
Abstract
Background
Pharmacotherapy remains the mainstay of treatment for acute bipolar mania, but there are many choices, including mood stabilizers (MSs) and antipsychotics (APs).
Objective
To provide an up-to-date and comprehensive review of the efficacy, acceptability and adverse effects of MSs and APs as combination or augmentation therapy versus monotherapy with either drug class for the treatment of acute mania.
Data Sources
The Cochrane Central Register of Controlled Trials, MEDLINE, PsycINFO, Scopus, and clinical trial databases were searched for articles published between the inception of the databases and July 1, 2014. The following keywords were used: [bipolar disorder, mania, manic, mixed bipolar, schizoaffective] combined with the names of MSs and APs. The reference lists of all the identified randomized controlled trials (RCTs), articles that cited the identified trials, and recent systematic reviews were also checked.
Study Selection
Double-blind RCTs comparing MS and AP as combination or augmentation therapy with either monotherapy during the acute phase treatment of mania were included in the present study. The electronic search yielded 6,445 potential articles in September 2013 and 264 new references in an updated search performed in July 2014. Finally, 19 RCTs were considered eligible for our meta-analyses: MS plus AP combination or augmentation therapy was compared with MS monotherapy in 14 trials (n = 3,651) and with AP monotherapy in 6 trials (n = 606) [one study compared combination therapy versus both MS monotherapy and AP monotherapy].
Data Extraction
The primary outcomes were the mean change scores on validated rating scales for mania and all-cause discontinuation at 3 weeks. The secondary outcomes included response, remission, the mean change scores for depression, dropouts due to adverse events and to inefficacy, and adverse events at 3 weeks and mean change scores on validated rating scales at 1 week. Using random-effects models, standardized mean difference (SMD), risk ratio (RR) and numbers needed to treat with their 95 % confidence intervals (CIs) were calculated.
Results
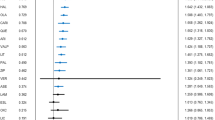
Most patients included in trials comparing combination/augmentation therapy versus MS monotherapy had prior treatment with an MS, while more than 70 % of participants in trials comparing combination/augmentation therapy versus AP monotherapy had not been on medications or were washed out from their previous medication before randomization. MS plus AP combination/augmentation therapy was more effective than MS monotherapy in terms of change in scores on mania rating scales at 3 weeks (SMD −0.26; 95 % CI −0.36 to −0.15) and at 1 week (SMD −0.17, −0.29 to −0.04). MS plus AP combination/augmentation therapy was more effective than AP monotherapy at 3 weeks (SMD −0.31, −0.50 to −0.12), but not at 1 week (SMD −0.22, −0.84 to 0.40). No significant differences were seen between the combination/augmentation therapy and either monotherapy group in study withdrawal for any reason (MS + AP vs. MS monotherapy: RR 0.99, 0.88–1.12; MS + AP vs. AP monotherapy: RR 0.70, 0.47–1.04) or adverse events (MS + AP vs. MS monotherapy: RR 1.39, 0.97–1.99; MS + AP vs. AP monotherapy: RR 0.62, 0.27–1.40). The combination/augmentation therapy was associated with more side effects, especially with somnolence, while it did not increase treatment-emergent depression.
Conclusions
Combining MS and AP is more efficacious and more burdensome than, but overall as acceptable as, the continuation of MS or AP monotherapy, when either monotherapy has not been successful. There is currently no robust evidence to judge whether MS and AP combination therapy is more efficacious than MS monotherapy as the initial therapy for acutely manic patients without prior medication.





Similar content being viewed by others


References
Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96.
Merikangas KR, Akiskal HS, Angst J, et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch Gen Psychiatry. 2007;64(5):543–52.
Simon GE, Unutzer J. Health care utilization and costs among patients treated for bipolar disorder in an insured population. Psychiatr Serv. 1999;50(10):1303–8.
Grunze H, Vieta E, Goodwin GM, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders: update 2009 on the treatment of acute mania. World J Biol Psychiatry. 2009;10(2):85–116.
NICE. Bipolar disorder. July 2006. http://publications.nice.org.uk/bipolar-disorder-cg38.
Goodwin GM, Psycho CGBA. Evidence-based guidelines for treating bipolar disorder: revised second edition-recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346–88.
Smith LA, Cornelius V, Warnock A, et al. Acute bipolar mania: a systematic review and meta-analysis of co-therapy vs. monotherapy. Acta Psychiatr Scand. 2007;115(1):12–20.
Scherk H, Pajonk FG, Leucht S. Second-generation antipsychotic agents in the treatment of acute mania: a systematic review and meta-analysis of randomized controlled trials. Arch Gen Psychiatry. 2007;64(4):442–55.
Vieta E. The treatment of mixed states and the risk of switching to depression. Eur Psychiatry. 2005;20(2):96–100.
The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Updated March, 2011; 5.1.0 2011 http://handbook.cochrane.org/.
Malhi GS, Adams D, Lampe L, et al. Clinical practice recommendations for bipolar disorder. Acta Psychiatr Scand. 2009;119(Suppl. 439):27–46.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Furukawa TA, Cipriani A, Barbui C, et al. Imputing response rates from means and standard deviations in meta-analyses. Int Clin Psychopharmacol. 2005;20(1):49–52.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Divalproex Extended Release and placebo, lithium, or quetiapine for mania. ClinicalTrials.gov. http://clinicaltrials.gov/show/NCT00183443. Accessed 20 Sept 2013.
Quetiapine Sr as Adjunctive Treatment In Mixed States of Bipolar Disorder. ClinicalTrials.gov. http://clinicaltrials.gov/show/NCT01195363. Accessed 20 Sept 2013.
Berwaerts J, Lane R, Nuamah IF, et al. Paliperidone extended-release as adjunctive therapy to lithium or valproate in the treatment of acute mania: a randomized, placebo-controlled study. J Affect Disord. 2011;129(1–3):252–60.
Study to Evaluate the Efficacy and Safety of Aripiprazole Administered With Lithium or Valproate Over 12 Weeks in the Treatment of Mania in Bipolar I Disorder. ClinicalTrials.gov. http://clinicaltrials.gov/show/NCT00665366. Accessed 20 Sep 2013.
Garfinkel PE, Stancer HC, Persad E. A comparison of haloperidol, lithium carbonate and their combination in the treatment of mania. J Affect Disord. 1980;2(4):279–88.
Houston JP, Tohen M, Degenhardt EK, et al. Olanzapine-divalproex combination versus divalproex monotherapy in the treatment of bipolar mixed episodes: a double-blind, placebo-controlled study. J Clin Psychiatry. 2009;70(11):1540–7.
Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry. 2002;159(7):1146–54.
Sachs G, Chengappa KN, Suppes T, et al. Quetiapine with lithium or divalproex for the treatment of bipolar mania: a randomized, double-blind, placebo-controlled study. Bipolar Disord. 2004;6(3):213–23.
Sachs GS, Vanderburg DG, Edman S, et al. Adjunctive oral ziprasidone in patients with acute mania treated with lithium or divalproex, part 1: results of a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2012;73(11):1412–9.
Szegedi A, Calabrese JR, Stet L, et al. Asenapine as adjunctive treatment for acute mania associated with bipolar disorder results of a 12-week core study and 40-week extension. J Clin Psychopharmacol. 2012;32(1):46–55.
Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry. 2002;59(1):62–9.
Tohen M, Bowden CL, Smulevich AB, et al. Olanzapine plus carbamazepine v. carbamazepine alone in treating manic episodes. Br J Psychiatry. 2008;192(2):135–43.
Vieta E, T’joen C, McQuade RD, et al. Efficacy of adjunctive aripiprazole to either valproate or lithium in bipolar mania patients partially nonresponsive to valproate/lithium monotherapy: A placebo-controlled study. Am J Psychiatry. 2008;165(10):1316–25.
Weisler RH, Dunn J, English P. Ziprasidone in adjunctive treatment of acute mania: a randomised, double-blind, placebo-controlled trial. Eur Neuropsychopharmacol. 2003;13(SUPPL. 4):S344–5.
Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blind, randomised controlled trial. Br J Psychiatry. 2003;182:369.
Yatham LN, Vieta E, Young AH, et al. A double blind, randomized, placebo-controlled trial of quetiapine as an add-on therapy to lithium or divalproex for the treatment of bipolar mania. Int Clin Psychopharmacol. 2007;22(4):212–20.
Biederman J, Lerner Y, Belmaker RH. Combination of lithium carbonate and haloperidol in schizo-affective disorder: a controlled study. Arch Gen Psychiatry. 1979;36(3):327–33.
Bourin M. An international, multicenter, double-blind, randomized, placebo-controlled, phase IV study of the safety and efficacy of lithium versus placebo as an add on to SEROQUEL XR (Quetiapine Fumarate) in adult patients with acute mania. AstraZeneca Clinical Trials. http://www.astrazenecaclinicaltrials.com/_mshost800325/content/clinical-trials/resources/pdf/D144AC00003. Accessed 20 Sept 2013.
Chou JC, Czobor P, Charles O, et al. Acute mania: haloperidol dose and augmentation with lithium or lorazepam. J Clin Psychopharmacol. 1999;19(6):500–5.
Möller HJ, Kissling W, Riehl T, et al. Doubleblind evaluation of the antimanic properties of carbamazepine as a comedication to haloperidol. Prog Neuropsychopharmacol Biol Psychiatry. 1989;13(1–2):127–36.
Müller-Oerlinghausen B, Retzow A, Henn FA, et al. Valproate as an adjunct to neuroleptic medication for the treatment of acute episodes of mania: a prospective, randomized, double-blind, placebo-controlled, multicenter study. European Valproate Mania Study Group. J Clin Psychopharmacol. 2000;20(2):195–203.
Keck PE, Orsulak PJ, Cutler AJ, et al. Aripiprazole monotherapy in the treatment of acute bipolar I mania: A randomized, double-blind, placebo- and lithium-controlled study. J Affect Disord. 2009;112(1–3):36–49.
Niufan G, Tohen M, Qiuqing A, et al. Olanzapine versus lithium in the acute treatment of bipolar mania: A double-blind, randomized, controlled trial. J Affect Disord. 2008;105(1–3):101–8.
Tohen M, Baker RW, Altshuler LL, et al. Olanzapine versus divalproex in the treatment of acute mania. Am J Psychiatry. 2002;159(6):1011–7.
Tohen M, Vieta E, Goodwin GM, et al. Olanzapine versus divalproex versus placebo in the treatment of mild to moderate mania: a randomized, 12-week, double-blind study. J Clin Psychiatry. 2008;69(11):1776–89.
Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. Lancet. 2011;378(9799):1306–15.
Acknowledgments
YO, AT and NT have received honoraria for speaking at meetings sponsored by Eli Lilly. YH has no conflicts of interest. TAF has received lecture fees from Eli Lilly, Meiji, Mochida, MSD, Pfizer and Tanabe-Mitsubishi, and consultancy fees from Sekisui and Takeda Science Foundation. He is diplomate of the Academy of Cognitive Therapy. He has received royalties from Igaku-Shoin, Seiwa-Shoten and Nihon Bunka Kagaku-sha. The Japanese Ministry of Education, Science, and Technology, the Japanese Ministry of Health, Labor and Welfare, and the Japan Foundation for Neuroscience and Mental Health have funded his research projects. No sources of funding were used to assist with the preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ogawa, Y., Tajika, A., Takeshima, N. et al. Mood Stabilizers and Antipsychotics for Acute Mania: A Systematic Review and Meta-Analysis of Combination/Augmentation Therapy Versus Monotherapy. CNS Drugs 28, 989–1003 (2014). https://doi.org/10.1007/s40263-014-0197-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40263-014-0197-8