
Abstract
Purpose of Review
Leishmaniasis is a leading cause of parasitic death, with incidence rising from decreased resources to administer insecticide and anti-leishmanial treatments due to the COVID-19 pandemic. Leishmaniasis is nonendemic in the United States (U.S.), but enzootic canine populations and potentially competent vectors warrant monitoring of autochthonous disease as a fluctuating climate facilitates vector expansion. Recent studies concerning sand fly distribution and vector capacity were assessed for implications of autochthonous transmission within the U.S.
Recent Findings
Climate change and insecticide resistance provide challenges in sand fly control. While most Leishmania-infected dogs in the U.S. were infected via vertical transmission or were imported, autochthonous vector-borne cases were reported. Autochthonous vector-borne human cases have been reported in four states. Further vaccine research could contribute to infection control.
Summary
Both cutaneous and visceral leishmaniasis cases in the U.S. are increasingly reported. Prevention measures including vector control and responsible animal breeding are critical to halt this zoonotic disease.
Similar content being viewed by others


Introduction
Leishmaniasis is a worldwide neglected tropical disease that affects between 700,000 and 1 million people per year [1]. In the Americas, the Pan American Health Organization (PAHO) reports an average of 53,387 cutaneous leishmaniasis (CL) cases per year and an average of 3400 visceral leishmaniasis (VL) cases per year, both largely occurring in Brazil [2]. While many CL cases were considered cured, VL had an approximate 8% case fatality rate in 2020, which varied by country [2]. The COVID-19 pandemic has decreased funding for leishmaniasis programs and negatively affected disease control, impacting surveillance, chemotherapy availability, and residual insecticide spraying programs [3, 4]. These impacts will likely prolong leishmaniasis control and elimination [3].
In endemic areas, Phlebotomus and Lutzomyia sand flies transmit Leishmania protozoal parasites. Dogs are the main reservoir for visceralizing leishmaniosis (CanL), and dogs from over 70 countries have this disease [5]. Other reservoirs for Leishmania spp. include rabbits, hares, rats, and mustelids [6••]. Although documented to occur in endemic areas, Leishmania spp. transmission via vertical transmission is a predominant means of CanL transmission in the United States (U.S.), especially in canine populations [7, 8••, 9]. Vector-borne transmission is the most reported mode of transmission worldwide, and the expanding distribution of Lutzomyia spp. in the Americas heightens risk for autochthonous leishmaniasis cases, in both humans and animals. Monitoring sand fly distributions and incidence of leishmaniasis within the U.S. will provide evidence to institute prevention measures, including effective insecticide treatments, vaccination, and educational campaigns. For nonendemic areas, such as the U.S., previous research emphasized imported cases, but expansion of sand fly distributions has increased autochthonous transmission. This review highlights recent findings concerning the ability of sand flies to vector Leishmania spp. in the U.S. as well as recent human and canine cases, both imported and autochthonous.
Sand Flies as Leishmania Vectors
Leishmaniasis is a vector-borne parasitic disease caused by 20 species of flagellated protozoans of the Leishmania genus [10]. The Leishmania parasite is transmitted between mammalian hosts by female sand flies of the genus Phlebotomus in the Old World and the genus Lutzomyia in the New World [11]. Currently, 93 of the 800 known sand fly species have been incriminated as competent vectors for Leishmania parasites [11]. Confirmed Phlebotomus vectors have been reported in Africa, Asia, the Mediterranean, and the Middle East [11]. Further, Phlebotomus spp. in the Old World can vector Leishmania spp. that cause VL, CL, and mucocutaneous leishmaniasis (MCL) [11]. In the U.S., experts estimate that three sand fly species of the Lutzomyia genus are competent vectors for CL: Lutzomyia anthophora, Lutzomyia diabolica, and Lutzomyia shannoni [12].
Sand Fly Species of Interest in the U.S.
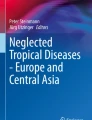
The three Lutzomyia spp. found in multiple U.S. states (Fig. 1) are associated with autochthonous transmission of cutaneous Leishmania infections, principally L. mexicana (Table 1) [13,14,15,16,17,18]. Multiple Lutzomyia species are associated with L. mexicana transmission in North America [19], but transmission dynamics of L. mexicana within the U.S. is still not well understood. Lu. diabolica was considered the probable vector for CL in Texas due to its anthropophagic nature and wide distribution in the state [12]. Lu. anthophora typically prefers to feed on non-human hosts and has thus been disregarded as a vector for Leishmania spp. responsible for human infections [12]. However, a study in Texas found that 98% of the sand flies found within 100 m of the autochthonous CL patients were Lu. anthophora [20•]. Further, two of the 188 Lu. anthophora collected had human DNA within them [20•]. This finding suggests that Lu. anthophora was the most likely vector species for CL in the area and that the sand flies had actively fed on humans there [20•]. Recent surveillance efforts to identify local cases of human leishmaniasis identified the human blood that was PCR-positive for L. mexicana within Lu. anthophora specimens, which also suggests that Lu. anthophora is a Leishmania vector species in Texas [20•].

Autochthonous cutaneous Leishmania infections reported in the U.S. and potential sand fly vector locations. aTexas, Oklahoma, and Florida also have found sand fly vectors
Several studies have determined the prevalence of Leishmania infection in sand flies in the U.S. A study published in 2001 found natural Leishmania infection in one of 347 Lu. anthophora sand flies collected from south-central Texas [28], while a 1993 study in San Antonio, Texas identified Leishmania parasites in three of 27 female Lu. anthophora sand flies collected [29]. These studies suggest that there is variability regarding Leishmania burden in Lu. anthophora in Texas. Similar variability in parasitic burden has been documented in Mexico [30, 31]. Research examining the potential role of sand fly vectors in the U.S. has highlighted the abundance of habitable territory for Lu. cruciata, Lu. diabolica, and Lu. shannoni [32–34]. Studies in Ossabaw Island, Georgia, found that Lu. shannoni was established in the area and survived seasonal variability [33, 34]. In addition, studies on U.S. Army bases have indicated risk of leishmaniasis incidence due to compounding factors of competent sand fly vectors, expanding sand fly habitats, and imported leishmaniasis cases in military personnel [32, 35].
Beyond the observations of sand fly habitats in the U.S., research has shown a clear potential for these sand flies to locally transmit Leishmania parasites. For example, Lawyer et al. (1987) established the development of L. mexicana parasites within Lu. diabolica and Lu. shannoni and incriminated both species as potential vectors for L. mexicana [36]. Further, Schaut et al. (2015) found that L. infantum from hunting dogs remained infectious in sand flies, which provided evidence of the risk for human exposure within areas where infected hunting dogs and sand fly populations overlap [23].
In addition to Lu. diabolica and Lu. shannoni, Lu. cruciata has been identified as an important vector for Leishmania transmission. Studies in Mexico have supported the role of Lu. cruciata as an important vector for Leishmania spp. both experimentally and naturally in the environment [30, 37, 38]. Interestingly, although Lu. cruciata is found in Texas, it is more commonly reported in Florida [17]. Increased surveillance is needed to improve our understanding of the distribution and transmission dynamics of Lu. anthophora, Lu. diabolica, Lu. shannoni, and Lu. cruciata to prevent and monitor the increased transmission of Leishmania in the U.S.
Insecticides and Sand Flies
Insecticide resistance remains a significant challenge to the success of sand fly control. For example, a recent study by Denlinger et al. (2015) evaluated the insecticide susceptibility of Lu. longipalpis and P. papatasi in a laboratory setting [39]. The authors found that Lu. longipalpis and P. papatasi were most susceptible to carbamates bendiocarb and propoxur as well as the organophosphate fenitrothion [39], but Lu. longipalpis and P. papatasi were least susceptible to DDT [39].
Notably, while using a CDC bottle bioassay, Denlinger et al. (2016) established diagnostic doses and times for the phlebotomine sand flies [40]. Both Lu. longipalpis and P. papatasi were highly susceptible to carbamates and more resistant to DDT’s insecticide effects [39]. However, little is known about how carbamates and DDT-based insecticides would impact sand fly species in the U.S.
Novel topical insecticide formulations have proven effective for preventing sand fly bites and, in turn, canine Leishmania infections [41]. Deltamethrin-impregnated collars have an estimated maximum efficacy of 2 weeks [41]. Collars impregnated with fulmethrin and imidacloprid have effectively protected puppies in hyperendemic areas of southern Italy [41]. Spot-on topicals that use permethrin and imidacloprid in combination have been notably efficacious at protecting canine health by repelling sand flies [41]. Recently, topical treatments that use dinotefuran, permethrin, and pyriproxyfen in combination or permethrin and fipronil in combination were 96% efficacious at repelling and 88% efficacious at killing sand flies for 21 days [41]. Finally, insecticide lotions that use permethrin or pyriproxyfen provide effective sand fly protection [41]. Various insecticides are efficacious either in isolation or combination, although, more research is needed to identify the emergence of insecticide resistance among U.S. sand flies.
Potential Impact of Climate Change on Leishmaniasis in the USA
Sand fly development is significantly affected by ambient temperatures and subsequently changes in climate conditions [42]. As the climate changes, it is expected to impact vector distributions around the world. In turn, vector-borne disease distributions will change. Currently, scientists estimate that the world’s temperature will increase by more than 1.5℃ between 2030 and 2052 [42,43,44]. Typically, sand fly vectors require temperatures as high as 20–26℃ to develop and sustain life [42, 44]. Thus, extreme freezing events may inhibit sand fly survival and distributions. Conversely, increased temperatures may allow sand fly vectors to move progressively northward [12]. Current ecological niche models focused on Lu. anthophora and Lu. diabolica in North America included risk factors such as habitat availability, dispersal ability, and the number of people at risk for leishmaniasis [17, 44]. These models predict that the risk of leishmaniasis will spread beyond the current range of the southern U.S. to as far north as Michigan [17]. The geographic distribution of Lu. longipalpis could spread beyond its current range of southern Mexico into southern Texas and Louisiana [45]. Therefore, it is essential to monitor the sand fly distribution as the climate continues to change.
Xenodiagnoses from Vertically Infected Dogs
The risk of Lu. longipalpis range expansion is just one of several plausible concerns for future Leishmania spp. transmission in the U.S. Schaut et al. (2015) demonstrated the ability of sand flies to become infected with the Leishmania parasite from vertically infected dogs in the U.S. [22], which suggests that Leishmania transmission from infected dogs is possible. More recently, Scorza et al. (2021) demonstrated that this population of hunting dogs has an abundant dermal parasite burden and that subclinical animals transmitted Leishmania parasites during xenodiagnoses to Lu. longipalpis [46••]. Lu. longipalpis ingested parasites from the skin of dogs with mild to moderate clinical disease [46••], which suggests that healthy-appearing, vertically infected dogs can transmit parasites to sand flies and propagate emergence of L. infantum in locations where Lu. longipalpis or other competent vector species were present [46••]. Therefore, clinicians, public health practitioners, and scientists must remain mindful of the impact of subclinical dogs on maintaining Leishmania parasites in the environment, particularly in non-endemic areas where Lu. longipalpis may gain an ecological foothold with a changing climate.
Interrupted Feeding Increases Burden of Leishmania Parasites
Given the potential propagation effect of sand flies feeding on infected hosts, preventing multiple blood meals could vastly decrease parasite burden for vectored transmission in the U.S. Researchers have found that sequential blood meals increased Leishmania parasite replication due to interrupted feeding within the sand fly vector [47]. During the time an interrupted sand fly seeks a second blood meal, it has rapidly expanding numbers of parasites within its midgut. Serafim et al. (2018) found that when sand flies took a second blood meal from an uninfected host, Leishmania parasite load was 125-fold greater than from sand flies that consumed just one blood meal [47]. Consequently, a sand fly that feeds on an infected human or canine host followed by a secondary noninfected host could significantly increase the parasitic burden within the sand fly. The likelihood of interrupted sand fly blood feeding in the wild is high. Therefore, while the burden of human leishmaniasis in the U.S. may remain low, the risk of parasite amplification could be much greater than previously understood based on single blood meal studies.
Disease Manifestations and Implications
Canine Vertical Transmission
Canine leishmaniosis (CanL), the visceral form of Leishmania spp. disease, is caused predominantly by Leishmania infantum. Notably, CanL is principally manifested as dermatopathies, especially in earlier stages of disease [48]. Canine cutaneous leishmaniosis can be caused by a variety of Leishmania spp. and vectored by different sand fly species depending on the geographic location. In the U.S., vertical transmission is the primary mode for transmission of autochthonous L. infantum CanL. In 2011, Boggiatto et al. found 10/12 naturally infected neonatal puppies with L. infantum parasites in their organs [7]. Vida et al. (2016) followed three remaining puppies from the Boggiatto et al. (2011) litter after whelping from an infected bitch, who was oligosymptomatic [9]. These dogs were tested for parasite load and immunologic response every 6 months for 6 years to assess progression of disease [9]. One dog was oligosymptomatic and had a positive antibody titer and intermittent qPCR positivity [9]. The second dog was asymptomatic, had positive antibody titers, and had a strong CD4+ T cell response [9]. The third dog was considered healthy [9]. All three dogs had either positive qPCR or IFAT and had CD4+ T cell proliferation and IFN-γ production to L. infantum antigen over the 6-year follow-up period [9]. This study showed that dogs from an infected bitch had variable responses in disease progression and immunologic response, but each dog had evidence of infection [9].
Toepp et al. (2019) evaluated the risk of offspring being positive for L. infantum during their lifetime if the dams had confirmed L. infantum infection [8••]. The authors found that these dogs had 13.84 times higher risk of being positive for L. infantum during their lifetime compared to dogs born to a diagnostically negative dam from the same kennels [8••]. Based on the data from this study, vertical transmission of L. infantum had a basic reproductive number of 4.16 [8••]. Additionally, 19 of 20 dogs followed until death had confirmed CanL as the cause of death [8••]. This study revealed the significance of L. infantum propagating through generations of dogs. It is essential to prevent breeding of infected dams to prevent further transmission of L. infantum [8••].
Canine Imported and Autochthonous Cases
Dogs are considered the main reservoir species of L. infantum among endemic areas with competent sand flies, such as the Mediterranean Basin, southern Europe, South America, and northern Africa [49]. Sand flies can infect naïve dogs during blood meals, and conversely, infected dogs can transmit parasites to naïve sand flies. Dogs without clinical signs of disease are also infectious to sand flies and thus transmit Leishmania parasites [49]. However, dogs with clinical signs have been shown to be more infectious to sand flies than subclinical dogs, although precise disease scores were not used [49, 50]. There are more infected, subclinical dogs than diseased dogs [51].
In the U.S., infected dogs were imported from Europe hundreds of years ago, and the parasites have persisted largely through vertical transmission [7, 8••, 9, 52]. There are also imported cases from competent sand fly-endemic areas, which have potential to propagate infections via vertical transmission in the U.S. For example, a U.S. Boxer with no travel history but whelped from a dam native to an endemic part of Spain, developed CanL, including granulomatous cutaneous lesions, anemia, hyperglobulinemia, hypoalbuminemia, and lymphadenomegaly [53]. This Boxer was euthanized approximately three years after its CanL diagnosis [53]. Additionally, Gin et al. (2021) found 125 L. infantum-positive dogs in the U.S. and Canada between 2006 and 2019 with at least 60 of these dogs having documented foreign travel to endemic areas [54]. Military working dogs are also at-risk for L. infantum infection; for example, 54/378 dogs evaluated by Seal et al. (2022) were Leishmania-positive, with 44/54 of these dogs having reported travel to or inhabitance in endemic areas [55].
Autochthonous CanL cases have occurred in the U.S. [56] largely due to vertical transmission. Foxhound kennels have reported CanL cases in the U.S. since 1980 [56, 57]. Some autochthonous CanL cases were infected via direct contact from dog bites or fights with an infected dog; the infected dog had evidence of previous importation from endemic areas [56]. Some studies report L. infantum-positive dogs with no recorded foreign travel history and unconfirmed mode of transmission [54, 55].
Besides vertical transmission of L. infantum, there is possibility of future autochthonous canine cases due to bites from infected sand flies within non-endemic regions. Within the U.S., autochthonous CanL cases from a known sand fly transmission of Leishmania parasites have not been reported. However, in controlled laboratory settings, sand flies became infected with L. infantum after biting naturally infected hounds, and they also transmitted L. infantum to hamsters [23]. This controlled laboratory experiment shows potential for L. infantum to be transmitted by a competent sand fly vector if the particular vector was present in natural settings within the U.S. [23].
In contrast to the visceral form (CanL), autochthonous canine cutaneous cases have been reported within the U.S. sand flies in Texas and Mexico have transmitted L. mexicana to dogs and cats (Fig. 1) [58–61]. Additionally, an equine cutaneous case of L. siamensis infection was diagnosed in a Morgan mare in Florida with no international travel history (Fig. 1) [62].
Human Imported and Autochthonous Cases
In humans, imported cases of both cutaneous and visceral forms of leishmaniasis have been reported in the U.S. A traveler was likely infected in southern France and developed VL upon return to the U.S. [63]. This traveler had signs such as fever, splenomegaly, and pancytopenia [63]. Some signs that are reported in human VL cases but rarely in dogs include fever, abdominal pain, and ascites [51]. Travelers returning from Costa Rica and Panama developed CL, caused by L. panamensis or L. braziliensis [64, 65]. One of these patients with L. panamensis infection also traveled to the Florida Keys before visiting Central America [65].
U.S. military members are at risk of leishmaniasis largely due to deployments to competent sand fly-endemic areas, such as Middle Eastern countries [66]. CL is the most common form in the U.S. military with L. major being the most common etiologic agent [66]. Asymptomatic VL is also reported in U.S. military members deployed to Iraq, as Mody et al. (2019) found 39/200 (19.5%) deployers with L. infantum infection [67]. Additionally, military members are at-risk for zoonotic VL especially among canine military units [66].
Human autochthonous CL has been reported in Texas (Fig. 1). A man living in central Texas became infected with L. mexicana and developed dermatologic lesions on his legs persisting for over 1 year [20•]. Kipp et al. (2020) caught sand flies near the patient’s home and found infected sand flies, largely Lutzomyia spp. [20•]. Two men in Oklahoma had CL, although the Leishmania spp. was unconfirmed [13]. McIlwee et al. (2018) reported 41 autochthonous human CL cases from 2006 to 2017 in the U.S. [68••]. Most of these cases were infected with L. mexicana [68••]. A woman in Arizona also had autochthonous CL, but the etiologic species was undetermined after sequencing (Fig. 1) [69]. Interestingly, a 1-year-old boy from North Dakota was infected with L. donovani complex, which caused a focal periocular lesion, and determined to have CL (Fig. 1) [70].
Insights for Vaccination and Prevention
While three vaccines are currently approved and available for dogs in Europe and Brazil [71], there are no licensed vaccines for canine leishmaniosis in the U.S. vaccine effectiveness varies by product [71]. Current vaccines may provide immunoprotection, and the LeishTec®. Vaccine has reduced progression of CanL and mortality [72•]. Toepp et al. (2018) conducted a blinded, controlled field trial with 557 asymptomatic dogs randomized to receive the LeishTec® vaccine or placebo of sterile water [72•]. Asymptomatic dogs that received LeishTec had statistically decreased clinical score (these dogs were 33% less likely to have clinical progression of disease compared to dogs receiving placebo) [72•]. Additionally, asymptomatic dogs less than 6 years old receiving placebo had 3.129 (p = 0.0245) times the risk of mortality during the study period compared to dogs receiving LeishTec® [72•]. Among dogs that became symptomatic for CanL during the study period, there were more dogs from the placebo group that became symptomatic, had progression of disease, and died [72•]. Therefore, this study concluded that dogs considered healthy but infected could benefit from vaccination [72•].
In a follow-up study by Toepp et al. (2018), a safety analysis of the LeishTec® vaccine trial revealed a 3.09% occurrence of mild adverse effects among vaccinated dogs [73]. The authors found that six of the approximate 300 included dogs had severe adverse effects from either the vaccine or placebo, and there was no difference in the number of dogs having severe adverse effects between the two groups [73].
There are no vaccines available for human leishmaniasis. Several vaccine candidates are in preclinical trials, and a few candidates are in clinical trials. Vaccine candidates include killed parasite vaccines, recombinant protein vaccines, DNA vaccines, and chimeric vaccines [74]. Preclinical vaccine candidates assessed in murine models include CRISPR-edited centrin gene knockout strain of L. major (LmCen−/−) and ChimeraT recombinant vaccines [75, 76]. Previously, killed vaccines Leishvaccine and autoclaved L. major (ALM) vaccine reached phase II, although Leishvaccine underperformed in phase III, and the ALM vaccine had limited immunoprotection in phase II [74, 77]. The DNA vaccine ChAD63-KH also reached phase II and has potential for therapeutic uses in addition to prevention [77]. A recombinant vaccine in phase II is Leish-F1, designed for VL protection [74, 77]. Challenges for leishmaniasis vaccines include market profit potential, demand for vaccines, protection against different Leishmania spp., and effectiveness outside of clinical trials [74, 78].
For prevention of CanL in endemic areas or for dogs traveling to endemic areas, there are insecticides and repellents commercially available to deter sand fly bites (such as collar and spot-on formulations) [41]. Regardless of geographic location, Leishmania-positive dogs should not be bred or used as blood donors [41]. Dogs at-risk should be tested for Leishmania infection before being bred [41].
For human leishmaniasis prevention, methods include residual insecticide spraying in households, removal of sand fly breeding habitats, insecticide-treated bed nets or clothing, and controlling animal reservoirs [79].
Conclusions
Within the U.S., there is potential for sand flies to expand their distribution due to climate change [17]. Consequently, CL cases could become more prevalent in the southern states. As Leishmania-infected dogs have experimentally contributed to sand fly transmission of L. infantum [46••], which causes visceralizing disease, there is a risk of potential autochthonous zoonosis in the U.S. Continued vigilance for responsible animal breeding and practice of vector prevention measures is warranted.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
World Health Organization. Leishmaniasis. 2022 Jan 8. Available from: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis.
Pan American Health Organization. Leishmaniasis: epidemiological report of the Americas. No. 10, December 2021. Washington, D.C.: PAHO; 2021. Available from: https://iris.paho.org/handle/10665.2/51742
Le Rutte EA, Coffeng LE, Munoz J, de Vlas SJ. Modelling the impact of COVID-19-related programme interruptions on visceral leishmaniasis in India. Trans R Soc Trop Med Hyg. 2021;115(3):229–35. https://doi.org/10.1093/trstmh/trab012.
Makoni M. New threats to visceral leishmaniasis control. Lancet Microbe. 2021;2(11):e574. https://doi.org/10.1016/S2666-5247(21)00285-8.
Baneth G. Canine Leishmaniosis. In: Strube C, Mehlhorn H, editors. Dog parasites endangering human health. Parasitology Research Monographs. Switzerland: Springer Nature Switzerland AG; 2021 27–43
Bourdeau P, Rowton E, Petersen C. Impact of different Leishmania reservoirs on sand fly transmission: perspectives from xenodiagnosis and other one health observations. Vet Parasitol. 2020;287:109237. https://doi.org/10.1016/j.vetpar.2020.109237. Highlighted a need for more research into the skin parasitism of alternative Leishmania hosts. Presented evidence that dogs and other reservoir animals may limit or lack the skin parasitism to transmit L. donovani to P. argentipes
Boggiatto PM, Gibson-Corley KN, Metz K, Gallup JM, Hostetter JM, Mullin K, et al. Transplacental transmission of Leishmania infantum as a means for continued disease incidence in North America. PLoS Negl Trop Dis. 2011;5(4):e1019. https://doi.org/10.1371/journal.pntd.0001019.
Toepp AJ, Bennett C, Scott B, Senesac R, Oleson JJ, Petersen CA. Maternal Leishmania infantum infection status has significant impact on leishmaniasis in offspring. PLoS Negl Trop Dis. 2019;13(2):e0007058. https://doi.org/10.1371/journal.pntd.0007058. Signified vertical transmission of Leishmania in canines by establishing a relative risk and basic reproductive number
Vida B, Toepp A, Schaut RG, Esch KJ, Juelsgaard R, Shimak RM, et al. Immunologic progression of canine leishmaniosis following vertical transmission in United States dogs. Vet Immunol Immunopathol. 2016;169:34–8. https://doi.org/10.1016/j.vetimm.2015.11.008.
Burza S, Croft SL, Boelaert M. Leishmaniasis. The Lancet. 2018;392(10151):951–70. https://doi.org/10.1016/S0140-6736(18)31204-2.
Pace D. Leishmaniasis. J Infect. 2014;69:S10–8. https://doi.org/10.1016/j.jinf.2014.07.016.
Curtin JM, Aronson NE. Leishmaniasis in the United States: emerging issues in a region of low endemicity. Microorganisms. 2021;9(3):578. https://doi.org/10.3390/microorganisms9030578.
Clarke CF, Bradley KK, Wright JH, Glowicz J. Case report: emergence of autochthonous cutaneous leishmaniasis in northeastern Texas and southeastern Oklahoma. Am J Trop Med Hyg. 2013;88(1):157–61. https://doi.org/10.4269/ajtmh.2012.11-0717.
Haddow AD, Curler G, Moulton JK. New records of Lutzomyia shannoni and Lutzomyia vexator (Diptera: Psychodidae) in eastern Tennessee. J Vector Ecol. 2008;33(2):393–6. https://doi.org/10.3376/1081-1710-33.2.393.
Mead DG, Cupp EW. Occurrence of Lutzomyia anthophora (Diptera: Psychodidae) in Arizona. J Med Entomol. 1995;32(5):747–8. https://doi.org/10.1093/jmedent/32.5.747.
Minter L, Kovacic B, Claborn DM, Lawyer P, Florin D, Brown GC. New state records for Lutzomyia shannoni and Lutzomyia vexator. J Med Entomol. 2009;46(4):965–8. https://doi.org/10.1603/033.046.0432.
Moo-Llanes D, Ibarra-Cerdeña CN, Rebollar-Téllez EA, Ibáñez-Bernal S, González C, Ramsey JM. Current and future niche of North and Central American sand flies (Diptera: Psychodidae) in climate change scenarios. PLoS Negl Trop Dis. 2013;7(9):e2421. https://doi.org/10.1371/journal.pntd.0002421.
Weng JL, Young SL, Gordon DM, Claborn D, Petersen C, Ramalho-Ortigao M. First report of phlebotomine sand flies (Diptera: Psychodidae) in Kansas and Missouri, and a PCR method to distinguish Lutzomyia shannoni from Lutzomyia vexator. J Med Entomol. 2012;49(6):1460–5. https://doi.org/10.1603/me12105.
Maroli M, Feliciangeli MD, Bichaud L, Charrel RN, Gradoni L. Phlebotomine sandflies and the spreading of leishmaniases and other diseases of public health concern. Med Vet Entomol. 2013;27(2):123–47. https://doi.org/10.1111/j.1365-2915.2012.01034.x.
Kipp EJ, de Almeida M, Marcet PL, Bradbury RS, Benedict TK, Lin W, et al. An atypical case of autochthonous cutaneous leishmaniasis associated with naturally infected Phlebotomine sand flies in Texas, United States. Am J Trop Med Hyg. 2020;103(4):1496–501. https://doi.org/10.4269/ajtmh.20-0107. Reported a case of autochthonous cutaneous leishmaniaisis, caused by L. mexicana, in Texas and identified Lutzomyia (Dampfomyia) anthophora as the potential vector
Endris RG, Young DG, Perkins PV. Experimental transmission of Leishmania mexicana by a North American sand fly, Lutzomyia anthophora (Diptera: Psychodidae). J Med Entomol. 1987;24(2):243–7. https://doi.org/10.1093/jmedent/24.2.243.
Lawyer PG, Young DG. Experimental transmission of Leishmania mexicana to hamsters by bites of phlebotomine sand flies (Diptera: Psychodidae) from the United States. J Med Entomol. 1987;24(4):458–62. https://doi.org/10.1093/jmedent/24.4.458.
Schaut RG, Robles-Murguia M, Juelsgaard R, Esch KJ, Bartholomay LC, Ramalho-Ortigao M, et al. Vectorborne transmission of Leishmania infantum from hounds. United States Emerg Infect Dis. 2015;21(12):2209–12. https://doi.org/10.3201/eid2112.141167.
Travi BL, Ferro C, Cadena H, Montoya-Lerma J, Adler GH. Canine visceral leishmaniasis: dog infectivity to sand flies from non-endemic areas. Res Vet Sci. 2002;72(1):83–6. https://doi.org/10.1053/rvsc.2001.0527.
Young DG, Perkins PV. Phlebotomine sand flies of North America (Diptera: Psychodidae). Mosquito News. 1984;44(2).
Minter L, Kovacic B, Claborn DM, Lawyer P, Florin D, Brown GC. New state records for Lutzomyia shannoni and Lutzomyia vexator. J Med Entomol. 2009;46(4):965–8. https://doi.org/10.1603/033.046.0432.
Weng J-L, Young SL, Gordon DM, Claborn D, Petersen C, Ramalho-Ortigao M. First report of phlebotomine sand flies (Diptera: Psychodidae) in Kansas and Missouri, and a PCR method to distinguish Lutzomyia shannoni from Lutzomyia vexator. J Med Entomol. 2012;49(6):1460–5. https://doi.org/10.1603/me12105.
McHugh CP, Ostrander BF, Raymond RW, Kerr SF. Population dynamics of sand flies (Diptera: Physchodidae) at two foci of leishmaniasis in Texas. J Med Entomol. 2001;38(2):268–77. https://doi.org/10.1603/0022-2585-38.2.268.
McHugh CP, Grogl M, Kreutzer RD. Isolation of Leishmania mexicana (Kinetoplastida: Trypanosomatidae) from Lutzomyia anthophora (Diptera: Psychodidae) collected in Texas. J Med Entomol. 1993;30(3):631–3. https://doi.org/10.1093/jmedent/30.3.631.
Pech-May A, Peraza-Herrera G, Moo-Llanes DA, Escobedo-Ortegón J, Berzunza-Cruz M, Becker-Fauser I, et al. Assessing the importance of four sandfly species (Diptera: Psychodidae) as vectors of Leishmania mexicana in Campeche. Mexico Med Vet Entomol. 2016;30(3):310–20. https://doi.org/10.1111/mve.12169.
Pech-May A, Escobedo-OrtegÓN FJ, Berzunza-Cruz M, Rebollar-TÉLlez EA. Incrimination of four sandfly species previously unrecognized as vectors of Leishmania parasites in Mexico. Med Vet Entomol. 2010;24(2):150–61. https://doi.org/10.1111/j.1365-2915.2010.00870.x.
Claborn D, Masuoka P, Morrow M, Keep L. Habitat analysis of North American sand flies near veterans returning from leishmania-endemic war zones. Int J Health Geogr. 2008;7(1):65. https://doi.org/10.1186/1476-072X-7-65.
Comer JA, Kavanaugh DM, Stallknecht DE, Ware GO, Corn JL, Nettles VF. Effect of forest type on the distribution of Lutzomyia shannoni (Diptera: Psyehodidae) and vesicular stomatitis virus on Ossabaw Island. Georgia J Med Entomol. 1993;30(3):555–60. https://doi.org/10.1093/jmedent/30.3.555.
Brinson FJ, Hagan DV, Comer JA, Strohlein DA. Seasonal abundance of Lutzomyia shannoni (Diptera: Psychodidae) on Ossabaw Island. Georgia J Med Entomol. 1992;29(2):178–82. https://doi.org/10.1093/jmedent/29.2.178.
Claborn DM, Rowton ED, Lawyer PG, Brown GC, Keep LW. Species diversity and relative abundance of phlebotomine sand flies (Diptera: Psychodidae) on three Army installations in the southern United States and susceptibility of a domestic sand fly to infection with Old World Leishmania major. Mil Med. 2009;174(11):1203–8. https://doi.org/10.7205/milmed-d-00-4309.
Lawyer PG, Young DG, Butler JF, Akin DE. Development of Leishmania mexicana in Lutzomyia diabolica and Lutzomyia shannoni (Diptera: Psychodidae)1. J Med Entomol. 1987;24(3):347–55. https://doi.org/10.1093/jmedent/24.3.347.
Serrano AK, Rojas JC, Cruz-López LC, Malo EA, Mikery OF, Castillo A. Presence of putative male-produced sex pheromone in Lutzomyia cruciata (Diptera: Psychodidae), vector of Leishmania mexicana. J Med Entomol. 2016;53(6):1261–7. https://doi.org/10.1093/jme/tjw118.
Rebollar-Téllez EA, Ramírez-Fraire A, Andrade-Narvaez FJ. A two years study on vectors of cutaneous Leishmaniasis Evidence for sylvatic transmission cycle in the state of Campeche Mexico. Mem Inst Oswaldo Cruz. 1996;91(5):555–60. https://doi.org/10.1590/s0074-02761996000500004.
Denlinger DS, Lozano-Fuentes S, Lawyer PG, Black WCt, Bernhardt SA. Assessing insecticide susceptibility of laboratory Lutzomyia longipalpis and Phlebotomus papatasi sand flies (Diptera: Psychodidae: Phlebotominae). J Med Entomol. 2015;52(5):1003–12. https://doi.org/10.1093/jme/tjv091.
Denlinger DS, Creswell JA, Anderson JL, Reese CK, Bernhardt SA. Diagnostic doses and times for Phlebotomus papatasi and Lutzomyia longipalpis sand flies (Diptera: Psychodidae: Phlebotominae) using the CDC bottle bioassay to assess insecticide resistance. Parasit Vectors. 2016;9:212. https://doi.org/10.1186/s13071-016-1496-3.
Miro G, Petersen C, Cardoso L, Bourdeau P, Baneth G, Solano-Gallego L, et al. Novel areas for prevention and control of canine leishmaniosis. Trends Parasitol. 2017;33(9):718–30. https://doi.org/10.1016/j.pt.2017.05.005.
Hlavacova J, Votypka J, Volf P. The effect of temperature on Leishmania (Kinetoplastida: Trypanosomatidae) development in sand flies. J Med Entomol. 2013;50(5):955–8.
Adamkiewicz T, Baltrus P, Li C, Carter-Wicker K, Gaglioti A. Quality of care indicators in patients with sickle cell disease (SCD): Influenza vaccination and routine eye examination are associated with outpatient utilization but not acute hospital care, whereas comorbidity indexes are strongly associated with both. Blood. 2018;132. https://doi.org/10.1182/blood-2018-99-120132.
Koch LK, Kochmann J, Klimpel S, Cunze S. Modeling the climatic suitability of leishmaniasis vector species in Europe. Sci Rep. 2017;7(1):13325. https://doi.org/10.1038/s41598-017-13822-1.
Moo-Llanes D, Ibarra-Cerdeña CN, Rebollar-Téllez EA, Ibáñez-Bernal S, González C, Ramsey JM. Current and future niche of North and Central American sand flies (Diptera: psychodidae) in climate change scenarios. PLoS Negl Trop Dis. 2013;7(9):e2421-e. https://doi.org/10.1371/journal.pntd.0002421.
Scorza BM, Mahachi KG, Cox AC, Toepp AJ, Leal-Lima A, Kumar Kushwaha A, et al. Leishmania infantum xenodiagnosis from vertically infected dogs reveals significant skin tropism. PLoS Negl Trop Dis. 2021;15(10):e0009366. https://doi.org/10.1371/journal.pntd.0009366. Vertically infected dogs presented significant skin tropism permiting transmission of Leishmania infantum to Lutzomyia longipalpis during a xenodiagnosis study. Identified the association between outward transmission potential from infected dogs to sand flies and early clinical status among L. infantum-infected dogs
Serafim TD, Coutinho-Abreu IV, Oliveira F, Meneses C, Kamhawi S, Valenzuela JG. Sequential blood meals promote Leishmania replication and reverse metacyclogenesis augmenting vector infectivity. Nat Microbiol. 2018;3(5):548–55. https://doi.org/10.1038/s41564-018-0125-7.
Solano-Gallego L, Miro G, Koutinas A, Cardoso L, Pennisi MG, Ferrer L, et al. LeishVet guidelines for the practical management of canine leishmaniosis. Parasit Vectors. 2011;4:86. https://doi.org/10.1186/1756-3305-4-86.
Drug resistance in Leishmania parasites: consequences, molecular mechanisms and possible treatments. New York, NY: Springer Berlin Heidelberg; 2018.
Quinnell RJ, Courtenay O. Transmission, reservoir hosts and control of zoonotic visceral leishmaniasis. Parasitol. 2009;136(14):1915–34. https://doi.org/10.1017/S0031182009991156.
Miro G, Lopez-Velez R. Clinical management of canine leishmaniosis versus human leishmaniasis due to Leishmania infantum: putting “One Health” principles into practice. Vet Parasitol. 2018;254:151–9. https://doi.org/10.1016/j.vetpar.2018.03.002.
Franssen SU, Sanders MJ, Berriman M, Petersen CA, Cotton JA. Geographic origin and vertical transmission of Leishmania infantum parasites in hunting hounds. United States Emerg Infect Dis. 2022;28(6):1211–23. https://doi.org/10.3201/eid2806.211746.
de Almeida ME, Spann DR, Bradbury RS. Leishmania infantum in US-Born Dog. Emerg Infect Dis. 2020;26(8):1882–4. https://doi.org/10.3201/eid2608.200149.
Gin TE, Lashnits E, Wilson JM, Breitschwerdt EB, Qurollo B. Demographics and travel history of imported and autochthonous cases of leishmaniosis in dogs in the United States and Canada, 2006 to 2019. J Vet Intern Med. 2021;35(2):954–64. https://doi.org/10.1111/jvim.16071.
Seal LM, Mullaney SB, Waugh SG. Leishmaniasis in the United States military veterinary patient population. J Am Vet Med Assoc. 2021;260(1):46–9. https://doi.org/10.2460/javma.21.05.0226.
Schantz PM, Steurer FJ, Duprey ZH, Kurpel KP, Barr SC, Jackson JE, et al. Autochthonous visceral leishmaniasis in dogs in North America. J Am Vet Med Assoc. 2005;226(8):1316–22. https://doi.org/10.2460/javma.2005.226.1316.
Anderson DC, Buckner RG, Glenn BL, MacVean DW. Endemic canine leishmaniasis. Vet Pathol. 1980;17(1):94–6. https://doi.org/10.1177/030098588001700110.
Castillo-Ureta H, Zazueta-Moreno JM, Rendon-Maldonado JG, Torres-Avendano JI, Lopez-Moreno HS, Olimon-Andalon V, et al. First report of autochthonous canine leishmaniasis caused by Leishmania (L.) mexicana in Sinaloa Mexico. Acta Trop. 2019;190:253–6. https://doi.org/10.1016/j.actatropica.2018.11.027.
Hopke K, Meyers A, Auckland L, Hamer S, Florin D, Diesel A, et al. Leishmania mexicana in a central Texas cat: clinical presentation, molecular identification, sandfly vector collection and novel management. JFMS Open Rep. 2021;7(1):2055116921999595. https://doi.org/10.1177/2055116921999595.
Petersen CA. Leishmaniasis, an emerging disease found in companion animals in the United States. Top Companion Anim Med. 2009;24(4):182–8. https://doi.org/10.1053/j.tcam.2009.06.006.
Trainor KE, Porter BF, Logan KS, Hoffman RJ, Snowden KF. Eight cases of feline cutaneous leishmaniasis in Texas. Vet Pathol. 2010;47(6):1076–81. https://doi.org/10.1177/0300985810382094.
Reuss SM, Dunbar MD, Calderwood Mays MB, Owen JL, Mallicote MF, Archer LL, et al. Autochthonous Leishmania siamensis in horse, Florida, USA. Emerg Infect Dis. 2012;18(9):1545–7. https://doi.org/10.3201/eid1809.120184.
Haque L, Villanueva M, Russo A, Yuan Y, Lee EJ, Topal J, et al. A rare case of visceral leishmaniasis in an immunocompetent traveler returning to the United States from Europe. PLoS Negl Trop Dis. 2018;12(10):e0006727. https://doi.org/10.1371/journal.pntd.0006727.
Ergen EN, King AH, Tuli M. Cutaneous leishmaniasis: an emerging infectious disease in travelers. Cutis. 2015;96(4):E22–6.
Chan CX, Simmons BJ, Call JE, Yan S, Glass JS, Chapman MS. Cutaneous leishmaniasis successfully treated with miltefosine. Cutis. 2020;106(4):206–9. https://doi.org/10.12788/cutis.0086.
Beiter KJ, Wentlent ZJ, Hamouda AR, Thomas BN. Nonconventional opponents: a review of malaria and leishmaniasis among United States Armed Forces. PeerJ. 2019;7:e6313. https://doi.org/10.7717/peerj.6313.
Mody RM, Lakhal-Naouar I, Sherwood JE, Koles NL, Shaw D, Bigley DP, et al. Asymptomatic visceral Leishmania infantum infection in US soldiers deployed to Iraq. Clin Infect Dis. 2019;68(12):2036–44. https://doi.org/10.1093/cid/ciy811.
McIlwee BE, Weis SE, Hosler GA. Incidence of endemic human cutaneous leishmaniasis in the United States. JAMA Dermatol. 2018;154(9):1032–9. https://doi.org/10.1001/jamadermatol.2018.2133. Reported 41 of 69 autochthonous leishmaniasis cases in Texas from 2007 to 2017. Most autochthonous leishmaniasis cases had L. mexicana identified as the infectious agent when speciation was performed
de Almeida M, Zheng Y, Nascimento FS, Bishop H, Cama VA, Batra D, et al. Cutaneous leishmaniasis caused by an unknown Leishmania strain, Arizona, USA. Emerg Infect Dis. 2021;27(6):1714–7. https://doi.org/10.3201/eid2706.204198.
Douvoyiannis M, Khromachou T, Byers N, Hargreaves J, Murray HW. Cutaneous leishmaniasis in North Dakota. Clin Infect Dis. 2014;59(5):e73–5. https://doi.org/10.1093/cid/ciu386.
Velez R, Gallego M. Commercially approved vaccines for canine leishmaniosis: a review of available data on their safety and efficacy. Trop Med Int Health. 2020;25(5):540–57. https://doi.org/10.1111/tmi.13382.
Toepp A, Larson M, Wilson G, Grinnage-Pulley T, Bennett C, Leal-Lima A, et al. Randomized, controlled, double-blinded field trial to assess Leishmania vaccine effectiveness as immunotherapy for canine leishmaniosis. Vaccine. 2018;36(43):6433–41. https://doi.org/10.1016/j.vaccine.2018.08.087. Found that anti-Leishmania vaccination in subclinical dogs significantly decreased risk of leishmaniosis clinical progression
Toepp A, Larson M, Grinnage-Pulley T, Bennett C, Anderson M, Parrish M, et al. Safety analysis of Leishmania vaccine used in a randomized canine vaccine/immunotherapy trial. Am J Trop Med Hyg. 2018;98(5):1332–8. https://doi.org/10.4269/ajtmh.17-0888.
Srivastava S, Shankar P, Mishra J, Singh S. Possibilities and challenges for developing a successful vaccine for leishmaniasis. Parasit Vectors. 2016;9(1):277. https://doi.org/10.1186/s13071-016-1553-y.
Lage DP, Ribeiro PAF, Dias DS, Mendonca DVC, Ramos FF, Carvalho LM, et al. A candidate vaccine for human visceral leishmaniasis based on a specific T cell epitope-containing chimeric protein protects mice against Leishmania infantum infection. NPJ Vaccines. 2020;5:75. https://doi.org/10.1038/s41541-020-00224-0.
Zhang WW, Karmakar S, Gannavaram S, Dey R, Lypaczewski P, Ismail N, et al. A second generation leishmanization vaccine with a markerless attenuated Leishmania major strain using CRISPR gene editing. Nat Commun. 2020;11(1):3461. https://doi.org/10.1038/s41467-020-17154-z.
Moafi M, Rezvan H, Sherkat R, Taleban R. Leishmania vaccines entered in clinical trials: a review of literature. Int J Prev Med. 2019;10:95. https://doi.org/10.4103/ijpvm.IJPVM_116_18.
Malvolti S, Malhame M, Mantel CF, Le Rutte EA, Kaye PM. Human leishmaniasis vaccines: use cases, target population and potential global demand. PLoS Negl Trop Dis. 2021;15(9):e0009742. https://doi.org/10.1371/journal.pntd.0009742.
Stockdale L, Newton R. A review of preventative methods against human leishmaniasis infection. PLoS Negl Trop Dis. 2013;7(6):e2278. https://doi.org/10.1371/journal.pntd.0002278.
Acknowledgements
Figure 1 map was created with mapchart.net.
Funding
National Institutes of Health (NIH) grant R01TW010500.
Author information
Authors and Affiliations
Contributions
All authors conceptualized the review article. EAB and KGM reviewed the published literature. The original draft was written by EAB and KGM. All authors reviewed and edited the draft. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Emerging Vector Borne Diseases in the U.S.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Beasley, E.A., Mahachi, K.G. & Petersen, C.A. Possibility of Leishmania Transmission via Lutzomyia spp. Sand Flies Within the USA and Implications for Human and Canine Autochthonous Infection. Curr Trop Med Rep 9, 160–168 (2022). https://doi.org/10.1007/s40475-022-00267-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40475-022-00267-4