
Abstract
Purpose of the Review
To provide a systematic review of experimental studies concerning cognitive functions in compulsive buying-shopping disorder (CBSD) and to evaluate the studies as supporting or not supporting the affective and cognitive interactions proposed by the Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors.
Recent Findings
The results of the present review concerning CBSD mirror findings regarding cue reactivity and disadvantageous decision making in other addictive behaviors, but they also demonstrate a relative lack of experimental studies addressing other cognitive domains such as attentional bias, inhibitory control, implicit associations, or Pavlovian-to-instrumental transfer. Experimental work on physiological and neural correlates of affective and cognitive mechanisms and their interaction in CBSD is still at the beginning.
Summary
While a reasonable number of experimental neuropsychological studies support the application of the I-PACE framework to CBSD, future research is required to systematically examine affective and cognitive interactions in CBSD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Key features of compulsive buying-shopping disorder (CBSD) include diminished control over the consumption of consumer goods and extreme preoccupation with buying/shopping, resulting in excessive purchasing of items without utilizing them for their intended purposes [1•]. While unregulated buying/shopping behavior leads to substantial negative consequences and impairments in important areas of functioning (e.g., debts, family discord, reduced quality of life) and/or clinically relevant distress, it is continued or even escalated [2]. CBSD is a cross-national public health problem [3•, 4] with an estimated prevalence of approximately 5% in the adult population [5]. However, whether CBSD can be recognized as a distinct mental disorder, and if so, how it should be best classified, has been debated for many years. Because of shared clinical features with impulse control disorders, the categorization of CBSD as such has been favored by some authors in the past [6]. Typical overlapping features are, e.g., repetitive failures to resist a strong impulse or urge to purchase consumer goods, longer-term harm either to the individual or to others due to inappropriate spending, and the increasing tension or affective arousal prior to a CBSD episode, which is relieved while buying/shopping [2]. These considerations may have contributed to the mention of CBSD as an example of “other specified impulse control disorder” in the coding tool of the 11th revision of the International Classification of Diseases (ICD-11) [7]. To be consistent with the ICD-11 terminology, we use the term “compulsive buying-shopping disorder” throughout the text to describe the phenomenon.
Very recently, CBSD has been linked to disorders due to addictive behaviors because of phenomenological and potential neurocognitive similarities [3•, 8,9,10]. By applying the ICD-11 criteria for gambling and gaming disorders to CBSD, phenomenological parallels exist with respect to impaired control over the behavior (e.g., onset, frequency, intensity, duration, termination, context), increasing priority given to the behavior to the extent that it takes precedence over other life interests and daily activities, continuation or escalation of the behavior despite negative consequences, and significant distress or impairment in important areas of functioning due to the behavior [7]. In terms of neurocognitive overlaps, an increasing number of experimental studies are being published indicating that CBSD fits in the ICD-11 category “disorders due to addictive behaviors” [3•, 8,9,10].
Regarding neurocognitive processes, it seems reasonable to apply the Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors to CBSD, particularly the inner circle of affective and cognitive interactions [11•]. In accordance with the I-PACE model, an urge to buy/shop something can be induced by internal (e.g., discomfort, boredom, self-insecurity) and/or external (e.g., advertisements, watching influencer posts, having extra money available) triggers. The repeated experience of positive feelings or relief from negative mood states while buying/shopping may result in an attentional bias related to these triggers, which in turn can reinforce the urge to buy/shop (in later stage of CBSD the craving for buying/shopping) and lead to an increase of buying/shopping activities. These interactions may be moderated by reduced general inhibitory control in the early stages and mediated by stimulus-specific inhibitory control deficits in the later stages of CBSD, finally resulting in more and more habitual maladaptive buying/shopping patterns [11•, 12•]. The affective and cognitive processes are likely to be associated with neuroadaptive changes in frontostriatal circuits over time [11•, 13•]. However, while a number of studies investigated affective and cognitive mechanisms in CBSD using behavioral tasks, neuroimaging studies on neural correlates are so far scarce [14••, 15].
The present systematic review of experimental studies addressing cognitive functions in CBSD represents an update of past narrative reviews [9, 10]. It was based on a systematic literature search and subsequent breakdown of results by cognitive domains. Since the number of studies on this topic was still relatively sparse, the time period for literature search was not restricted. At the same time, special attention was paid to progress made since 2018. Furthermore, we differentiated between studies using standardized behavioral tasks and those using adapted task versions with shopping-related cues. Another goal of the present systematic review was to evaluate the studies as supporting or not supporting the affective and cognitive interactions proposed by the I-PACE model [11•].
Method
The literature search aimed to identify all studies that assessed cognitive functions in relation to CBSD with experimental paradigms until July 2022. A comprehensive search string was created and adopted for Scopus and PubMed (see Table S1 in supplementary material). The complete search strings for both engines can be found in the supplementary Table S1. Studies written in English that conducted experimental research in cognitive domains related to CBSD were included. Studies not meeting these criteria were excluded. The initial search from both websites yielded a total of 377 papers (PubMed: 27 and Scopus: 350). After reading titles and abstracts, duplicates and publications not meeting the inclusion criteria were excluded, resulting in a final number of 26 studies included in the present review (see flow diagram, Figure S1 in supplementary material). After reviewing the full texts of included publications, the study results were divided according to cognitive domains they addressed. It is important to note that one paper can belong to more than one domain, if multiple cognitive domains were investigated within the study.
Results
Cognitive Domains
The experimental results were assigned to the following cognitive domains: working memory/learning abilities, attention/attentional bias, cognitive flexibility/planning, cue reactivity/craving, Pavlovian-to-instrumental transfer (PIT; i.e., the shift from behavior underlying Pavlovian conditioning to behavior rather driven by instrumental conditioning), decision making, inhibitory control, implicit associations, and others (i.e., if the paradigm was developed for the specific study). Table S2 (in the supplementary material) lists an overview of all included studies by cognitive domain. Most studies addressed multiple cognitive processes and applied multiple experimental paradigms accordingly. The most important results are summarized below. Of the 26 studies, a total of eight have been published since 2018. Detailed information about all included studies (i.e., sample description, design, operationalization of CBSD, experimental paradigm, outcome variables, main findings) is shown in Table 1.
Working Memory/Learning Abilities
The number of studies that focused particularly on memory processes in CBSD is comparably small. The advantage of the studies is that they all compared individuals with CBSD with healthy control participants. Two studies used established test batteries to measure general cognitive functioning with neutral cues (without shopping-related cues) [16, 18]. Individuals with CBSD exhibited greater deficits in spatial working memory than control participants in one study [16], but did not differ from control participants in another study on a spatial memory and a verbal learning task [18].
In the study of Kyrios et al. [17], a mood induction followed by a subsequent recognition memory task with shopping-related pictures was used. Surprisingly, a memory-facilitating effect of depressed mood was found in healthy control participants but not in individuals with CBSD [17]. In the second part of the same study, a recognition memory task in which products of high or low preference/rank were paired with functional or emotional words was conducted [17]. Persons with CBSD showed inferior performance when products were paired with functional words and superior performance when preferred products were paired with emotional words.
Attention/Attentional Bias
With regard to general, not shopping-related attention and concentration performance, no difference emerged between individuals with CBSD and control participants on the d2-test [22], Stroop Color Word Test [18, 22, 23], and Letter–Number Sequencing subtest from the Wechsler Adult Intelligence Scale [18] between patients with CBSD and healthy control participants. Jiang et al. [21] used an adopted version of the Stroop task (i.e., modified with online shopping words) to investigate potential attentional bias towards online shopping in a convenience sample. Individuals with high symptom severity of online CBSD showed attentional bias towards online shopping-related stimuli [21].
Studies using the dot-probe paradigm (DPP) with shopping-related compared to neutral pictures did not reveal conclusive results. Vogel et al. [20••] reported a lack of differences in DPP performance between patients with CBSD and healthy individuals. Trotzke et al. [19••] and Jiang et al. [21] administered the DPP with shopping-related pictures in convenience samples and did not find significant correlations between symptoms of CBSD and DPP performance. However, it is worth noting that in the Trotzke et al. [19••] study potential habituation effects were observed due to the administration of different tasks. The authors reported significant positive correlations between the attentional bias score and CBSD symptom severity after controlling for sequence effects (order of task administration) [19••].
Cognitive Flexibility/Planning
A small number of studies addressed cognitive flexibility in individuals with CBSD compared to healthy control participants by using standardized (all not adopted with shopping-related cues) experimental paradigms. Derbyshire et al. [16] administered the Intra-Extra Dimensional Set Shift Task to measure rule learning and behavior flexibility. Black et al. [18] and Trotzke et al. [22] used the Wisconsin Card Sorting Test to assess categorization and cognitive shifting abilities. None of the studies included in this review found any differences between individuals with CBSD and control participants [16, 18, 22].
Cue Reactivity
To measure cue-induced affective or craving responses, shopping-related cues were used in all studies, and different methods were chosen: subjective ratings of affective/craving responses (e.g., valence, arousal, urge to shop, purchase desire), peripheral physiological measure (skin conductance response, SCR), electroencephalogram recording (EEG), and functional brain imaging (fMRI).
In convenience samples, a positive correlation between symptoms of CBSD and subjective affective/craving responses towards shopping-related pictures was found [19••, 24••, 25, 26, 29]. Findings from clinical samples support the results. Patients with CBSD reported stronger subjective craving towards shopping-related cues than control participants [20••, 28] and an increase in subjective craving after the cue-reactivity paradigm [28].
Studies measuring cue reactivity with peripheral physiological measures revealed no correlation between SCR and symptom severity of CBSD in a convenience female sample [29]. In a clinical sample, SCR in response to shopping cues was stronger in patients with CBSD than in control participants [28]. However, there were no significant SCR differences within the CBSD group across shopping-related and neutral pictures, which may have indicated a generally elevated level of arousal in individuals with CBSD compared to healthy control individuals.
Lawrence et al. [27] assessed electroencephalogram cue reactivity in a convenience female sample. They used a combination of a recognition memory task with shopping-related pictures and a cue-reactivity paradigm (with a recall and a rating phase), where participants had to indicate their subjective urge to buy for each picture. Responses to preferred and non-preferred items were set in relation to EEG brain connectivity. The results indicated a left-sided lateralization in the EEG during the presentation of high-urge items in relation to CBSD symptom severity [27].
Trotzke et al. [14••] investigated neural correlates of cue reactivity in patients with CBSD compared to healthy control participants. They applied a cue-reactivity paradigm with individualized shopping-related and control pictures using fMRI and found stronger activities in the dorsal (but not in the ventral) striatum in patients with CBSD than in control participants during exposure to shopping-related compared to neutral pictures. However, increased activity in the ventral striatum was related to symptom severity in individuals with CBSD but not in the control group [14••]. These correlational results were consistent with the fMRI findings of Raab et al. [15] who found increased activity in the ventral striatum (nucleus accumbens) when patients with CBSD were presented with images of attractive consumer goods.
Pavlovian-to-Instrumental Transfer
The shift from Pavlovian-to-instrumental conditioning has been studied in many mental health conditions including substance use disorders and behavioral addictions (for an overview: Garbusow et al., 2022 [40]), but only once so in CBSD. Vogel et al. [30••] administered a PIT paradigm with appetitive pictures related to online gaming and online shopping applications in a convenience sample. During the Pavlovian phase, 62% of the sample learned the experimental contingencies and were able to discriminate between stimuli predicting the presentation of gaming-related pictures and stimuli predicting the presentation of shopping-related pictures. Symptoms of gaming disorder, but not online CBSD, predicted awareness [30••]. Specific PIT-effects for gaming and buying/shopping were observed in persons aware of experimental contingencies [30••]. Symptom severity of gaming disorder contributed to the gaming PIT-effect, while the magnitude of buying/shopping PIT-effect was not associated with online CBSD symptom severity [30••].
Decision Making
To explore decision-making abilities in CBSD, mainly standardized versions (without shopping-related cues) of the Iowa Gambling Task (IGT), Cambridge Gambling Task (CGT), Delay Discounting Task (DDT), and Game of Dice Task (GDT) have been utilized. Studies using the IGT, which assesses decision making under ambiguity, revealed mixed results. Billieux et al. [33] found no correlation between IGT net scores and symptoms of CBSD in a convenience sample and Black et al. [18] found no differences between individuals with CBSD and controls in IGT performance. In contrast, the studies of Trotzke et al. [22] and Voth et al. [23] indicated more disadvantageous decision making under ambiguity in patients with CBSD compared to control participants. Studies involving the DDT in a convenience sample [31] or the CGT in a clinical sample [16] also showed decision-making deficits related to CBSD. In terms of decision making under risky conditions, however, studies using the GDT did not find group differences between individuals with a high propensity towards CBSD compared to those with low propensity [32] or patients with CBSD compared to control participants [22].
The more recent IGT study by Trotzke et al. [24••] is an exception because it used a modified task with online shopping-related pictures placed either on the advantageous decks or on the disadvantageous decks (with control pictures on the opposing ones in a convenience sample). Participants with high online CBSD symptom severity compared to those with low severity showed performance deficits when the shopping cues were placed on the disadvantageous decks [24••].
The following three studies made use of adapted or specifically developed, closer to “real-world”, buying/shopping-specific decision-making tasks with images of consumer products. Vogt et al. [34] applied a mood induction and subsequent purchase task with pictures of consumer goods of relevance for female shoppers (clothes, shoes, jewelry, makeup). They assessed the following shopping-related proxies: likelihood to expose oneself to shopping websites, willingness to pay more money, product-specific urge to buy, and probability to buy. Participants with high symptom severity of CBSD differed from those with low severity in all variables, except the willingness to pay [34]. McQueen et al. [35] utilized images from eight product categories (body care items, accessories, sports equipment, kitchen items, clothes, jewelry, footwear, electronic leisure items) and found that buying-related cognitions may increase the likelihood to purchase consumer items on a shopping-related decision-making task, regardless of financial constraints. Raab et al. [15] investigated the neural correlates of purchasing decisions with fMRI by using an adapted version of the Saving Holdings or Purchase task [41] with images from six product categories (accessories, drinks, clothing, cosmetics, jewelry, and sweets). They found a higher activity in the ventral striatum (nucleus accumbens) during the presentation of purchasable products, lower insula activity during price presentation, and increased activation of the anterior cingulate cortex (ACC) during purchase decisions in individuals with CBSD compared to control participants [15].
Inhibitory Control
The experimental studies that have employed behavioral tasks to examine response inhibition in CBSD reported mixed findings. With regard to studies using traditional behavioral tasks (without shopping-related cues) in convenience samples, poor response inhibition as measured with the Stroop Matching Task or the Go/No-Go Task was related to more symptoms of CBSD in two studies [36••, 37], while no correlations between task performance and symptoms of CBSD were found regarding the Stop Signal Task in a third study [33]. By using shopping-related versus neutral cues, Hague and colleagues [38] found that individuals with high symptom severity of CBSD performed worse on the Go/No-Go task.
Using the Stop Signal Task in clinical samples, individuals with CBSD did not differ from the control group in one study [32] but showed poorer task performance than control participants in another study [16]. Applying a modified version of the Go/No-Go Task with shopping-related and neutral pictures, no differences in task performance between patients with CBSD and control participants were found in the study of Vogel et al. [20••]. However, using a modified affective shifting task in a convenience sample, Trotzke et al. [19••] indicated interactions between implicit cognitive processes (attentional bias, implicit associations), craving responses, and inhibitory control performance on symptom severity of CBSD [19••].
A unique study (including 5 sub-studies) on the effect of friendship reminders on inhibitory control was carried out by de Vries et al. [25] in a convenience sample. In sub-study 1, participants were assigned to a “friendship reminder condition” or a control condition and performed a modified Go/No-Go Task with tempting clothing pictures compared to basic furniture pictures. The results indicated that remembering a close friend (“friendship condition”) was associated with less inhibition failures in No-go trials (clothing items) in participants with high symptom severity of CBSD compared to those with low severity. In sub-study 3, task performance on the incongruent trial of the traditional Stroop Color Word Task (without shopping-related cues) was used to assess participants’ ability to identify a conflict and to implement self-control [25] (note that according to the authors, the task was not used to assess attention). Participants had to bring a close friend and were assigned to one of the following conditions: (1) being alone, (2) staying with a friend, or (3) being with a stranger. The mere physical presence of a friend reduced the response latencies on incongruent trials in individuals with high CBSD scores as compared to being alone or with a stranger. Sub-study 5 explored the neural correlates of friendship reminders on inhibitory control (same modified Go/No-Go Task as in sub-study 1). Participants with low levels of CBSD showed reduced activation in the ACC and dorsolateral prefrontal cortex after friendship reminders, while participants with high CBSD symptoms had an increased activity in these brain areas [25]. Taken together, the findings of de Vries et al. [25] suggest that for individuals with CBSD, friendship reminders or the presence of a friend increase self-control in shopping-related conflict situations.
Implicit Associations
At present, there is a relative lack of experimental studies addressing implicit associations in relation to CBSD. Black et al. [18] did not find differences in general associative abilities (verbal fluency) between patients with CBSD and control participants in the Controlled Word Association Test (without shopping-related cues). More recently, a modified version of the Implicit Associations Task (IAT) with shopping-related versus neutral pictures was applied to assess implicit associations towards buying/shopping. By using the same modified IAT in their studies, Vogel et al. [20••] did not observe differences in implicit associations between patients with CBSD and control participants, and Trotzke et al. [19••] did not detect a link between task performance and CBSD symptoms in a convenience sample. However, when the analyses were adjusted for habituation effects (i.e., controlling for order of task administration) in the Trotzke et al. [19••] study, more symptoms of CBSD were associated with more positive implicit associations towards shopping-related cues.
Application of the I-PACE Model to CBSD
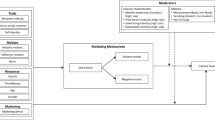
Figure 1 attempts to place the studies concerning cognitive functions in CBSD that support or do not support assumptions of the I-PACE model within the inner circle of affective and cognitive interactions [11•]. While research clearly supports the prominent role of cue reactivity and craving, relatively few studies have addressed the other components of the model, or studies have not produced conclusive results. Nevertheless, a reasonable number of experimental neuropsychological studies, particularly those using shopping-specific cues, support the application of the I-PACE framework to CBSD (see Table 1 for details).

Experimental studies on cognitive functions in CBSD supporting (+) or not supporting (−) the assumptions of the I-PACE model for addictive behaviors [11•]. Notes: A detailed description of all studies is shown in Table 1. The paper by de Vries and colleagues [25] has not been included in Figure 1 due to the highly specific ‘friendship’ condition. The paper by Nicolai et al. [39] and components of the investigation by Black et al. [18] have not been included in Figure 1 due to high specificity of tasks. The thickness of the blue boxes in the Figure represents the supporting and non-supporting studies. Figure 1 must be interpreted under consideration of the fact that the included studies differ regarding the methodology (i.e., sample size, convenience vs. clinical sample, neutral cues vs. shopping specific cues etc.). PIT = Pavlovian-to-instrumental transfer
Conclusions
The results of the present review concerning CBSD mirror findings regarding cue reactivity, craving, and disadvantageous decision making in other addictive behaviors [9, 10, 11•, 13•, 14••, 15, 16, 19••, 20••, 22, 23, 24••, 26,27,28,29, 31, 34, 35, 42,43,44], but they also demonstrate a relative lack of experimental studies addressing other cognitive domains (e.g., attentional bias, inhibitory control, implicit associations, Pavlovian-to-instrumental transfer). As shown in Fig. 1, there is, however, preliminary support for affective and cognitive mechanisms and their interactions in CBSD as assumed by the I-PACE model for addictive behaviors [11•]. This applies in particular to cue-induced craving [14••, 15, 19••, 20••, 24••, 26,27,28,29] and disadvantageous decision making under ambiguity [22, 23, 24••] which may be the basis for shopping-specific habitual decisions and behaviors [15, 24••, 30••, 34, 35]. Other studies stressed the role of buying-related beliefs in CBSD [35]. Some studies showed moderating effects of craving, implicit associations, or inhibitory control on symptoms of CBSD [19••] or on decision making [24••], providing further insights into potential pathomechanisms and support for the application of the I-PACE model to CBSD. Experimental work on the neural correlates of cue reactivity and executive functioning in CBSD is still at the beginning. The few neuroimaging studies highlight the importance of striatal activity in cue exposure and of prefrontal structures, ACC, and insula in inhibitory control/goal conflict identification [14••, 15, 25]. These outcomes together with the other results mentioned above correspond with findings about cue reactivity, craving, executive functions, and neural pathways involved in addictive disorders [8, 11•, 44]. Therefore, the present findings do not only support the application of the theoretical I-PACE framework to CBSD, but they also argue for classifying CBSD as a disorder due to addictive behaviors.
The interest in CBSD in the last years has accelerated, and there has been progress in neurocognitive research on CBSD compared to the last reviews [9, 10]. An advantage of most studies published since 2018 is that, with few exceptions, they have used behavioral tasks with disorder-specific shopping cues. Nevertheless, the number of experimental studies conducted within the past 5 years is low as compared to experimental and neuroimaging studies in other behavioral addictions, e.g., gaming disorder [13•, 45]. Studies of CBSD primarily addressed cue reactivity and possible deficits in inhibitory control processes in CBSD as key characteristics of addictive behaviors. In contrast, attentional processes, implicit associations, and the shift from Pavlovian-to-instrumental conditioning have been studied less intensively.
Clinical Implications
The importance of cue-induced craving responses in CBSD has several clinical implications. Buying and shopping are necessary everyday activities. The complete avoidance of stores and online shopping platforms or abstinence from the consumption of consumer goods is not realistic. The ubiquity of advertising, merchandising, and other external buying/shopping stimuli can cause strong urges to buy/shop and craving responses. Therefore, psychotherapy of CBSD should deal with external (e.g., advertisements, watching influencer posts, having extra money available) and internal (e.g., discomfort, boredom, self-insecurity) triggers and strengthen self-control abilities to normalize buying/shopping behaviors. Traditional cognitive-behavioral strategies have been shown to be helpful in treating patients with CBSD (for review see: [46]). Patients could further benefit from third-wave behavioral treatments such as mindfulness-based therapy [47] or from adjunct neurocognitive approaches such as inhibitory control and cognitive bias modification trainings [48].
Limitations
The summarized studies and hence this systematic review have several limitations. First, small sample sizes in some studies limit the statistical power of their findings and might be a possible reason for failure to report differences between individuals with CBSD and healthy control participants [49, 50]. Second, convenience samples of some studies partly relied on college or university student samples imposing further constraints for external validity [51]. However, using predefined convenience samples represents an adequate attempt to explore research questions and serve planning studies in clinical samples. Third, the number of studies in some of the cognitive areas (e.g., PIT, implicit associations) is limited hindering conclusions that can be drawn from these sections. Lastly, Fig. 1 must be interpreted with caution, given the fact that the included studies differ regarding the methodology (i.e., sample size, convenience vs. clinical sample, neutral cues vs. shopping-specific cues).
Future Directions
The examination of psychophysiological and neural correlates of affective and cognitive mechanisms of CBSD would contribute to a better understanding of the phenomenon. In addition, more studies are required that differentiate between general cognitive deficits and specific affective and cognitive alterations in response to buying-shopping-related stimuli. As suggested in the I-PACE model for addictive behaviors [11•], specific stimulus-related inhibitory control deficits are considered especially relevant in later stages of the addiction process. In line with this, future studies should aim at investigating clinical samples and/or samples at a large scale showing risky and pathological behaviors. Longitudinal studies would help to explore trajectories of underlying cognitive mechanisms and draw causal interpretations regarding the direction of interactions between cognitive processes and symptoms of CBSD. Moreover, potential tertiary or external aspects that might influence CBSD such as stress vulnerability, genetic predispositions, or context variables should be considered, as well as comorbidity with other mental disorders.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Müller A, Laskowski NM, Trotzke P, Ali K, Fassnacht DB, de Zwaan M, et al. Proposed diagnostic criteria for compulsive buying-shopping disorder: a Delphi expert consensus study. J Behav Addict. 2021;10:208–22. https://doi.org/10.1556/2006.2021.00013. This study represents a synthesis of expert opinions with a Delphi approach regarding diagnostic criteria for CBSD and bundles them into consensual proposed diagnostic criteria for CBSD.
Black DW. Compulsive shopping: a review and update. Curr Opin Psychol. 2022;46:101321.
Müller A, Brand M, Claes L, Demetrovics Z, de Zwaan M, Fernández-Aranda F, et al. Buying-shopping disorder-is there enough evidence to support its inclusion in ICD-11? CNS Spectr. 2019;24:374–79. https://doi.org/10.1017/S1092852918001323. This perspective paper provides a comprehensive outline of CBSD literature and reviews eligibility to be considered a separate mental health condition contributing to a recent debate regarding the classification of CBSD, e.g., in ICD-11.
Parra-Díaz P, Chico-García JL, Beltrán-Corbellini Á, Rodríguez-Jorge F, Fernández-Escandón CL, Alonso-Cánovas A, Martínez-Castrillo JC. Does the country make a difference in impulse control disorders? A systematic review. Mov Disord Clin Pract. 2021;8:25–32. https://doi.org/10.1002/mdc3.13128.
Maraz A, Griffiths MD, Demetrovics Z. The prevalence of compulsive buying: a meta-analysis. Addiction. 2016;111:408–19. https://doi.org/10.1111/add.13223.
Grant JE, Potenza MN. Impulse control disorders: clinical characteristics and pharmacological management. Ann Clin Psychiatry. 2004;16:27–34. https://doi.org/10.1080/10401230490281366.
WHO. International Classification of Diseases (11th revision): 2022. https://icd.who.int/ct11/icd11_mms/en/release. Accessed 5 Feb 2023
Brand M, Rumpf H-J, Demetrovics Z, Müller A, Stark R, King DL, et al. Which conditions should be considered as disorders in the International Classification of Diseases (ICD-11) designation of “other specified disorders due to addictive behaviors”? J Behav Addict. 2020;11:150–9. https://doi.org/10.1556/2006.2020.00035.
Kyrios M, Trotzke P, Lawrence L, Fassnacht DB, Ali K, Laskowski NM, Müller A. Behavioral neuroscience of buying-shopping disorder: a review. Curr Behav Neurosci Rep. 2018;5:263–70. https://doi.org/10.1007/s40473-018-0165-6.
Trotzke P, Brand M, Starcke K. Cue-reactivity, craving, and decision making in buying disorder: a review of the current knowledge and future directions. Curr Addict Rep. 2017;4:246–53. https://doi.org/10.1007/s40429-017-0155-x.
Brand M, Wegmann E, Stark R, Müller A, Wölfling K, Robbins TW, Potenza MN. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci Biobehav Rev. 2019;104:1–10. https://doi.org/10.1016/j.neubiorev.2019.06.032. This work represents the update of the I-PACE model, a central model for behavioral addictions, now differentiating between an earlier stage and a later stage of behavioral addictions.
Müller A, Joshi M, Thomas TA. Excessive shopping on the internet: recent trends in compulsive buying-shopping disorder. Curr Opin Behav Sci. 2022;44:101116. https://doi.org/10.1016/j.cobeha.2022.101116. The short review is about the latest research in CBSD and recent developments, e.g., COVID-19. It focuses, wherever possible, on online CBSD showing progress but yet a vast lack of research in this emerging problematic behavior.
Brand M. Can internet use become addictive? Science. 2022;376:798–9. https://doi.org/10.1126/science.abn4189. The perspective paper shows similarities between substance use disorders and internet-use disorders and briefly reviews neural pathways involved in internet-use disorders. It represents a concise overview shedding light on further research directions in the field.
Trotzke P, Starcke K, Pedersen A, Brand M. Dorsal and ventral striatum activity in individuals with buying-shopping disorder during cue-exposure: a functional magnetic resonance imaging study. Addict Biol. 2021;26:e13073. https://doi.org/10.1111/adb.13073. A fMRI study with shopping-related cues is reported that highlights the pivotal role of the striatal area in CBSD and provides support for a ventral-dorsal gradient in the course of the CBSD development. It is one of the first neuroimaging studies in CBSD.
Raab G, Elger CE, Neuner M, Weber B. A Neurological study of compulsive buying behaviour. J Consum Policy. 2011;34:401–13. https://doi.org/10.1007/s10603-011-9168-3.
Derbyshire KL, Chamberlain SR, Odlaug BL, Schreiber L, Grant JE. Neurocognitive functioning in compulsive buying disorder. Ann Clin Psychiatry. 2014;26:57–63. https://doi.org/10.5194/gi-2016-11-RC2.
Kyrios M, McQueen P, Moulding R. Experimental analysis of the relationship between depressed mood and compulsive buying. J Behav Ther Exp Psychiatry. 2013;44:194–200. https://doi.org/10.1016/j.jbtep.2012.10.004.
Black DW, Shaw M, McCormick B, Bayless JD, Allen J. Neuropsychological performance, impulsivity, ADHD symptoms, and novelty seeking in compulsive buying disorder. Psychiatry Res. 2012;200:581–7. https://doi.org/10.1016/j.psychres.2012.06.003.
Trotzke P, Müller A, Brand M, Starcke K, Steins-Loeber S. Buying despite negative consequences: interaction of craving, implicit cognitive processes, and inhibitory control in the context of buying-shopping disorder. Addict Behav. 2020;110:106523. https://doi.org/10.1016/j.addbeh.2020.106523. This study shows that an increase in craving can be observed during the cue-reactivity paradigm. Additionally, it also proves that craving, implicit cognitions, and attentional bias are all related to CBSD severity.
Vogel B, Trotzke P, Steins-Loeber S, Schäfer G, Stenger J, de Zwaan M, et al. An experimental examination of cognitive processes and response inhibition in patients seeking treatment for buying-shopping disorder. PLoS ONE. 2019;14:e0212415. https://doi.org/10.1371/journal.pone.0212415. This paper proves the vital role of craving in CBSD, where individuals show stronger cravings reactions for buying shopping-related stimuli.
Jiang Z, Zhao X, Li C. Self-control predicts attentional bias assessed by online shopping-related Stroop in high online shopping addiction tendency college students. Compr Psychiatry. 2017;75:14–21. https://doi.org/10.1016/j.comppsych.2017.02.007.
Trotzke P, Starcke K, Pedersen A, Müller A, Brand M. Impaired decision making under ambiguity but not under risk in individuals with pathological buying-behavioral and psychophysiological evidence. Psychiatry Res. 2015;229:551–8. https://doi.org/10.1016/j.psychres.2015.05.043.
Voth EM, Claes L, Georgiadou E, Selle J, Trotzke P, Brand M, et al. Reactive and regulative temperament in patients with compulsive buying and non-clinical controls measured by self-report and performance-based tasks. Compr Psychiatry. 2014;55:1505–12. https://doi.org/10.1016/j.comppsych.2014.05.011.
Trotzke P, Starcke K, Müller A, Brand M. Cue-induced craving and symptoms of online-buying-shopping disorder interfere with performance on the Iowa Gambling Task modified with online-shopping cues. Addict Behav. 2019;96:82–8. https://doi.org/10.1016/j.addbeh.2019.04.008. The study examined cue reactivity and decision making in online CBSD. It is among the first studies reporting dysfunctional decision making in a decision-making task with online shopping pictures in persons with symptoms of online CBSD.
de Vries EL, Fennis BM, Bijmolt TH, ter Horst GJ, Marsman J-BC. Friends with benefits: Behavioral and fMRI studies on the effect of friendship reminders on self-control for compulsive and non-compulsive buyers. Int J Res Mark. 2018;35:336–58. https://doi.org/10.1016/j.ijresmar.2017.12.004.
Trotzke P, Starcke K, Müller A, Brand M. Pathological buying online as a specific form of internet addiction: a model-based experimental investigation. PLoS ONE. 2015;10:e0140296. https://doi.org/10.1371/journal.pone.0140296.
Lawrence LM, Ciorciari J, Kyrios M. Cognitive processes associated with compulsive buying behaviours and related EEG coherence. Psychiatry Res. 2014;221:97–103. https://doi.org/10.1016/j.pscychresns.2013.10.005.
Trotzke P, Starcke K, Pedersen A, Brand M. Cue-induced craving in pathological buying: empirical evidence and clinical implications. Psychosom Med. 2014;76:694–700. https://doi.org/10.1097/PSY.0000000000000126.
Starcke K, Schlereth B, Domass D, Schöler T, Brand M. Cue reactivity towards shopping cues in female participants. J Behav Addict. 2013;2:17–22. https://doi.org/10.1556/JBA.1.2012.012.
Vogel V, Kollei I, Duka T, Snagowski J, Brand M, Müller A, Loeber S. Pavlovian-to-instrumental transfer: a new paradigm to assess pathological mechanisms with regard to the use of Internet applications. Behav Brain Res. 2018;347:8–16. https://doi.org/10.1016/j.bbr.2018.03.009. The study is the first to use a PIT paradigm in the context of persons with online CBSD symptoms. It investigated if the PIT effect was associated to online CBSD symptoms in a convenience sample but found no association.
Nicolai J, Moshagen M. Dissociating pathological buying from obsessive-compulsive symptoms using delay discounting. Z Psychol. 2017;225:244–51. https://doi.org/10.1027/2151-2604/a000308.
Vogt S, Hunger A, Pietrowsky R, Gerlach AL. Impulsivity in consumers with high compulsive buying propensity. J Obsessive Compuls Relat Disord. 2015;7:54–64. https://doi.org/10.1016/j.jocrd.2015.10.002.
Billieux J, Gay P, Rochat L, van der Linden M. The role of urgency and its underlying psychological mechanisms in problematic behaviours. Behav Res Ther. 2010;48:1085–96. https://doi.org/10.1016/j.brat.2010.07.008.
Vogt S, Hunger A, Türpe T, Pietrowsky R, Gerlach AL. Effects of mood induction on consumers with vs. without compulsive buying propensity: an experimental study. Psychiatry Res. 2014;220:342–47. https://doi.org/10.1016/j.psychres.2014.06.014.
McQueen P, Moulding R, Kyrios M. Experimental evidence for the influence of cognitions on compulsive buying. J Behav Ther Exp Psychiatry. 2014;45:496–501. https://doi.org/10.1016/j.jbtep.2014.07.003.
Lindheimer N, Nicolai J, Moshagen M. General rather than specific: cognitive deficits in suppressing task irrelevant stimuli are associated with buying-shopping disorder. PLoS ONE. 2020;15:e0237093. https://doi.org/10.1371/journal.pone.0237093. This paper focuses mainly on the Stroop Task and shows how CBSD is associated with poorer performance on this task, proving that the disorder results in deficits with respect to stimulus interference, reflecting general cognitive shortcomings.
Nicolai J, Darancó S, Moshagen M. Effects of mood state on impulsivity in pathological buying. Psychiatry Res. 2016;244:351–6. https://doi.org/10.1016/j.psychres.2016.08.009.
Hague B, Kellett S, Sheeran P. Testing the generalizability of impulse control problems in compulsive buying. J Soc Clin Psychol. 2016;35:269–88. https://doi.org/10.1521/jscp.2016.35.4.269.
Nicolai J, Moshagen M. Pathological buying symptoms are associated with distortions in judging elapsed time. J Behav Addict. 2018;7:752–9. https://doi.org/10.1556/2006.7.2018.80.
Garbusow M, Ebrahimi C, Riemerschmid C, Daldrup L, Rothkirch M, Chen K, et al. Pavlovian-to-instrumental transfer across mental disorders: a review. Neuropsychobiology. 2022;81(5):418–434. https://doi.org/10.1159/000525579
Knutson B, Rick S, Wimmer GE, Prelec D, Loewenstein G. Neural predictors of purchases. Neuron. 2007;53:147–56. https://doi.org/10.1016/j.neuron.2006.11.010.
Starcke K, Antons S, Trotzke P, Brand M. Cue-reactivity in behavioral addictions: a meta-analysis and methodological considerations. J Behav Addict. 2018;7:227–38. https://doi.org/10.1556/2006.7.2018.39.
Antons S, Brand M, Potenza MN. Neurobiology of cue-reactivity, craving, and inhibitory control in non-substance addictive behaviors. J Neurol Sci. 2020;415:116952.
Berridge KC, Robinson TE. Liking, wanting, and the incentive-sensitization theory of addiction. Am Psychol. 2016;71:670–9. https://doi.org/10.1037/amp0000059.
Weinstein A, Lejoyeux M. Neurobiological mechanisms underlying internet gaming disorder. Dialogues Clin Neurosci. 2020;22:113–26. https://doi.org/10.31887/DCNS.2020.22.2/aweinstein.
Hague B, Hall J, Kellett S. Treatments for compulsive buying: a systematic review of the quality, effectiveness and progression of the outcome evidence. J Behav Addict. 2016;5:379–94. https://doi.org/10.1556/2006.5.2016.064.
Schwebel FJ, Korecki JR, Witkiewitz K. Addictive behavior change and mindfulness-based interventions: current research and future directions. Curr Addict Rep. 2020;7:117–24. https://doi.org/10.1007/s40429-020-00302-2.
Reichl D, Enewoldsen N, Müller A, Steins-Loeber S. Pilot testing of an adaptive, individualized inhibitory control training for binge drinking: first evidence on feasibility, acceptance, and efficacy. Psychol Res. 2022. https://doi.org/10.1007/s00426-022-01725-4.
Button KS, Ioannidis JPA, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, Munafò MR. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14:365–76. https://doi.org/10.1038/nrn3475.
Ioannidis JPA. Why most published research findings are false. PLoS Med. 2005;2:e124. https://doi.org/10.1371/journal.pmed.0020124.
Stroebe W, Gadenne V, Nijstad BA. Do our psychological laws apply only to college students?: External validity revisited. Basic Appl Soc Psych. 2018;40:384–95. https://doi.org/10.1080/01973533.2018.1513362.
Funding
Open Access funding enabled and organized by Projekt DEAL. The work of TAT, MJ, SSL, and AM on this article was carried out in the context of the Research Unit “Affective and cognitive mechanisms of specific Internet-use disorders”, FOR2974, funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) — 411232260.
Some authors have received further funding/grants from public sources (e.g., DAAD: AM; Federal Ministry of Education and Research: AM, SSL; Innovationsfonds of the Gemeinsame Bundesausschuss: SSL).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Addictions.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thomas, T.A., Joshi, M., Trotzke, P. et al. Cognitive Functions in Compulsive Buying-Shopping Disorder: a Systematic Review. Curr Behav Neurosci Rep 10, 1–19 (2023). https://doi.org/10.1007/s40473-023-00255-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40473-023-00255-6