
Abstract
Objective
The objective of this study was to assess the pharmacokinetic and pharmacodynamic profiles and safety of edoxaban in patients with nonvalvular atrial fibrillation (NVAF) who were hospitalized with acute heart failure (AHF).
Methods
The trough plasma concentrations of edoxaban, and the coagulation biomarkers prothrombin fragments 1 and 2 (F1+2) and d-dimer, were determined. Twenty-six patients received edoxaban 60 mg (30 mg when dose adjustment was required) and blood samples were collected immediately before oral edoxaban administration for 7 consecutive days after hospitalization and on the day of discharge.
Results
The mean observation period was 13 (range 7–46) days. Trough plasma concentrations of edoxaban were constant from day 2 onwards. On day 1, the variation was greater owing to the differing intervals between the last edoxaban dose and day 1 blood collection. Trough plasma concentrations were higher in patients with reduced creatinine clearance (≤ 50 mL/min). Median values for F1+2 and d-dimer remained within normal ranges throughout the study. There were no drug discontinuations, and no serious adverse events were reported.
Conclusions
This is the first study of edoxaban pharmacokinetics and pharmacodynamics in patients with NVAF and AHF, and shows that the pharmacokinetic and pharmacodynamic profiles of edoxaban were constant during hospitalization. Thus, even in patients with NVAF and AHF, edoxaban anticoagulation therapy with guided dose adjustment is considered to be a safe and appropriate intervention. In particular, patients with reduced creatinine clearance should adhere to dose adjustment criteria.
Clinical Trial Registration
jRCTs031190006 (Japan Registry of Clinical Trials), 5 April, 2019 retrospectively registered.
Similar content being viewed by others


Embolic prophylaxis with anticoagulant drugs is required in patients with atrial fibrillation (AF) and heart failure (HF) but HF may alter the pharmacokinetic (PK) and pharmacodynamic (PD) profiles of direct-acting oral anticoagulants (DOACs). | |
This was the first study to assess the PK and PD profiles and safety of edoxaban in patients with non-valvular (NV) AF who were hospitalized with acute HF. | |
The PK and PD profiles of edoxaban were found to be constant from Day 2 onwards in patients with NVAF and acute HF, suggesting that appropriate stroke prevention with edoxaban is feasible at the current dose regimen. | |
These findings may encourage enhanced confidence in the clinical pharmacology of DOACs in this setting; however, additional research with other DOACs is required. |
1 Introduction
Worldwide, about 26 million people have heart failure (acute and chronic), and this prevalence is increasing each year [1, 2]. In Japan, approximately 40% of patients with acute heart failure also have a history of atrial fibrillation (AF) [3, 4]. Although these findings are generally similar to those from the USA and Europe [5], the US Framingham study reported that ≥ 60% of patients with heart failure also had previous or concurrent AF [6].
Owing to the high frequency of thromboembolic complications, embolic prophylaxis with anticoagulants is required in patients with AF with heart failure [7]. It is reported that heart failure is associated with a hypercoagulable state as shown by the elevations of coagulation markers, thrombin/antithrombin complex, prothrombin fragment F1 + 2 (F1+2), and d-dimers [8]. In recent years, several direct-acting oral anticoagulants (DOACs) have been approved for anticoagulation in patients with nonvalvular AF (NVAF) [9, 10]. DOACs include a direct thrombin inhibitor and factor Xa inhibitors [10], and large-scale global clinical trials have demonstrated stable antithrombotic efficacy and reduced bleeding relative to warfarin at fixed doses of these agents [11,12,13,14]. Moreover, as US data showed that heart failure complicates prothrombin time-international normalized ratio control in warfarin-treated patients, DOACs may provide appropriate antithrombotic prophylaxis for patients with NVAF and acute heart failure [14].
In acute heart failure, worsening renal function is reported in up to 30% of patients [15]. The guidelines from the European Society of Cardiology (2016) and American College of Cardiology/American Heart Association (2019) outline that DOAC dosage adjustment is required in patients with renal dysfunction [16, 17]. Japanese guidelines (2017) also suggest that DOACs should be administered cautiously, owing to renal function changes associated with alterations in NVAF pathology and treatment [18]. Indeed, pathophysiologic changes in acute heart failure may cause altered gastrointestinal blood flow and modified drug absorption in patients with concurrent renal impairment [19, 20].
There are few previous publications reporting pharmacokinetic (PK) and pharmacodynamic (PD) data for DOACs in acute heart failure per se, although some changes in rivaroxaban pharmacokinetics and apixaban pharmacodynamics in patients with NVAF and both acute and chronic heart failure have been demonstrated [21,22,23]. Edoxaban, a direct oral factor Xa inhibitor, has demonstrated stable antithrombotic activity and reduced bleeding relative to warfarin at fixed doses in global clinical trials, and is now widely used to provide antithrombotic prophylaxis in patients with NVAF [13]. As with other DOACs, the plasma concentration of edoxaban is increased in patients with low renal function, thus the dose of edoxaban should be adjusted from 60 mg to 30 mg in patients with creatinine clearance (CrCL) of 15–50 mL/min. Despite a favorable and predictable PK profile [20, 24, 25], it is unclear whether the PK and PD profiles of edoxaban remain stable over time in patients with acute heart failure. Thus, the current study was designed to evaluate the PK and PD profiles and safety of edoxaban in patients with NVAF and acute heart failure, to better characterize appropriate antithrombotic prophylaxis.
2 Methods
2.1 Study Design
This was a prospective, multicenter, uncontrolled, open-label study in hospitalized patients with NVAF and acute heart failure. The study was conducted at six institutions from February 2019 to January 2020. The study was conducted in accordance with ethical principles of the Declaration of Helsinki, International Conference on Harmonisation-Good Clinical Practice, and all applicable Japanese laws and regulations concerning clinical research. All patients, or their legal proxies, provided written informed consent for participation in the study.
Edoxaban was administered according to the Japanese labeling [26]. Edoxaban 60 mg was administered once daily. Edoxaban 30 mg was administered if any one of the following criteria for dose adjustment was met: bodyweight ≤ 60 kg; CrCL 15–50 mL/min; or concomitant use of P-glycoprotein inhibitors, such as cyclosporine, erythromycin, quinidine, or verapamil.
The definition of day 1 in the study differed between patients receiving or not receiving edoxaban before hospitalization (Electronic Supplementary Material [ESM]). For patients receiving edoxaban before hospitalization, the day of the first edoxaban administration after hospitalization was defined as day 1. For patients not receiving anticoagulants, the day of the second edoxaban administration after hospitalization was defined as day 1. The interval between the first administration and the second administration was ≥ 12 h. Blood collection in all patients was performed just before oral edoxaban administration on day 1. Additional blood samples were collected immediately before oral edoxaban administration for seven consecutive days after hospitalization. The final blood sample was collected on the day of discharge, or when the investigator determined that the patient had entered the clinically stable phase of heart failure and observation could be stopped. Edoxaban was administered at a set time so that the dosing interval during hospitalization was 24 h, and medication time and blood sampling time were recorded. There were no restrictions regarding water intake.
2.2 Study Participants
2.2.1 Inclusion Criteria
The study included patients aged ≥ 20 years with NVAF who were hospitalized with acute heart failure (including acute exacerbations of chronic heart failure). Eligible patients were either receiving edoxaban administration at the time of obtaining informed consent or agreed to commence edoxaban therapy after obtaining informed consent and were considered suitable for oral drug administration.
2.2.2 Exclusion Criteria
The principal exclusion criteria comprised: oral anticoagulant therapy, other than edoxaban, at the time of hospital admission; previous hypersensitivity to edoxaban; acute bacterial endocarditis; renal failure (CrCL < 15 mL/min, calculated using the Cockcroft-Gault equation); dual antiplatelet therapy; cardiopulmonary arrest or cardiogenic shock; gastrointestinal hemorrhage or major hemorrhage (International Society on Thrombosis and Haemostasis criteria [27]) within 4 weeks of enrollment; unlikely to complete the study (for example, because of advanced malignancy); pregnancy; participation in another clinical trial; or judged by the principal investigator to be inappropriate for the study. Combination therapy with anticoagulants (e.g., warfarin and other DOACs) was prohibited.
2.3 Study Endpoints
The PK endpoints were trough plasma edoxaban concentrations from day 1 to day 7 and the final blood sample, and ratios of trough plasma edoxaban concentration on each day to that of the final blood sample. Pharmacodynamic endpoints included the change in the coagulation biomarkers, F1+2, and d-dimer levels throughout the study. The methods for measuring edoxaban, F1+2, and d-dimer have been reported previously [28]. In brief, plasma edoxaban concentrations were measured via liquid chromatography-tandem mass spectrometry solid-phase extraction (SCIEX, Framingham, MA, USA) at Shin Nippon Biomedical Laboratories, Ltd. (Wakayama, Japan). d-dimer and F1+2 were measured using a latex immunoturbidimetric assay (KAINOS Laboratories, Inc., Tokyo, Japan) and an enzyme-linked immunosorbent assay (Siemens Healthineers AG, Erlangen, Germany), respectively at SRL Medisearch Inc. (Tokyo, Japan).
Other parameters evaluated were mortality (including cardiovascular mortality); stroke (including ischemic or hemorrhagic stroke, but excluding transient ischemic attack) and systemic embolism; intracranial hemorrhage; and major bleeding (fatal bleeding, symptomatic intramuscular bleeding, or hemoglobin reduction of ≥ 2 g/dL [or hematocrit decrease of ≥ 6%] and clinically evident hemorrhage requiring transfusion). Safety was assessed via the occurrence of adverse events, classified using the Medical Dictionary for Regulatory Activities/Japanese version 22.0, and via changes in laboratory test values.
2.4 Statistical Analyses
The target sample size was set at 30 based on feasibility. Assuming intra-individual coefficient variations of 0.3–0.5 and geometric mean ratios of trough plasma edoxaban concentration to that of the final blood sample to be 0.5–2.0, this number of study participants allowed trough plasma edoxaban concentrations to be analyzed with a degree of accuracy.
Summary statistics were calculated for all PK and PD endpoints. For the PK endpoint of trough edoxaban ratio, the geometric least-squares mean ratios on each day to that of final blood samples and their two-sided 90% CIs were calculated using a linear mixed model, with the time point as the fixed effect and the study subject as the random effect. All statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA).
3 Results
Demographic and baseline characteristics for the analysis population (N = 26) are shown in Table 1. As it was difficult to recruit patients who met the inclusion criteria during the enrollment period (February 2019–January 2020), only 26 patients were registered and enrollment was completed without reaching the target sample size (N = 30). All 26 enrolled patients completed the study. Overall, 69.2% of patients were male, mean age was 71 years, mean bodyweight was 64.9 kg, and 12 patients (46.2%) weighed 60 kg or less. Only 13 patients (50.0%) had normal renal function (CrCL > 50 mL/min), whereas the other 13 patients (50.0%) had moderate or greater renal dysfunction (CrCL 15–50 mL/min). Seven patients (26.9%) had a body weight ≤ 60 kg and CrCL ≤ 50 mL/min. Persistent AF was the most frequent AF classification (38.5%), followed by paroxysmal AF (34.6%). A total of 21 patients (80.8%) had not been previously hospitalized for heart failure. Most patients (61.5%) had heart failure with reduced ejection fraction, the majority (88.5%) had stage C heart failure (American College of Cardiology Foundation/American Heart Association), and most (61.5%) had a clinical scenario 2 (ESM). At registration, frequently administered medications for heart failure were diuretics (82.6% of patients), β-blockers (56.5%), and angiotensin-converting enzyme inhibitors (47.8%).
Altogether, five patients (19.2%) were treated with edoxaban 60 mg and 21 patients (80.8%) received a dosage of 30 mg; one patient had edoxaban dosage modification during the study, from 30 mg (day 1) to 60 mg (day 2), and then 30 mg from day 4 onwards; for our analyses, this patient was categorized as the 30-mg dose. The mean observation period was 13 (range 7–46) days.
A total of 13 patients (50%) had received edoxaban before hospitalization, all at a dose of 30 mg. In these cases, the last pre-hospital dose of edoxaban was administered 12–40 h before edoxaban administration on study day 1.
3.1 PK Endpoints
Trough plasma concentrations of edoxaban from days 1 to 7 and the final blood sample are shown in Fig. 1 and the ESM. Edoxaban trough concentrations were constant from day 2 onwards: median (interquartile range) was 27.4 (13.9–49.0) ng/mL, 26.8 (16.0–44.2) ng/mL, 21.2 (16.7–41.4) ng/mL, and 24.2 (19.8–40.0) ng/mL on day 1, day 2, day 7, and at the final blood sample point, respectively. The variation was greatest on day 1, when trough plasma edoxaban concentrations tended to decrease in line with the increase in time interval between the last pre-study drug administration and day 1 blood collection (ESM). The geometric least-square mean ratios of trough plasma edoxaban concentration on each day to that of the final blood sample ranged from a minimum of 0.905 to a maximum of 0.987 between day 1 and day 7 (ESM).

Trough plasma edoxaban concentrations during the administration period (all patients; N = 26). Data are presented as box-and-whisker plots, in which the rhombus represents the mean, the lower and higher ends of the box represent Q1 and Q3, respectively, the horizontal line within each box represents the median, the bars represent 90th and 10th percentiles, and the dots represent 95th and 5th percentiles
Except for day 1, median trough plasma edoxaban concentrations were almost the same and stable, regardless of the history of edoxaban use before hospitalization (Fig. 2). On day 1, median trough plasma edoxaban concentration was higher in patients without a history of edoxaban use before hospitalization; in these patients, the interval between the last edoxaban dose and day 1 blood collection was shorter than in patients who were receiving edoxaban before hospitalization (ESM).

Trough plasma edoxaban concentrations according to history of edoxaban use before hospitalization. Data are presented as box-and-whisker plots, in which the rhombus represents mean, the lower and higher ends of the box represent Q1 and Q3, respectively, the horizontal line within each box represents the median, the bars represent 90th and 10th percentiles, and the dots represent 95th and 5th percentiles
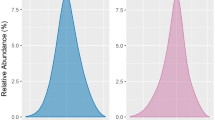
Median trough plasma edoxaban concentration was higher in the 30-mg group than in the 60-mg group (Fig. 3a). When patients treated with 30 mg were stratified by renal function (CrCL ≤ 50 mL/min or > 50 mL/min), patients with CrCL ≤ 50 mL/min tended to have higher PK values (Fig. 3b). Patient-level data are shown in the ESM.

Trough plasma edoxaban concentrations: a according to edoxaban dosage; and b according to edoxaban dosage and creatinine clearance (CrCL). Data are presented as box-and-whisker plots, in which the rhombus represents mean, the lower and higher ends of the box represent Q1 and Q3, respectively, the horizontal line within each box represents the median, the bars represent 90th and 10th percentiles, and the dots represent 95th and 5th percentiles
3.2 PD Endpoints
Median values for prothrombin F1+2 (Fig. 4a) and d-dimer (Fig. 4b) remained within normal ranges throughout the study. Dose-specific data are shown in the ESM.

Effects of edoxaban on pharmacodynamic parameters (all patients; N = 26). a Prothrombin fragments 1 and 2 (F1+2); dashed lines indicate the normal range (69–229 pmol/L [28]). b d-dimer levels; the dashed line indicates the standard threshold value (< 1.0 μg/mL [28]). Data are presented as box-and-whisker plots, in which the rhombus represents mean, the lower and higher ends of the box represent Q1 and Q3, respectively, the horizontal line within each box represents the median, the bars represent 90th and 10th percentiles, and the dots represent 95th and 5th percentiles
3.3 Other Parameters and Safety
There were no deaths (including cardiovascular mortality), or cases of stroke (including ischemic or hemorrhagic stroke, but excluding transient ischemic attack), systemic embolism, intracranial hemorrhage, or major bleeding during the study. Adverse events occurred in 11 patients, and primarily comprised gastrointestinal disorders (n = 4: abdominal discomfort [n = 1], constipation [n = 1], isolated rectal ulcer syndrome [n = 1], and nausea [n = 1]). One adverse event, a case of elevated protein induced by vitamin K absence or antagonist-II, was considered causally related to edoxaban. There were no serious adverse events, including deaths, and no adverse reactions that led to discontinuation of edoxaban during the study.
4 Discussion
Given the marked heterogeneity of patients with acute heart failure presentation, it is important to carefully assess the potential for any PK variability in the drugs used during clinical treatment. In this study, which provides the first data from an investigation of edoxaban pharmacokinetics and pharmacodynamics in patients with NVAF and acute heart failure, trough plasma concentration of edoxaban varied on day 1 (owing to the differences in time from the last edoxaban dose) but were constant from day 2 onwards. It was found that edoxaban pharmacokinetics (trough values) from day 2 remained stable, even in patients with early acute heart failure who started new treatment with edoxaban, and no serious adverse events occurred.
Importantly, patients with NVAF, including those with acute heart failure, have a high risk of cerebral infarction, and appropriate anticoagulant therapy should be given to prevent such injury occurring [29, 30]. However, there is a paucity of published data regarding changes in the pharmacokinetics and pharmacodynamics of DOACs in patients with acute heart failure. Indeed, the heart failure disease category includes both acute and chronic heart failure, and in a previous study of rivaroxaban, PK and PD (F1+2, d-dimer, and thrombin/antithrombin complex) profiles were similar in patients with acute or chronic heart failure [21]. It was also reported that the PK and PD profiles of rivaroxaban were similar in patients with heart failure compared with healthy subjects; however, some changes in the rivaroxaban area under the plasma concentration–time curve and clearance parameters have been observed, which are likely due to reduced renal and hepatic function associated with heart failure [21, 22]. Another study showed that the PD profile (i.e., intrinsic factor Xa activity) of apixaban in patients with NVAF was affected by heart failure [23].
In the present study, it was considered that edoxaban could be used safely, either after previous continuous edoxaban administration or when a new treatment schedule was started. Altogether, the PK and PD profiles of edoxaban were consistent with those in the ENGAGE AF-TIMI 48 trial, in which the efficacy and safety of edoxaban were confirmed in Asian patients with NVAF [31]. In that trial, trough plasma edoxaban concentrations in Asian patients ranged from 13.9 to 47.4 ng/mL (interquartile range), and edoxaban dosage adjustments prevented elevated drug concentrations and facilitated patient risk management regarding bleeding [31]. In the present study, interquartile ranges of trough plasma edoxaban concentrations were similar to those of the Asian patients in the ENGAGE AF-TIMI 48 trial throughout the study period. Moreover, in the overall population of the ENGAGE AF-TIMI 48 study [13], approximately 60% of patients had heart failure, compared with 100% in the current study; nevertheless, blood edoxaban concentrations were not notably different between studies. Therefore, it is considered that administration of edoxaban may reduce the risks of bleeding, stroke, or systemic embolic events in patients with NVAF with acute heart failure to the same extent as in patients with NVAF without acute heart failure.
Interestingly, the KYU-RABLE study in Japanese patients with NVAF undergoing catheter ablation confirmed the clinical utility of continued periprocedural edoxaban therapy; plasma concentrations of the coagulation biomarkers d-dimer and F1+2 were unchanged and remained within the normal range (< 1.0 μg/mL for d-dimer and 69–229 pmol/L for F1+2) [28]. In the current study, median plasma concentrations of the coagulation biomarkers were also within the normal range.
Although data for DOACs have been limited, there have been multiple reports showing irregular pharmacokinetics of other drugs in patients with acute heart failure [32]. For example, the peak plasma tolvaptan concentration after administration of 15 mg in patients with heart failure was 1.9 times higher than that in healthy people, and the area under the plasma concentration–time curve was 3.4 times higher. It has been reported that this may be due to reduced drug clearance and reduced volume of distribution in patients with heart failure [33]. Of potentially major clinical relevance, there are also reports of patients with heart failure with a significantly prolonged elimination half-life (t½) for oral furosemide (+ 70%); significantly reduced clearance (− 50%) after intravenous furosemide administration, although volume of distribution and t½ were similar to values in controls; significantly shorter t½ (− 44%) for carvedilol; and increased values for time to reach peak plasma concentration (+ 67%) and t½ (+ 130%), and reduced clearance (− 75%), after oral enalapril administration in patients with heart failure [32]. Although the prothrombin time-international normalized ratio is known to be unstable when warfarin is used in patients with heart failure [14], the results from our study show that edoxaban pharmacokinetics and pharmacodynamics are not affected by acute heart failure.
The median trough plasma edoxaban concentration was greater in the 30-mg group than in the 60-mg group, for which there are two possible explanations: pathophysiologic aspects of acute heart failure per se or differences in renal function. In the 30-mg vs 60-mg group, a smaller proportion of patients were male (61.9% vs 100.0%), patients were older (mean age 75 vs 57 years), had a lower body mass index (mean 23.6 vs 27.2 kg/m2), and a smaller proportion of patients (57.1% vs 80.0%) had heart failure with reduced ejection fraction. Overall, 13/26 patients (50.0%) had a CrCL of 15–50 mL/min, and therefore required an edoxaban dose adjustment to 30 mg, as per the Japanese labeling [26]; other 8/26 patients (30.8%) also received edoxaban 30 mg. Importantly, a CrCL of 15–50 mL/min vs > 50 mL/min was associated with greater trough plasma edoxaban concentrations. Thus, it should be noted that the label-recommended dose reduction in edoxaban is crucial in patients with impaired renal function.
Compared with the other study periods, the trough plasma edoxaban concentration on day 1 varied widely. This is because the definition of day 1 varied; the time interval between the last edoxaban dose on day 1 and blood sampling ranged from 12.8 to 26.9 h in patients who did not receive edoxaban before hospitalization, and from 23.5 to 40.3 h in patients who received edoxaban before hospitalization. This explains the variability in plasma edoxaban concentrations on day 1. After day 2, plasma edoxaban concentration remained constant, despite treatment for acute heart failure and entry into the clinically stable phase of heart failure. This suggests that the pathophysiological processes underlying acute heart failure do not affect the pharmacokinetics of edoxaban. Indeed, CrCL levels did not show any remarkable changes during this study period (data not shown).
Regarding study limitations, the sample size was small and, as such, analyses according to the different presentations of acute heart failure were not possible. Further, generalizability of the results to patients with severe heart failure is limited, as the study included only three patients with American College of Cardiology Foundation/American Heart Association stage D heart failure. As this study was designed to evaluate patients who received emergency hospitalization, it was not always possible to obtain prior medical data relating to previous hospitalizations for acute heart failure. Instead, in this study, the time of discharge (i.e., the time when heart failure management by hospitalization became unnecessary) was regarded as the time when the pathological condition of heart failure was stable, which was set as a reference for the final PD levels. No specific data were available for patients with dehydration or acute kidney injury, and these populations may warrant further investigation.
5 Conclusions
The PK and PD profiles of edoxaban showed no marked deviations in patients with NVAF and acute heart failure compared with those without heart failure. Thus, even in this patient population, edoxaban anticoagulation therapy with guided dose adjustment is considered safe and can be recommended. In particular, patients with reduced CrCL should adhere to dose adjustment criteria.
References
Shiga T, Suzuki A, Haruta S, Mori F, Ota Y, Yagi M, et al. Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan. ESC Heart Fail. 2019;6(3):475–86.
Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017;3(1):7–11.
Fujii N, Naito K, Nakahara N, Nakano A, Takagi S. Clinical characteristics and outcomes in super-elderly patients (>85 years) with heart failure: single center observational study in Japan. Acute Med Surg. 2014;1(2):76–82.
Horiuchi Y, Tanimoto S, Latif A, Urayama KY, Aoki J, Yahagi K, et al. Identifying novel phenotypes of acute heart failure using cluster analysis of clinical variables. Int J Cardiol. 2018;262:57–63.
Sato N, Kajimoto K, Asai K, Mizuno M, Minami Y, Nagashima M, et al. Acute decompensated heart failure syndromes (ATTEND) registry: a prospective observational multicenter cohort study: rationale, design, and preliminary data. Am Heart J. 2010;159(6):949-55.e1.
Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, et al. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016;133(5):484–92.
Thomas I, EncisoSilva J, Schlueter M, Greenberg B. Anticoagulation therapy and NOACs in heart failure. Handb Exp Pharmacol. 2017;243:515–35.
Jafri SM, Mammen EF, Masura J, Goldstein S. Effects of warfarin on markers of hypercoagulability in patients with heart failure. Am Heart J. 1997;134(1):27–36.
Khattak F, Alam MB, Paul TK, Rijal S, Wazir S, Lavie CJ, et al. Antithrombotic therapy in nonvalvular atrial fibrillation: consensus and challenges. Am J Med Sci. 2018;355(5):467–76.
Dobesh PP, Fanikos J. Direct oral anticoagulants for the prevention of stroke in patients with nonvalvular atrial fibrillation: understanding differences and similarities. Drugs. 2015;75(14):1627–44.
Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–92.
Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–91.
Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093–104.
Nelson WW, Desai S, Damaraju CV, Lu L, Fields LE, Wildgoose P, et al. International normalized ratio stability in warfarin-experienced patients with nonvalvular atrial fibrillation. Am J Cardiovasc Drugs. 2015;15(3):205–11.
Damman K, Valente MA, Voors AA, O’Connor CM, van Veldhuisen DJ, Hillege HL. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014;35(7):455–69.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC), developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200.
January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(1):104–32.
Tsutsui H, Isobe M, Ito H, Ito H, Okumura K, Ono M, et al. JCS 2017/JHFS 2017 guideline on diagnosis and treatment of acute and chronic heart failure: digest version. Circ J. 2019;83(10):2084–184.
Kida K, Shibagaki Y, Tominaga N, Matsumoto N, Akashi YJ, Miyake F, et al. Efficacy of tolvaptan added to furosemide in heart failure patients with advanced kidney dysfunction: a pharmacokinetic and pharmacodynamic study. Clin Pharmacokinet. 2015;54(3):273–84.
Aspromonte N, Colivicchi F. Clinical relevance of pharmacokinetic and pharmacodynamic properties of edoxaban when treating patients with atrial fibrillation and heart failure. Expert Opin Drug Metab Toxicol. 2017;13(1):113–22.
Gheorghiade M, Thyssen A, Zolynas R, Nadar VK, Greenberg BH, Mehra M, et al. Pharmacokinetics and pharmacodynamics of rivaroxaban and its effect on biomarkers of hypercoagulability in patients with chronic heart failure. J Heart Lung Transpl. 2011;30(2):218–26.
Mueck W, Stampfuss J, Kubitza D, Becka M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin Pharmacokinet. 2014;53(1):1–16.
Ueshima S, Hira D, Tomitsuka C, Nomura M, Kimura Y, Yamane T, et al. Population pharmacokinetics and pharmacodynamics of apixaban linking its plasma concentration to intrinsic activated coagulation factor X activity in Japanese patients with atrial fibrillation. AAPS J. 2019;21(5):80.
Ogata K, Mendell-Harary J, Tachibana M, Masumoto H, Oguma T, Kojima M, et al. Clinical safety, tolerability, pharmacokinetics, and pharmacodynamics of the novel factor Xa inhibitor edoxaban in healthy volunteers. J Clin Pharmacol. 2010;50(7):743–53.
Weitz JI, Connolly SJ, Patel I, Salazar D, Rohatagi S, Mendell J, et al. Randomised, parallel-group, multicentre, multinational phase 2 study comparing edoxaban, an oral factor Xa inhibitor, with warfarin for stroke prevention in patients with atrial fibrillation. Thromb Haemost. 2010;104(3):633–41.
Savaysa (edoxaban) tablets, for oral use [prescribing information]. Daiichi-Sankyo Co., Ltd., Tokyo, Japan. 2020. https://www.info.pmda.go.jp/downfiles/ph/PDF/430574_3339002F1020_1_05.pdf. Accessed 18 Nov 2020.
Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692–4.
Takahashi N, Mukai Y, Kimura T, Yamaguchi K, Matsumoto T, Origasa H, et al. Efficacy and safety of uninterrupted periprocedural edoxaban in patients undergoing catheter ablation for atrial fibrillation: the prospective KYU-RABLE study. Circ J. 2019;83(10):2017–24.
Ozyuncu N, Gulec S, Kaya CT, Goksuluk H, Tan TS, Vurgun VK, et al. Relation of acute decompensated heart failure to silent cerebral infarcts in patients with reduced left ventricular ejection fraction. Am J Cardiol. 2019;123(11):1835–9.
Deguchi I, Osada T, Takao M. Prescription status of oral anticoagulants in patients with acute cerebral infarction with non-valvular atrial fibrillation at the time of stroke onset. J Cardiol. 2020;75(5):544–8.
Chao TF, Chen SA, Ruff CT, Hamershock RA, Mercuri MF, Antman EM, et al. Clinical outcomes, edoxaban concentration, and anti-factor Xa activity of Asian patients with atrial fibrillation compared with non-Asians in the ENGAGE AF-TIMI 48 trial. Eur Heart J. 2019;40(19):1518–27.
Mangoni AA, Jarmuzewska EA. The influence of heart failure on the pharmacokinetics of cardiovascular and non-cardiovascular drugs: a critical appraisal of the evidence. Br J Clin Pharmacol. 2019;85(1):20–36.
Inomata T, Izumi T, Matsuzaki M, Hori M, Hirayama A; Tolvaptan Investigators. Phase III clinical pharmacology study of tolvaptan. Cardiovasc Drugs Ther. 2011;25(Suppl 1):S57–65.
Acknowledgements
We thank David Murdoch, B.Sc. (Hons), and Sally-Anne Mitchell, Ph.D., of Edanz Evidence Generation, for providing medical writing support, which was funded by Daiichi Sankyo Co., Ltd., Tokyo, Japan.
Author information
Authors and Affiliations
Contributions
TN, KK, TK, KY, AT, and TI designed the research and wrote the manuscript. TN, KK, MI, TS, NS, SD, MT, YJA, JA, and TI performed the research. TN, KK, YO, TK, KY, AT, NM, and TI planned the statistical analysis. TN, KK, YO, NM, and TI analyzed the data.
Corresponding author
Ethics declarations
Funding
This study was supported by Daiichi Sankyo Co., Ltd., Tokyo, Japan.
Conflict of Interest
Takeru Nabeta, Miwa Ishida, Takaaki Shiono, Norio Suzuki, Shunichi Doi, Maya Tsukahara, and Yuki Ohta have no conflicts of interest that are directly relevant to the content of this article. Keisuke Kida has received research funding from Daiichi Sankyo Co. Ltd., Terumo Corp., Novartis Pharma K.K., Amgen Astellas BioPharma K.K., and Bristol-Myers Squibb Co. Tetsuya Kimura, Keita Yamaguchi, and Atsushi Takita are employees of Daiichi Sankyo Co., Ltd. Naoki Matsumoto has received research funding from Pfizer Inc., Takeda Pharmaceutical Co., Ltd., Novartis Pharma K.K., Bayer Yakuhin Ltd., and Daiichi Sankyo Co., Ltd. Yoshihiro J. Akashi has received lecture fees from Daiichi Sankyo Co. Ltd., and scholarship funds from Medtronic Japan Co., Ltd., Abbott Japan Co., Ltd., Nihon Medi-Physics Co., Ltd., FUJIFILM Toyama Chemical Co., Ltd., and MC Co., Ltd. Junya Ako has received a speaking honorarium and research grant from Daiichi Sankyo Co., Ltd. Takayuki Inomata has received lecture fees from Daiichi Sankyo Co. Ltd., Otsuka Pharmaceutical Co., Pfizer Inc., Bristol-Myers Squibb Co., Bayer Yakuhin Ltd., Novartis Pharma K.K., and Ono Pharmaceutical Co., Ltd.
Ethics Approval
The study protocol and all related documentation were approved by the Kitasato Institute, Clinical Research Review Board (accreditation number: CRB3180002). The study was registered in the Japan Registry of Clinical Trials (No. jRCTs031190006).
Consent to Participate
All patients, or their legal proxies, provided written informed consent for participation in the study.
Consent for Publication
Not applicable.
Availability of Data and Material
The anonymized data underlying the results presented in this article may be made available to researchers upon submission of a reasonable request to the corresponding author. The decision to disclose the data will be made by the corresponding author and the funder, Daiichi Sankyo Co., Ltd. Data disclosure can be requested for 36 months from the article publication.
Code Availability
Not applicable.
Additional information
Some results from this study have been submitted as an abstract to the 85th Annual Scientific Meeting of the Japanese Circulation Society; 26–28 March, 2021; PACIFICO Yokohama Conference Center, Yokohama, Japan.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Nabeta, T., Kida, K., Ishida, M. et al. Plasma Concentration and Pharmacodynamics of Edoxaban in Patients with Nonvalvular Atrial Fibrillation and Acute Heart Failure. Clin Pharmacokinet 60, 1061–1071 (2021). https://doi.org/10.1007/s40262-021-00999-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-021-00999-y