
Abstract
Background
Use of the recombinant human granulocyte colony-stimulating factor (rhG-CSF) filgrastim accelerates neutrophil recovery following myelosuppressive chemotherapy. Since filgrastim requires multiple daily administrations, forms of rhG-CSF with a longer half life, including pegfilgrastim, have been developed. Pegfilgrastim is safe and effective in supporting neutrophil recovery and reducing febrile neutropenia after conventional chemotherapy. Pegfilgrastim has also been successfully used to support patients undergoing peripheral blood stem cell (PBSC) transplantation for haematological malignancies. To our knowledge, no cost-effectiveness analysis (CEA) of pegfilgrastim in this setting has been published yet.
Objective
We undertook a CEA to compare a single injection of pegfilgrastim versus repeated administrations of filgrastim in patients who had undergone PBSC transplantation for lymphoma or myeloma. The CEA was set in France and covered a period of 100 ± 10 days from transplant.
Methods
The CEA was designed as part of an open-label, multicentre, randomized phase II trial. Costs were assessed from the hospital’s point of view and are expressed in 2009 euros. Costs computation focused on inpatient, outpatient, and home care. Costs in the two arms of the study were compared using the Mann–Whitney test. When differences were statistically significant, multiple regression analyses were performed in order to identify cost drivers. Incremental cost-effectiveness ratios (ICER) were calculated for the major endpoints of the trial; i.e., duration of febrile neutropenia (absolute neutrophil count [ANC] <0.5 × 109/L and temperature ≥38 °C), duration of neutropenia (ANC <1.0 × 109/L and ANC <0.5 × 109/L), duration of thrombopenia (platelets <50 × 109/L and <20 × 109/L), and days with a temperature ≥38 °C). Uncertainty around the ICER was captured by a probabilistic analysis using a non-parametric bootstrap method.
Results
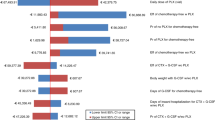
151 patients were enrolled at ten French centres from October 2008 to September 2009. The mean total cost in the pegfilgrastim arm of the study (n = 74) was €25,024 (SD 9,945). That in the filgrastim arm (n = 76) was €28,700 (SD 20,597). Pegfilgrastim strictly dominated filgrastim for days of febrile neutropenia avoided, days of neutropenia (ANC <1.0 × 109/L) avoided, days of thrombopenia (platelets <20 × 109/L) avoided, and days with temperature ≥38 °C) avoided. Pegfilgrastim was less costly and less effective than filgrastim for the number of days with ANC <0.5 × 109/L avoided and the number of days with platelets <50.0 × 109/L avoided. Taking uncertainty into account, the probabilities that pegfilgrastim strictly dominated filgrastim were 67 % for febrile neutropenia, 86 % for neutropenia (ANC <1.0 × 109/L), 59 % for thrombopenia (platelets <20 × 109/L), 86 % for temperature ≥38 °C, 32 % for neutropenia (ANC <0.5 × 109/L), and 43 % for thrombopenia (platelets <50 × 109/L). Conversely, the probability that filgrastim strictly dominated pegfilgrastim for neutropenia (ANC <0.5 × 109/L) is 5 %.
Conclusion
This study found no evidence that the use of pegfilgrastim is associated with greater cost in lymphoma and myeloma patients after high-dose chemotherapy and PBSC transplantation.




Similar content being viewed by others


References
Ljungman P, Urbano-Ispizua A, Cavazzana-Calvo M, et al. Allogeneic and autologous transplantation for haematological diseases, solid tumours and immune disorders: definitions and current practice in Europe. Bone Marrow Transpl. 2006;37(5):439–49.
Hornedo J, Sola C, Solano C, et al. The role of granulocyte colony stimulating factor (G-CSF) in the post-transplant period. Bone Marrow Transpl. 2002;29(9):737–43.
Vogel CL, Wojtukiewicz MZ, Carroll RR, et al. First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer: a multicenter, double-blind, placebo-controlled phase III study. J Clin Oncol. 2005;23(6):1178–84.
Hosing C, Qazilbash MH, Kebriaei P, et al. Fixed-dose single agent pegfilgrastim for peripheral blood progenitor cell mobilisation in patients with multiple myeloma. Br J Haematol. 2006;133(5):533–7.
Aapro MS, Bohlius J, Cameron DA, et al. 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer. 2011;47:8–32.
Martino M, Praticò G, Messina G, et al. Pegfilgrastim compared with filgrastim after high-dose melphalan and autologous hematopoietic peripheral blood stem cell transplantation in multiple myeloma patients. Eur J Haematol. 2006;77(5):410–5.
Rifkin R, Spitzer G, Orloff G, et al. Pegfilgrastim appears equivalent to daily dosing of filgrastim to treat neutropenia after autologous peripheral blood stem cell transplantation in patients with non-Hodgkin lymphoma. Clin Lymphoma Myeloma Leuk. 2010;10(3):186–91.
Castagna L, Bramanti S, Levis A, et al. Pegfilgrastim versus filgrastim after high-dose chemotherapy and autologous peripheral blood stem cell support. Ann Oncol. 2010;21(7):1482–5.
Gerds A, Fox-Geiman M, Dawravoo K, et al. Randomized phase III trial of pegfilgrastim versus filgrastim after autologus peripheral blood stem cell transplantation. Biol Blood Marrow Transpl. 2010;16(5):678–85.
Eldar-Lissai A, Cosler LE, Culakova E, et al. Economic analysis of prophylactic pegfilgrastim in adult cancer patients receiving chemotherapy. Value Health. 2008;11(2):172–9.
Lyman G, Lalla A, Barron R, et al. Cost-effectiveness of pegfilgrastim versus 6-day filgrastim primary prophylaxis in patients with non-Hodgkin’s lymphoma receiving CHOP-21 in United States. Curr Med Res Opin. 2009;25(2):401–11.
Liu Z, Doan V, Malin J, et al. The economic value of primary prophylaxis using pegfilgrastim compared with filgrastim in patients with breast cancer in the UK. Appl Health Econ Health Policy. 2009;7(3):193–205.
Numnum TM, Kimball KJ, Rocconi RP, et al. Pegfilgrastim for the prevention of febrile neutropenia in patients with epithelial ovarian carcinoma: a cost-effectiveness analysis. Int J Gynecol Cancer. 2007;17(5):1019–24.
Sebban C, Lefranc A, Perrier L, et al. A randomised phase II study of the efficacy, safety and cost-effectiveness of pegfilgrastim and filgrastim after autologous stem cell transplant for lymphoma and myeloma (PALM study). Eur J Cancer. 2012;48(5):713–20.
Journal Officiel de la République Française, arrêté du 02 janvier 2008 relatif au tarif de cession des produits sanguins labiles. JORF 2008. 0035. http://admi.net/jo/20080210/.
French National Authority for Health. L’évaluation économique à la Haute Autorité de Santé Principes et méthodes [Economic evaluation at the French National Health Authority: principles and methods]. http://www.has-sante.fr/portail/jcms/c_1003762/levaluation-economique-a-la-has-principes-et-methodes. Accessed 2011.
Claxton K, Sculpher M, McCabe C, et al. Probabilistic sensitivity analysis for NICE technology assessment: not an optional extra. Health Econ. 2005;14:339–47.
Mathew S, Adel N, Rice RD, et al. Retrospective comparison of the effects of filgrastim and pegfilgrastim on the pace of engraftment in auto-SCT patients. Bone Marrow Transpl. 2010;45:1522–7.
Staber PB, Holub R, Linkesch W, et al. Fixed-dose single administration of pegfilgrastim vs daily filgrastim in patients with haematological malignancies undergoing autologous peripheral blood stem cell transplantation. Bone Marrow Transpl. 2005;35(9):889–93.
Samaras P, Blickenstorfer M, Siciliano RD, et al. Pegfilgrastim reduces the length of hospitalization and the time to engraftment in multiple myeloma patients treated with melphalan 200 and auto-SCT compared with filgrastim. Ann Hematol. 2011;90:89–94.
Ziakas PD, Kourbeti IS. Pegfilgrastim vs. filgrastim for supportive care after autologous stem cell transplantation: can we decide? Clin Transpl. 2012;26(1):16–22.
Ballestrero A, Boy D, Gonella R, et al. Pegfilgrastim compared with filgrastim after autologous peripheral blood stem cell transplantation in patients with solid tumours and lymphomas. Ann Hematol. 2008;87(1):49–55.
Samaras P, Buset EM, Siciliano RD, et al. Equivalence of pegfilgrastim and filgrastim in lymphoma patients treated with BEAM followed by autologous stem cell transplantation. Oncology. 2010;79:93–7.
Ferrara F, Izzo T, Criscuolo C, et al. Comparison of fixed dose pegfilgrastim and daily filgrastim after autologous stem cell transplantation in patients with multiple myeloma autografted on an outpatient basis. Hematol Oncol. 2011;3:139–43.
Faucher C, Le Corroller Soriano AG, Esterni B, Vey N, et al. Randomized study of early hospital discharge following autologous blood SCT: medical outcomes and hospital costs. Bone Marrow Transpl. 2012;47(4):549–55.
McDiarmid S, Hutton B, Atkins H, et al. Performing allogeneic and autologous hematopoietic SCT in the outpatient setting: effects on infectious complications and early transplant outcomes. Bone Marrow Transpl. 2010;45(7):1220–6.
Gertz MA, Ansell SM, Dingli D, et al. Autologous stem cell transplant in 716 patients with multiple myeloma: low treatment-related mortality, feasibility of outpatient transplant, and effect of a multidisciplinary quality initiative. Mayo Clin Proc. 2008;83(10):1131–8.
McCabe C, Claxton K, Culyer AJ. The NICE cost-effectiveness threshold: what it is and what that means. Pharmacoeconomics. 2008;26:733–44.
National Institute for Health and Clinical Excellence. Assessing cost effectiveness. http://www.nice.org.uk/media/68D/29/The_guidelines_manual_2009_-_Chapter_7_Assessing_cost_effectiveness.pdf. Accessed 23 Jan 2013.
Lee SJ, Klar N, Weeks JC, et al. Predicting costs of stem-cell transplantation. J Clin Oncol. 2000;18:64–71.
Bennett C, Waters T, Stinson T, et al. Valuing clinical strategies early in development: a cost analysis of allogeneic peripheral blood stem cell transplantation. Bone Marrow Transpl. 1999;24:555–60.
Schulman KA, Birch R, Zhen B, et al. Effect of CD34+ cell dose on resource utilization in patients after high-dose chemotherapy with peripheral-blood stem-cell support. J Clin Oncol. 1999;17:1227–33.
Acknowledgment
The authors are grateful to the coordinating staff, physicians, clinical research assistants and nursing staff involved in this study as well as to the chief financial officers and pharmacists of participating centres. The authors also gratefully acknowledge Magali Hureau, Gérard de Pouvourville and Patrick Sylvestre Baron for feedback on a preliminary version of this paper. The authors thank Amgen France for its support in conducting this study. The authors would like to thank the referees for their insightful comments and suggestions. Rob Stepney, medical writer, Charlbury, UK, assisted with the final editing of the manuscript.
Source of financial support:
The study received research support from AMGEN Inc., Thousand Oaks, CA, USA. AMGEN had no involvement in the design, in the data management, in the analysis, or in the interpretation and reporting of this study.
Authors’ contributions
LP, AL, DP, CS designed the study, acquired and interpreted the clinical and cost data, undertook the statistical analysis, and prepared the manuscript. PQ, AST, BF, PB, PM, JOB, SL, FJ, DE participated in clinical data acquisition and analysis. CS, CP participated in the statistical analysis. CS is guarantor for the overall content of this manuscript.
Authorisation of the Commission Nationale de l’Informatique et des Libertés (CNIL):
1257249.
Unique Protocol ID:
PALM.
Secondary IDs:
ET2007–113.
Trial registration number:
NCT00794261.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Perrier, L., Lefranc, A., Pérol, D. et al. Cost Effectiveness of Pegfilgrastim Versus Filgrastim After High-Dose Chemotherapy and Autologous Stem Cell Transplantation in Patients with Lymphoma and Myeloma. Appl Health Econ Health Policy 11, 129–138 (2013). https://doi.org/10.1007/s40258-013-0011-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-013-0011-7