clinical trials and inception cohort studies indicate more favourable outcomes than studies of patients with established disease. Br J Rheumatol. 1995;34(3):196–9.
Gordon DA, Stein JL, Broder I. The extra-articular features of rheumatoid arthritis. A systematic analysis of 127 cases. Am J Med. 1973;54(4):445–52.
Wolfe F, Mitchell DM, Sibley JT, Fries JF, Bloch DA, Williams CA, et al. The mortality of rheumatoid arthritis. Arthritis Rheum. 1994;37(4):481–94.
Pincus T, Brooks RH, Callahan LF. Prediction of long-term mortality in patients with rheumatoid arthritis according to simple questionnaire and joint count measures. Ann Intern Med. 1994;120(1):26–34.
• Newman ED, Lerch V, Billet J, Berger A, Kirchner HL. Improving the quality of care of patients with rheumatic disease using patient-centric electronic redesign software. Arthritis Care Res. 2015;67(4):546–53. One of the few successful implementations of an electronic MDHAQ to assess and monitor patients in routine clinical care.
England BR, Tiong BK, Bergman MJ, Curtis JR, Kazi S, Mikuls TR, et al. 2019 update of the american college of rheumatology recommended rheumatoid arthritis disease activity measures. Arthritis Care Res. 2019;71(12):1540–55.
•• Pincus T, Schmukler J, Castrejon I. Patient questionnaires in osteoarthritis: what patients teach doctors about their osteoarthritis on a multidimensional health assessment questionnaire (MDHAQ) in clinical trials and clinical care. Clin Exp Rheumatol. 2019;37 Suppl 120(5):100–11. Physicians may save time and have availabe more complete information from the patient medical history using the MDHAQ in routine clinical care.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Rheumatoid Arthritis
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gibson, K.A., Pincus, T. A Self-Report Multidimensional Health Assessment Questionnaire (MDHAQ) for Face-To-Face or Telemedicine Encounters to Assess Clinical Severity (RAPID3) and Screen for Fibromyalgia (FAST) and Depression (DEP). Curr Treat Options in Rheum 7, 161–181 (2021). https://doi.org/10.1007/s40674-021-00175-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40674-021-00175-0