
Abstract
Feelings of burnout in professional students have been associated with additional psychological morbidities and decreased academic achievement. Due to the large volume of content that medical students need to learn during gross anatomy courses, it is possible that anatomical self-efficacy may be a contributing factor to feelings of burnout. Anatomical self-efficacy is defined as a student’s judgment of their ability to execute tasks related to learning anatomy and perform course activities (e.g., dissection). First-year medical students were invited to provide basic demographic information at the beginning of the semester and to complete the Oldenburg Burnout Inventory-student version (OLBI-SS) and the Anatomical Self-Efficacy Instrument (ASEI); at the beginning, middle, and end of the semester, they were enrolled in gross anatomy. Typical descriptive statistics for the demographic information were conducted, as well as, correlational analyses assessing if the information had a relationship with either anatomical self-efficacy or burnout. Female students were more burnt out than male students. Repeated measures ANOVA revealed that students’ feelings of burnout significantly increased from the beginning of the semester to the midpoint and the end of the semester (p < 0.05). Linear regression demonstrated a predictive relationship between anatomical self-efficacy and burnout (p < 0.05) at all three measurement points in which lower self-efficacy was predictive of increased feelings of burnout.
Similar content being viewed by others

Introduction
First-year medical students tend to find themselves in a stressful academic environment that leads to a significantly lower quality of mental health [1, 2] and burnout [1, 3] as compared to the general population of similar age. Some studies have found that up to one-in-four of their medical student participants are at high risk for burnout [4]. Burnout is a psychological syndrome that is characterized by increased emotional exhaustion, depersonalization, and decreased personal accomplishment in individuals who work with people in some capacity [5]. Burnout is a serious problem for all health professionals at every stage of their career [3, 6,7,8]. Burnout is a major issue for medical professionals as it is associated with other psychological disorders such as higher perceived stress, anxiety, depression, and unhealthy alcohol consumption [1, 3, 7,8,9,10]. The most troubling of these psychological comorbidities is suicidal ideation [1, 3, 7,8,9]. Dyrbye et al. [1] found that 11.2% of surveyed medical students, double the national average for the same age group, had considered suicide in the past year. These findings were strongly correlated with feelings of burnout, and students who met the criteria for burnout were two to three times more likely to have suicidal ideation [1]. Burnout may also threaten the integrity of the medical field. Dyrbye et al. [11] found that students who met the criteria of burnout were significantly more likely to omit patient examination findings or cheat on tests.
Several factors can affect stress and burnout in medical students, including but not limited to course load, moving away from home, incurring more student loan debt, or having stressful/negative interpersonal relationships with either peers, romantic partners, or instructors [2, 3, 12]. Many medical students are confronted with some combination, if not all of these factors simultaneously upon matriculating medical school. Another potential risk factor for individuals’ burnout is their gender. Some studies have found disparities between the relationship of burnout and gender [6, 13, 14], though there are mixed findings as to which gender is at higher risk, while other studies found no such association [4, 7]. Another contributor to burnout is the level of mistreatment students experience during their clinical years. Cook et al. found that 83% of the surveyed medical students had at least one experience of mistreatment by a faculty member or a resident, while 10.7% and 12.6% of students experienced recurring mistreatment by the faculty and residents, respectively [15]. Their study found that 34.1% of the surveyed students met the criteria for burnout and were significantly more likely to be burnt out if they experienced mistreatment.
While mistreatment in clinical training may contribute to burnout, students can still exhibit burnout in their preclinical education [4, 7]. A study investigating individuals at different points in their medical career found that early-career physicians (those with less than 5 years of practice) were less burnt out than residents and medical students [3]. This supports the claim that burnout begins early in an individual’s medical education and continues into residency [3, 16,17,18]. A suggested stressor in the preclinical phase of medical education that contributes to burnout is anatomy dissection/course work [3], and significant associations have been found between medical students’ reported feelings of stress about dissection and meeting the criteria for psychological morbidity on the General Health Questionnaire [2].
When considering how gross anatomy coursework may impact feelings of stress and burnout, it is important to consider anatomical self-efficacy. Self-efficacy, in general, refers to an individual’s judgments of their own ability to carry out a particular task [19], and it is well established that self-efficacy is positively correlated with academic success [20, 21]. Low self-efficacy has been shown to be associated with decreased motivation and increased anxiety [20], both of which are seen in burnout. A recent study demonstrated that the link between self-efficacy and academic achievement is quite important in medical students and that it is important to promote students’ self-efficacy in medical school [22]. Self-efficacy has been examined in a more general context of academic performance in higher education, but it can be assessed in a context-specific manner.
Anatomical self-efficacy, specifically, is defined as a student’s judgment of their ability to execute anatomical tasks and is a validated predictor of student academic performance in medical school [23]. Burgoon [24] developed and validated an instrument to measure anatomical self-efficacy of students enrolled in medical gross anatomy, and it was found that anatomical self-efficacy was predictive of examination scores in the course. Additionally, female students tended to have significantly lower levels of anatomical self-efficacy than their male peers [24]. This puts female students at risk of lower academic performance and may increase their likelihood of feeling academic burnout. When addressing the relationship between self-efficacy and burnout, one study found that surgical trainees within the highest quartile of burnout had a significant decrease in their self-efficacy [9]. Considering these trends, it is possible that self-efficacy, as it pertains to gross anatomy, may affect students’ feelings of burnout, or vice versa, students’ feelings of burnout may affect their anatomical self-efficacy.
Study Aims
This study aimed to ascertain if there is a relationship between first-year medical students’ anatomical self-efficacy and feelings of burnout. Specifically, this study measured students’ feelings of burnout and anatomical self-efficacy at the beginning, middle, and end of the semester in which they were enrolled in gross anatomy, tracking changes in each over the course of the semester in addition to examining associations between anatomical self-efficacy and burnout.
Methods
Context
The University of Mississippi Medical Center (UMMC) is a large academic health center that focuses on educating future health care providers across multiple disciplines. The UMMC School of Medicine is Mississippi’s only allopathic medical program and only admits state residents. The curriculum follows a traditional structure of 2 years of basic science education followed by 2 years of clinical clerkships. At the time of this study, first-year medical students were in their first semester of medical school and enrolled in Histology and Cell Biology, Biochemistry, Introduction to the Medical Profession, and Gross and Developmental Anatomy.
Gross and Developmental Anatomy was taught as a stand-alone course throughout the entirety of the fall semester. The course consisted of lectures, laboratory sessions, and self-study modules (SSMs). Laboratory sessions were mandatory for students to attend and consisted of 3-h long cadaveric dissections. Anatomy faculty and two graduate assistant teachers were available during these sessions to answer questions and help with dissections when necessary. SSMs were utilized by students at their own pace and specifically covered the embryology component of the course. SSMs were comprised of PowerPoint presentations that covered the developmental principles from gametogenesis to birth, clinical considerations, and provided practice examination questions.
The course was divided into four blocks: back and upper limb, thorax and abdomen, pelvis and lower limb, and finally, head and neck. At the end of each block, students took a 100-question multiple-choice examination consisting of roughly sixty-five gross anatomy and thirty-five embryology questions, as well as a fifty-seven free-response question laboratory practical examination. In addition to the examinations, students were assessed with four radiology quizzes, four ultrasound quizzes, fourteen embryology quizzes, and eight oral lab quizzes that were dispersed throughout the semester.
Instruments
Two instruments were used in this study, OLBI-SS and the ASEI. There are several existing measures for assessing burnout, and the choice to use the OLBI-SS was multifaceted. The original OLBI is a validated instrument for measuring burnout that measures two subscales that contribute to an individual’s feelings of burnout: exhaustion and disengagement [25, 26]. Additionally, it is well suited to measure both physical and cognitive aspects of exhaustion [25], and it has undergone revisions to assess burnout in students, the OLBI-SS [27, 28]. The OLBI-SS uses both positively and negatively worded questions, which more accurately measures these traits being assessed, and it forces students to pay closer attention to how they are answering their questions, increasing reliability [25]. The OLBI-SS can be used to measure either burnout or disengagement. When assessing burnout, positively worded items should be reverse coded; and when assessing disengagement, negatively worded items should be reverse coded [25]. Additionally, Janko and Smeds [9] set a precedent of using the OLBI when investigating potential relationships between burnout and self-efficacy in medical trainees. The ASEI is a validated instrument for measuring anatomical self-efficacy [24]. Both, the OLBI-SS and ASEI include Likert-type scale items consisting of sixteen questions each. The OLBI-SS items include four possible response choices, in which 1 is strongly agree, and 4 is strongly disagree. The ASEI items include five possible response choices, in which 1 is not at all confident, and 5 is totally confident.
Questionnaire Administration
First-year medical students at UMMC (n = 172) were invited to participate in the present study before their first lecture on Gross and Developmental Anatomy in the 2019 fall semester. They were provided a packet containing an informational letter, demographic information survey, OLBI-SS and the ASEI. The demographic questionnaire collected information regarding each student’s race/ethnicity, sex, gender identity, sexual orientation, age, marital status, undergraduate major, undergraduate grade point average (GPA), and highest-level degree previously earned. To capture any changes in their feelings of burnout and/or anatomical self-efficacy throughout the semester, the OLBI-SS and ASEI were given to students again at the halfway point and end of the course.
In order to maintain student anonymity, but still allow for tracking of individual participant responses throughout the semester, each student created a unique ID code using the prompt provided in the questionnaire packet. A sample ID was provided in the instructions to further clarify the ID structure. This prompt generated unique ID codes for each student and was provided at all three measurement points, so participants did not have to remember the ID code from measurement to measurement.
Statistical Analyses
Prior to analyses, responses to the eight positively worded questions on the OLBI-SS were reverse coded. This is done to accurately assess feelings of burnout [25], as well as adapting each item to have a similar directionality [29]. Doing so produces responses in which lower scores represent elevated feelings of exhaustion and disengagement. An individual’s overall score on the OLBI-SS is discussed as a sum of the responses on the questionnaire, with a maximum score of 64. Additionally, lower sums on the OLBI-SS are interpreted as elevated feelings of burnout as they represent lowered levels of “vigor” and “dedication” [25]. If a student failed to answer a question on the ASEI but responded to at least twelve of the sixteen items, the omitted response(s) was filled in with the mean of their other responses. This is in line with the procedure used by Burgoon [24]. An individual’s ASEI overall score is discussed as a mean of all responses on the questionnaire.
Basic descriptive statistics of demographic information were conducted at the first measurement point. Basic descriptive statistics were also conducted for the academic information collected at the first measurement point. Due to the large numbers of undergraduate majors listed, similar majors were grouped and relabeled. One example includes “biology, biological science, and biomedical science,” which were grouped under “Biological Sciences.” Similarly, responses of “biomedical engineering, biological engineering, and biology engineering” were grouped under “Biomedical Engineering.”
Descriptive statistics and correlations between burnout and anatomical self-efficacy were examined at each of the three measurement points. Repeated measures ANOVAs were conducted to determine any changes in feelings of overall burnout, the OLBI-SS subscales of exhaustion and disengagement, and anatomical self-efficacy over the duration of the semester. Repeated measures ANOVAs were conducted on individual ASEI items to determine any changes in self-efficacy for specific anatomical tasks. Linear regressions were conducted to assess the predictive relationship between feelings of burnout and anatomical self-efficacy.
Students were excluded from the analyses if they did not respond to all three measurement points, were unable to correctly recreate their ID code at a measurement point, did not complete both instruments, and/or did not answer at least twelve of the sixteen items on the ASEI at a particular measurement point. Additionally, correlational statistics were used to determine if any demographic variables of the students were related to feelings of burnout or anatomical self-efficacy at any measurement point. All statistical analyses were completed using SPSS version 27 (IBM Inc., Armonk, NY) and set to a significance level of α = 0.05.
Results
Demographic and Academic Information
Of the 172 first-year medical students, 87 (50.6%) completed the questionnaires at all three measurement points. Table 1 displays the results of the demographic information. Additionally, the mean age of the respondents was 23.2 (SD = 2.126) years, with a maximum of 35 and a minimum of 21. The participants had a mean MCAT score of 503.83 (SD = 4.854), with a maximum of 514 and a minimum of 492. Students were asked to report biological sex, as well as gender identity. There were no differences between sex and gender reported, so to simplify the results, only statistics regarding sex will be described.
Burnout and Anatomical Self-efficacy
When examining the 87 students who could be followed through the duration of the study, mean burnout scores were 41.16, 38.55, and 38.29 at the beginning, middle, and end of the semester, respectively. Repeated measures ANOVA assessing these changes in mean burnout scores throughout the semester revealed statistically significant differences between the mean burnout score at the early and mid-measurement points (p < 0.001), as well as the early and late measurement points (p < 0.001) (Fig. 1). The means for individual OLBI-SS items, as well as the disengagement and exhaustion subscales mean scores, are displayed in Table 2. For both subscales, repeated measures ANOVAs revealed statistically significant changes between the beginning of the course and the two follow-up measurement points (p < 0.05). At the early semester measurement, male students reported lower feelings of burnout (M = 42.77, SE = 0.85) than female students (M = 39.59, SE = 0.96), with a mean difference of 3.18, t(85) = −2.475, 95% CI [−5.73, − 0.65], p = 0.015, and again, at the late semester measurement point, male students reported lower feelings of burnout (M = 39.79, SE = 0.96) than female students (M = 36.82, SE = 1.06) with a mean difference of 2.97, t(85) = − 2.067, 95% CI [− 5.83, − 0.11], p = 0.042. Additionally, at the late semester measurement, there was a significant relationship between marital status and burnout, with married students having lower levels of burnout than their single peers F (2, 84) = 3.15, p = 0.048, ω = 0.22.

Changes in overall mean OLBI-SS scores from the beginning, middle, and end of the course for students who completed the questionnaires at all three measurement points. Repeated measures ANOVAs determined statistical changes between the beginning and middle measurement point, as well as the beginning and end measurement point
The mean scores for anatomical self-efficacy at the early, mid, and late measurements were 3.38, 3.39, and 3.44, respectively (Fig. 2). Repeated measures ANOVAs did not show any significant differences in mean anatomical self-efficacy scores between any measurement points. No demographic nor academic variables collected had a statistically significant relationship with any anatomical self-efficacy scores. Additional repeated measures ANOVAs found that certain items on the ASEI changed significantly. The findings for each ASEI item are displayed in Table 3.

Changes in overall mean ASEI scores from the beginning, middle, and end of the course. Repeated measures ANOVAs found no statistical changes between any measurement points
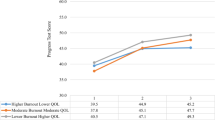
Linear regression revealed a significant predictive relationship between mean burnout and anatomical self-efficacy scores at all three measurements (p < 0.001) as displayed in Fig. 3.

The relationship between burnout and anatomical self-efficacy at the beginning, middle, and end of the semester. Linear regression at all three measurements demonstrates a significant, negative relationship between anatomical self-efficacy and burnout (p < 0.001). Lower scores on the OLBI-SS represent higher levels of burnout, while lower scores on the ASEI represent lower feelings of anatomical self-efficacy. R2 values reveal that 14.25%, 24.21%, and 25.91% of the variation in the scores are caused by each other at the first, middle, and end measurement points, respectively
Discussion
One of the study aims was to determine if students’ feelings of burnout changed throughout the semester in which they are enrolled in gross anatomy. Repeated measures ANOVAs revealed that first-year medical students at UMMC experienced significant changes in their feelings of burnout from the beginning of their gross anatomy course and the middle of the course, as well as the beginning and end of the course. The reported sums on the OLBI-SS decreased, corresponding to overall increased feelings of burnout. Their feelings of burnout did not significantly change between the middle of the course and the end of the course. A similar pattern was observed when looking specifically at the subscales of exhaustion and disengagement, where there was no significant change in either subscale between the middle and end of the course. This plateau of exhaustion and disengagement (and overall burnout) could be the result of students adjusting to the demands of medical school. Including qualitative assessment in future studies may be useful for explaining why these student burnout plateaus occurred toward the end of the semester.
At the beginning and end of the course, male students reported significantly lower feelings of burnout than female students. These findings align with the results of a study by Altannir et al. [13], which found that female students experienced significantly lower feelings of personal accomplishment and increased feelings of burnout compared to their male counterparts. In contrast, Cecil et al. [6] and Ilic et al. [14] found that male students were at higher risk of burnout, and other studies have found no gender disparities for increased risk of burnout [4, 7, 9]. One explanation for the inconsistent findings within the literature may come down to culture. Altannir et al. [13] attribute the culture and religion of their students to be a major contributor to their student’s feelings of burnout. Cecil et al. [6] suggest that male students may be more susceptible to depersonalization to explain their findings that male students are at higher risk of burnout. The mixed findings suggest that additional contextual factors are important in influencing the correlation between sex and burnout.
An interesting finding is that at the end of the semester married students had significantly lower feelings of burnout compared to their single peers. One explanation for this could be the additional support system that one can find in their spouse. When comparing the mental health of married and unmarried individuals, the social support system of unmarried people is less able to protect them the same way as married individuals [30]. It appears that marriage is not only an additional support system, but it is unique and difficult to recreate with other social support systems. However, the quality of the marriage does play a key role in this protective effect [30]. A review by Kiecolt-Glaser and Newton [31] highlights how the quality of a marriage, specifically, is important for improving a person’s quality of life, as they found marital happiness to be the strongest contributor to global happiness and health benefits. This seems to be a protective factor not only for burnout but comorbidities associated with a burnout like suicidal ideation and depression. Dyrbye et al. [3] reported that medical students and professionals who are married were less likely to have recent suicidal ideation. Male residents and early career physicians who were married were also less likely to have symptoms of depression [3].
Another aim of this study was to determine if students’ feelings of anatomical self-efficacy changed throughout the semester in which they were enrolled in gross anatomy. The analysis showed that it did not change in a statistically significant manner. While their overall scores on the ASEI gradually increased, this does not tell the whole story. Item breakdown of the ASEI found that students felt significantly more confident in their abilities to follow the lab manual, use dissection tools, complete dissections, and pronounce anatomical terminology. This is consistent with what researchers expect of students who have repeated participation/exposure to a task, as persistence is a contributing factor to self-efficacy [19]. Burgoon et al. [23] comment on how students who more actively participate in dissection acquire more proficiency in these skills and gain more information about anatomical relationships. This study did not assess the extent to which students participated in dissection; however, students had numerous opportunities to participate in dissection by the end of the semester. This repeated exposure and participation in dissection is a logical explanation for the increased feelings of self-efficacy for these tasks. It also points to the importance of engaging students in laboratory activities for them to actually reap the benefits of said activities.
Item analysis of the ASEI also showed that students felt significantly less confident in their abilities to retain and recall anatomical knowledge for use in clinical settings (item 15). This is concerning since medical students are expected to have a strong understanding of anatomy in their clinical years and residencies. Previous research found that the majority of residency program directors felt that their residents were not adequately prepared in particular anatomical areas [32]. More specifically, 41% of residency program directors felt that their residents were underprepared in “general anatomical knowledge” and 18.1% of program directors felt that their residents were either poorly or very poorly prepared in their anatomical knowledge upon entering residency [32]. Students in the present study only felt “fairly confident” that they would be able to answer anatomy-based questions in their clinical rotations. This should be of great importance to anatomy educators. It is the duty of medical anatomy educators to not only convey anatomical knowledge to their students but to prepare them to use the knowledge gained in a clinical setting.
Additionally, medical students consistently scored the lowest on their confidence in their ability to successfully answer questions during dissection laboratories. While not statistically significant, it is still useful for instructors to see that their confidence rating was lower at the end of the course than it was at the beginning. Students may feel they do not have the time to think about the anatomy while they are dissecting and just want to complete their tasks. This would explain their feelings of not being able to answer questions in laboratory sessions. Anecdotal experiences from working with medical students support this claim; however, further investigation would be beneficial to confirm this proposal. Anatomy instructors can tackle the issues of students feeling little confidence in their ability to use anatomical knowledge in a clinical setting and in their ability to answer questions in the dissection lab through intentional course design. For example, Lazarus et al. [33] incorporated anatomically adapted versions of a clinical Situation, Background, Assessment, and Recommendation (SBAR) handoff oral report in their medical gross anatomy dissection lab. Students felt that the SBARs were useful and promoted deeper learning of anatomy [33]. This link suggests that incorporating adapted clinical reporting improves students’ ability to use anatomy knowledge in a clinical setting [33]. Anatomy laboratories are well suited to implementing such activities to enhance the learning experience.
At the end of the course, one of the least confident tasks students reported was in their ability to be successful on laboratory practical examinations. This could be explained by a variety of factors, such as the fact that the final examination is on head and neck anatomy, often regarded as one of the more difficult body regions. It is also possible that students do not feel that the course content is adequately preparing them for the laboratory practical examinations. A factor felt by faculty and students at this point in the semester is increased fatigue, as the fall semester is quite intense. Additionally, at the end of the course, students were not only studying for the final gross anatomy block examination but were also studying for a comprehensive NBME Biochemistry board examination, a histology lecture and laboratory examination, and a comprehensive NBME Gross Anatomy and Embryology board examination.
Another potential factor affecting student burnout and anatomical self-efficacy is the frequent exposure to cadaveric tissue and body donors. Gross anatomy may be a student’s first experience with death and the emotional toll of navigating the topic of dying, and entering a dissection room can be challenging for some students [34]. Allison et al. [35] found that medical students with increased fear of death had significantly lower performance on gross anatomy laboratory practical examinations. The authors speculate that students with increased fear of death may avoid active participation in class or avoid spending time studying in the gross anatomy lab outside of scheduled class sessions. Students who avoid participation in the dissection lab due to increased fear of death may subsequently have lower anatomical self-efficacy than students with a lower fear of death. Students with increased fear of death compared to their peers may be at a higher risk of burnout due to consistent exposure to an environment that they find unwelcoming. While this link was not directly investigated, this explanation seems likely given that the participants from Allison et al. [35] were the same as the participants in the current study. Future research could investigate both of these lines of inquiry to establish if there is a link between fear of death and anatomical self-efficacy or burnout.
The final aim, and one of most interest, of this study was to establish if there is an association between anatomical self-efficacy and burnout, and linear regression revealed that a predictive, negative relationship exists. As feelings of burnout increased (OLBI-SS score decreased), feelings of anatomical self-efficacy decreased, and this relationship was present at all measurement points. This relationship is similar to the findings of Janko and Smeds [9] that surgical residents with the most burnout had the lowest levels of self-efficacy. Koeske and Koeske [36] suggest interventions to moderate an individual’s self-efficacy may improve one’s feelings of burnout. In examining this relationship between anatomical self-efficacy and burnout, it was a bit unexpected to find some demographic variables had statistically significant associations with burnout but not anatomical self-efficacy. It is possible there are other context-specific factors that were not examined that explain the lack of correlations between demographic variables and anatomical self-efficacy.
Limitations
There are some limitations of the current study that future research could improve upon. One limitation is the relatively small sample size of 87. Despite a response rate of 50.6%, this study only collected data from one medical class at one medical institution. Expanding to multiple institutions would provide a larger, more diverse pool of participants with different experiences that may or may not affect their anatomical self-efficacy and/or burnout, and results would be more generalizable to US medical students. No incentives were offered to students, and including participant incentives in the future could also bolster response rates. Questionnaires were distributed to students during mandatory clinical-correlation lectures in an effort to maximize the response rate. Additional plans for longitudinal analysis at the institution in the present study were disrupted due to the COVID-19 pandemic. Initially, the study aimed to also collect data from the first-year medical students entering medical school in 2020. In an effort to teach in a socially distant manner, the Gross and Developmental Anatomy course structure was altered significantly. Substantial alterations to the ASEI would have been necessary, and comparisons between cohorts would not be reasonable. Future research investigating burnout may also desire to use a mixed-methods design to include qualitative data, like that of Song [18]. Qualitative data provides a level of richness that cannot be obtained with solely qualitative data [37, 38] and could provide further insight into the experiences that affect students’ feelings of anatomical self-efficacy and burnout.
Conclusions
Given the current study’s findings and past research, it seems reasonable to suggest that a student’s anatomical self-efficacy is one of the contributors to their feelings of academic burnout. Educators should consider engaging students in a way that increases their feelings of anatomical self-efficacy, particularly with answering faculty questions during laboratory settings and applying anatomical knowledge to clinical settings. For example, instructors could take a scaffolding approach by which instructors initially model the thought process for answering such questions and applying foundational anatomical knowledge, then gradually asking the students to do the same with increasing independence (i.e., less guidance from instructors) as the course proceeds. Such tasks are asking students to reach higher levels of thinking by applying the knowledge they have learned, which is difficult to do early in the course and particularly in the first semester of medical school. A scaffolded approach would provide students with more guidance and feedback to hone their skills, increase their confidence and learning of skills and content in anatomy. Self-efficacy can also be promoted, generally or in anatomy, through shaping a classroom environment that helps students attribute their success or failure to effort instead of innate ability. Anatomy educators can provide opportunities and feedback in the laboratory setting with the aim of boosting students’ beliefs that they can successfully carry out laboratory-related tasks. Future studies to determine if implementing sessions designed to improve student anatomical self-efficacy is effective in reducing feelings of burnout would be beneficial to anatomy educators and medical educators more broadly.
Availability of Data and Material
Not applicable.
References
Dyrbye LN, Thomas MR, Massie FS; Power, Power DV, Eacker A, Harper W; Durning S, Moutier C, Szydlo DW, Novotny PJ, Sloan JA, Shanafelt TD. Burnout and suicidal ideation among U.S. medical students. Ann Intern Med. 2008. https://doi.org/10.7326/0003-4819-149-5-200809020-00008.
Guthrie EA, Black D, Shaw CM, Hamilton J, Creed FH, Tomenson B. Psychological stress in medical students: a comparison of two very different university courses. Stress Medicine. 1997. https://doi.org/10.1002/(SICI)1099-1700(199707)13:3<179::AID-SMI740>3.0.CO;2-E.
Dyrbye LN, West CP, Satele D, Boone S, Tan L, Sloan J, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014. https://doi.org/10.1097/ACM.0000000000000134.
Galán F, Sanmartín A, Polo J, Giner L. Burnout risk in medical students in Spain using the Maslach Burnout Inventory-Student Survey. Int Arch Occ Env Hea. 2011. https://doi.org/10.1007/s00420-011-0623-x.
Zalaquett CP, Wood RJ. Evaluating stress. Scarecrow Press; 1997.
Cecil J, McHale C, Hart J, Laidlaw A. Behaviour and burnout in medical students. Med Educ Online. 2014. https://doi.org/10.3402/meo.v19.25209.
Galán F, Ríos-Santos J-V, Polo J, Rios-Carrasco B, Bullón P. Burnout, depression and suicidal ideation in dental students. Med Oral Patol Oral Cir Bucal. 2014. https://doi.org/10.4317/medoral.19281.
Prinz P, Hertrich K, Hirschfelder U, de Zwaan M. Burnout, depression and depersonalisation–psychological factors and coping strategies in dental and medical students. GMS J Med Educ. 2012. https://doi.org/10.3205/zma000780.
Janko MR, Smeds MR. Burnout, depression, perceived stress, and self-efficacy in vascular surgery trainees. J Vasc Surg. 2019. https://doi.org/10.1016/j.jvs.2018.07.034.
Dahlin ME, Runeson B. Burnout and psychiatric morbidity among medical students entering clinical training: a three year prospective questionnaire and interview-based study. BMC Med Educ. 2007. https://doi.org/10.1186/1472-6920-7-6.
Dyrbye LN, Massie FS, Eacker A, Harper W, Power D, Durning SJ, et al. Relationship between burnout and professional conduct and attitudes among US medical students. JAMA. 2010. https://doi.org/10.1001/jama.2010.1318.
Kim B, Jee S, Lee J, An S, Lee SM. Relationships between social support and student burnout: a meta-analytic approach. Stress Health. 2018. https://doi.org/10.1002/smi.2771.
Altannir Y, Alnajjar W, Ahmad SO, Altannir M, Yousuf F, Obeidat A, et al. Assessment of burnout in medical undergraduate students in Riyadh. Saudi Arabia BMC Med Educ. 2019. https://doi.org/10.1186/s12909-019-1468-3.
Ilic I, Zivanovic Macuzic I, Kocic S, Ilic M. High risk of burnout in medical students in Serbia, by gender: a cross-sectional study. PLoS One. 2021. https://doi.org/10.1371/journal.pone.0256446.
Cook AF, Arora VM, Rasinski KA, Curlin FA, Yoon JD. The prevalence of medical student mistreatment and its association with burnout. Acad Med. 2014. https://doi.org/10.1097/ACM.0000000000000204.
Villwock JA, Sobin LB, Koester LA, Harris TM. Impostor syndrome and burnout among American medical students: a pilot study. Int J Med Educ. 2016. https://doi.org/10.5116/ijme.5801.eac4.
Carson AJ, Dias S, Johnston A, McLoughlin MA, O’Connor M, Robinson BL, Sellar RS, Trewavas JJC. Mental health in medical students a case control study using the 60 item General Health Questionnaire. Scot Med J. 2000. https://doi.org/10.1177/003693300004500406.
Song YK. “This isn’t being a doctor.”-Qualitative inquiry into the existential dimensions of medical student burnout. Med Sci Educ. 2020. https://doi.org/10.1007/s40670-020-01020-0.
Bandura A. Social foundations of thought and action: a social cognitive theory. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs, NJ, US: Prentice-Hall, Inc; 1986.
Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. 1993. https://doi.org/10.1207/s15326985ep2802_3.
Fazey DMA, Fazey JA. The potential for autonomy in learning: perceptions of competence, motivation and locus of control in first-year undergraduate students. Stud High Educ. 2001. https://doi.org/10.1080/03075070120076309.
Zheng B, Chang C, Lin C-H, Zhang Y. Self-efficacy, academic motivation, and self-regulation: how do they predict academic achievement for medical students? Med Sci Educ. 2021. https://doi.org/10.1007/s40670-020-01143-4.
Burgoon JM, Meece JL, Granger NA. Self-efficacy’s influence on student academic achievement in the medical anatomy curriculum. Anat Sci Educ. 2012. https://doi.org/10.1002/ase.1283.
Burgoon JM. An investigation of the self-efficacy of medical students for the anatomy curriculum: role of gender and prior experience, and self-efficacy’s influence on academic achievement. 2008.
Demerouti E, Bakker AB. The Oldenburg Burnout Inventory: a good alternative to measure burnout and engagement. Handbook of stress and burnout in health care. 2008:65–78.
Demerouti E, Mostert K, Bakker AB. Burnout and work engagement: a thorough investigation of the independency of both constructs. J Occup Health Psych. 2010. https://doi.org/10.1037/a0019408.
Maroco J, Campos JADB. Defining the student burnout construct: a structural analysis from three burnout inventories. Psychol Rep. 2012. https://doi.org/10.2466/14.10.20.PR0.111.6.814-830.
Reis D, Xanthopoulou D, Tsaousis I. Measuring job and academic burnout with the Oldenburg Burnout Inventory (OLBI): factorial invariance across samples and countries. Burn Res. 2015. https://doi.org/10.1016/j.burn.2014.11.001.
Campos JADB, Carlotto MS, Marôco J. Oldenburg Burnout Inventory-student version: cultural adaptation and validation into Portuguese. Psicol-Refle Crítica. 2012. https://doi.org/10.1590/S0102-79722012000400010.
Holt-Lunstad J, Birmingham W, Jones BQ. Is there something unique about marriage? The relative impact of marital status, relationship quality, and network social support on ambulatory blood pressure and mental health. Ann Behav Med. 2008. https://doi.org/10.1007/s12160-008-9018-y.
Kiecolt-Glaser JK, Newton TL. Marriage and health: his and hers. Psychol Bull. 2001. https://doi.org/10.1037/0033-2909.127.4.472.
Fillmore EP, Brokaw JJ, Kochhar K, Nalin PM. Understanding the current anatomical competence landscape: comparing perceptions of program directors, residents, and fourth-year medical students. Anat Sci Educ. 2016. https://doi.org/10.1002/ase.1578.
Lazarus MD, Dos Santos JA, Haidet PM, Whitcomb TL. Practicing handoffs early: applying a clinical framework in the anatomy laboratory. Anat Sci Educ. 2016. https://doi.org/10.1002/ase.1595.
Romo-Barrientos C, Criado-Álvarez JJ, González-González J, Ubeda-Bañon I, Flores-Cuadrado A, Saiz-Sánchez D, et al. Anxiety levels among health sciences students during their first visit to the dissection room. BMC Med Educ. 2020. https://doi.org/10.1186/s12909-020-02027-2.
Allison S, Notebaert A, Perkins E, Conway M, Dehon E. Fear of death and examination performance in a medical gross anatomy course with cadaveric dissection. Anat Sci Educ. 2021. https://doi.org/10.1002/ase.2092.
Koeske GF, Koeske RD. Work load and burnout: can social support and perceived accomplishment Help? Soc Work. 1989;34(3):243–8.
Nayar S, Stanley M. Qualitative research methodologies for occupational science and therapy. Routledge; 2014.
Stalmeijer RE, McNaughton N, Van Mook WNKA. Using focus groups in medical education research: AMEE Guide No. 91. Med Teach. 2014. https://doi.org/10.3109/0142159X.2014.917165.
Acknowledgements
The authors would like to thank Ellen Robertson, Ph.D., for her assistance with the statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
This study was approved by the University of Mississippi Medical Center Internal Review Board.
Consent to Participate
All participants voluntarily consented to participate in this study.
Consent for Publication
All participants were informed and consented to the publication of study findings.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ferriby, A., Schaefer, A.F. The Relationship Between Anatomical Self-efficacy and Feelings of Burnout in First-year Medical Students. Med.Sci.Educ. 32, 437–446 (2022). https://doi.org/10.1007/s40670-022-01511-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40670-022-01511-2