
Abstract
Introduction
Chronic kidney disease (CKD) has been associated with accelerated retinal neurodegeneration. The purpose of this study is to evaluate the association between retinal neurodegeneration and the best-corrected visual acuity (BCVA) decline in patients with CKD.
Methods
Post hoc analysis of two prospective studies. Patients with CKD stage ≥ 3 were enrolled. Macular thickness, peripapillary retinal nerve fiber layer (pRNFL) thickness, and macular ganglion cell complex (GCC) thickness were measured by optical coherence tomography. Eyes were classified into three groups: Group 1, no GCC defect; Group 2, GCC defect confined to parafoveal area; and Group 3, GCC defects extending beyond the parafoveal area. Each group was matched for age, sex, axial length, lens status, and cataract grading.
Results
A total of 120 eyes (40 eyes in each group) from 120 patients (age 63.0 ± 10.3 years) were included. The logMAR BCVA was 0.076 ± 0.101, 0.100 ± 0.127, and 0.196 ± 0.191 in Group 1, 2, and 3, respectively. Group 3, but not Group 2, had a significantly worse BCVA than Group 1. In simple linear regression, parafoveal inner retinal thickness, pRNFL thickness, presence of pRNFL defect, GCC thickness, GCC global loss volume, GCC focal loss volume, and GCC defect extending beyond parafoveal area were associated with BCVA. Central subfield retinal thickness (CRT), parafoveal full retinal thickness, and parafoveal outer retinal thickness were not associated with BCVA. In backward stepwise linear regression, age and GCC defects extending beyond the parafoveal area were factors associated with BCVA. Moreover, GCC defect extending beyond parafoveal area was connected with worse BCVA in both phakic and pseudophakic subgroups.
Conclusions
GCC defect extending beyond parafoveal area could be an independent biomarker associated with decreased BCVA in patients with CKD. However, macular thinning measured by CRT or parafoveal full retinal thickness might have low discriminative power in determining BCVA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Macular thinning is common in patients with chronic kidney disease (CKD) and has been associated with retinal neurodegeneration. However, it is unclear to what extent retinal neurodegeneration might cause visual acuity decline in CKD patients. |
It is also unknown whether macular thinning could be used as a surrogate biomarker for predicting visual acuity decline. |
What was learned from the study? |
Retinal neural parameters, including parafoveal inner retinal thickness, peripapillary retinal nerve fiber layer-derived parameters, and ganglion cell complex-derived parameters were associated with best-corrected visual acuity (BCVA) in patients with CKD. |
However, macular thinning, measured by full retinal thickness, might have low discriminative power in determining BCVA. |
Introduction
Chronic kidney disease (CKD) is a prevalent disease affecting around 10% of the general population [1]. Its prevalence could raise to 44% for the elderly aged > 70 years or 36% for hypertensive patients [1]. Patients with CKD could have increased risk of visual impairment by three- to seven-fold [2, 3]. The causes of the visual decline may be attributed to either definite ocular diseases, such as cataract, glaucoma, age-related macular degeneration (AMD), diabetic retinopathy (DR), and other retinopathies [2, 3], or non-specific ocular pathologies such as retinal microvascular degeneration and retinal neurodegeneration [4,5,6].
Although retinal neurodegeneration has been reported in prior studies [4,5,6], it is unclear to what extent it might cause visual acuity decline in CKD patients. Ganglion cell complex (GCC) thickness on spectral domain optical coherence tomography (OCT) is a sensitive biomarker for retinal ganglion cells (RGCs) loss and can be used as an indicator of the retinal neurodegeneration [7,8,9,10,11]. Macular thinning is a common finding in patients with CKD, and has been associated with retinal neurodegeneration [4,5,6]. However, it is unknown whether GCC defects or macular thinning could be used as a surrogate biomarker for predicting visual acuity decline in CKD patients.
The purpose of this study was to evaluate the association between the retinal neurodegeneration and the best-corrected visual acuity (BCVA) decline in patients with CKD, particularly in patients without definite causes of visual loss. We hypothesize that the extensive RGC loss over central macula, represented by GCC defects extending beyond the parafoveal area, could be a factor contributing to visual decline. Subgroup analyses were also conducted in phakic and pseudophakic eyes, as these might help to predict the visual outcome of cataract surgery in patients with CKD.
Methods
This study was a post hoc analysis of the OCT images dataset obtained from two prospective studies [4, 12] that evaluated retinal microvascular changes and neurodegeneration in patients with CKD at a tertiary hospital, Keelung Chang Gung Memorial Hospital, in Taiwan. This study followed the tenets of the Declaration of Helsinki and was approved by the Chang Gung Memorial Hospital Institutional Review Board (IRB No.: 202200738B0). Patients with CKD stage ≥ 3 were enrolled between August 2017 and July 2019. CKD was diagnosed if the patient had structural or functional abnormalities of their kidneys and a decrease of estimated glomerular filtration rate (eGFR) to < 60 mL/min/1.73 m2 for > 3 months [13].
Demographic data were collected through a standardized questionnaire. BCVA was measured by a standard Snellen chart light box at 6 m, and then converted to the logarithm of the minimum angle of resolution (logMAR) for calculation. A noncontact tonometer (NT-3000; Nidek, Tokyo, Japan) and a IOLMaster (Carl Zeiss Meditec, Jena, Germany) were used for intraocular pressure (IOP) and axial length measurements, respectively. The cataract was graded through slit-lamp biomicroscopy using the Lens Opacities Classification System III (LOCS III) with nuclear opalescence (Grade 1–6), cortical cataract (Grade 1–5), and posterior subcapsular cataract (Grade 1–5) [14].
The exclusion criteria were (1) the presence of any ocular diseases that could affect the GCC thickness, including glaucoma, DR, AMD, macular pucker, retinal vessel occlusion, and optic nerve disease; (2) high myopia (myopia < –6 D or axial length > 26 mm); (3) dense cataract or media opacity obscuring vision; (4) poor quality of OCT image [signal strength index (SSI) < 40 or presence of significant artifacts]; (5) IOP > 21 mmHg; (6) any prior ocular surgeries except uncomplicated cataract surgery; and (7) pregnancy.
Retinal Neural Parameters
A spectral domain OCT (RTVue XR Avanti; Optovue, Fremont, CA, USA) was used to obtain all retinal neural parameters. Retinal thicknesses were provided in Early Treatment Diabetic Retinopathy Study thickness charts. Central subfield retinal thickness (CRT) was the average thickness within central 1-mm circle. Parafoveal area was defined as the 1-mm round annulus area extending from the 1-mm circle above. Inner retinal thickness was measured from internal limiting membrane to inner plexiform layer (IPL). Outer retinal thickness was measured from IPL to retinal pigment epithelium. Peripapillary retinal nerve fiber layer (pRNFL) thickness was measured with an optic nerve head (OHN) scan over a 3.45-mm-diameter circle centered on the ONH. GCC over macula was measured by scanning a region of 7 × 7 mm2 centered on a point 1 mm temporal to the fovea. The GCC consists of the nerve fiber layer (NFL), ganglion cell layer (GCL), and IPL. The average GCC thickness, GCC global loss volume (GLV, %), and GCC focal loss volume (FLV, %) within a 6-mm circle were calculated by the OCT machine. The machine also provides color-coded Normative Database (NDB) Reference Maps for pRNFL and GCC, showing regions where the thickness is normal (green, p value > 5%), borderline (yellow, p value between 1 and 5%), and outside of normal (red, p value < 1%) compared to the normative database. In this study, a GCC defect was defined as the region of GCC thickness outside of normal (red). The presence of pRNFL defects meant that pRNFL thickness is outside of normal (red) in any of the eight sectors.
Classification of GCC Defect
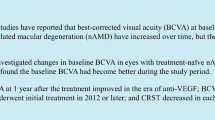
Patients were classified into three groups according to the extensiveness of their GCC defect (Fig. 1A–C): Group 1, no GCC defect; Group 2, GCC defect confined to parafoveal area; and Group 3, GCC defects extending beyond parafoveal area. Because this study focused on the RGC loss over central macula, eyes with perifoveal GCC defects that did not connect to a parafoveal defect (Fig. 1D) were excluded in the statistical analysis. A 3-mm-diameter circle centered on fovea was drawn on the GCC NDB Reference Map using Photoshop CS6 (v.13.0; Adobe Systems, San Jose, CA, USA) to indicate the boundary of the parafoveal area.

Classification of ganglion cell complex (GCC) defects using GCC Normative Database Reference Maps: red color indicates GCC defect where thickness is outside normal range, the dark-blue circle indicates the boundary of the parafoveal area. A No GCC defect. B GCC defect confined to parafoveal area. C GCC defects extending beyond the parafoveal area. D Presence of perifoveal GCC defect without connecting to a parafoveal defect
Statistical Analysis
Eyes in each group were matched by age, sex, axial length, lens status (phakic vs. pseudophakic), and cataract grading. Eyes that successfully matched across all three groups were included for statistical analysis. Only one eye from each patient could be used for analysis. Clinical characteristics were compared between groups. Continuous variables were analyzed with one way analysis of variance (ANOVA), while categorical variables were analyzed using the chi-square test. Bonferroni post hoc multiple comparison tests were applied to compare the groups. Moreover, a simple linear regression model (Model 1) was used to determine the association of each retinal neural parameter with logMAR BCVA, while a multiple linear regression model (Model 2) was used to determine the above association after controlling for age, sex, axial length, lens status, and SSI. Then, age, parafoveal inner retinal thickness, presence of pRNFL defect, and GCC defect extending beyond the parafoveal area were added into a multiple linear regression model using a backward stepwise method (Model 3) to determine whether these were independent factors. In subgroup analysis, we compared the logMAR BCVA among patients with or without GCC defects extending beyond parafoveal area using the independent sample t test in phakic and pseudophakic eyes, respectively. All statistical analyses were calculated using IBM SPSS Statistics v.26.0 (IBM, Armonk, NY, USA). A two-tailed p value of < 0.05 was considered statistically significant.
Results
We identified 447 eligible eyes from 249 patients (110 female, 139 male; mean age ± standard deviation, 62.9 ± 10.0) for this study. Fifty-one eyes had been exuded due to the presence of macular pucker (20 eyes), high myopia (11 eyes), RNFL SSI < 40 (14 eyes), GCC SSI < 40 (4 eyes), and the presence of other retinal disease (2 eyes). Figure 2 shows the flowchart and the number of eligible eyes in each group. One hundred and twenty eyes from 120 patients (39 female, 81 male; mean age, 63.0 ± 10.3 years) were successfully matched and divided into three 40-patient groups. The mean eGFR was 28.1 ± 20.9 mL/min/1.73 m2. Figure 3 illustrates the representative patients in each group.

Flowchart of this study

Representative cases from each group. A–D Group 1: a 63-year-old woman with diabetes, hypertension, and chronic kidney disease (CKD) stage 3. The best corrected visual acuity (BCVA) was 20/20 in her left eye. No significant abnormalities were found in A color fundus photo, B central subfield retinal thickness (CRT) and parafoveal full retinal thickness, C peripapillary retinal nerve fiber layer (pRNFL) thickness, and D ganglion cell complex (GCC) thickness. E–H Group 2: a 66-year-old woman with diabetes, hypertension, and CKD stage 3. The BCVA was 20/20 in her right eye. E Normal fundus. F Decreased CRT and parafoveal full retinal thickness. G Normal pRNFL thickness. F GCC defect confined to parafoveal area. I–L Group 3: a 64-year-old man with gout, hyperlipidemia, and CKD stage 3. The BCVA was 20/40 in his right eye. I Normal fundus. J Decreased CRT and parafoveal full retinal thickness. K Decreased pRNFL thickness with pRNFL defect over inferior-temporal sector. L GCC defect extending beyond the parafoveal area
Table 1 presents the comparison of the demographic data and the clinical characteristics among the three groups. Comparing to Group 1, both Group 2 and Group 3 had significantly lower proportions of CKD stage 3 (p value 0.660 and 0.006, respectively), decreased CRT (p value < 0.001 and < 0.001, respectively), decreased parafoveal full retinal thickness (p value 0.007 and < 0.001, respectively), decreased prafoveal inner retinal thickness (p value < 0.001 and < 0.001, respectively), decreased GCC thickness (p value < 0.001 and < 0.001, respectively), increased GCC GLV (p value 0.002 and < 0.001, respectively), and increased GCC FLV (p value 0.047 and < 0.001, respectively). However, only Group 3 had significantly lower eGFR (p value 0.001), decreased parafoveal outer retinal thickness (p value < 0.001), decreased pRNFL thickness (p value < 0.001), and a higher proportion of pRNFL defect (p value < 0.001) when compared to Group 1.
The logMAR BCVA was 0.076 (equivalent to 20/24) ± 0.101 in Group 1, 0.100 (equivalent to 20/25) ± 0.127 in Group 2, and 0.196 (equivalent to 20/31) ± 0.191 in Group 3 (Table 1). Statistical analysis showed that Group 3 appeared to have significantly worse logMAR BCVA than in Group 1 and Group 2. However, no significant difference was noticed between Group 1 and Group 2.
Table 2 shows the results of the linear regression analysis. The simple regression model (Model 1) showed that parafoveal inner retinal thickness (p = 0.001), pRNFL thickness (p = 0.009), presence of pRNFL defect (p < 0.001), GCC thickness (p = 0.003), GCC GLV (p < 0.001), GCC FLV (p < 0.001), and GCC defects extending beyond the parafoveal area (p < 0.001) were factors associated with logMAR BCVA. However, CRT, parafoveal full retinal thickness, and parafoveal outer retinal thickness were not associated with BCVA. Similar results were obtained from the multiple linear regression model (Model 2) after controlling for age, sex, pseudophakic, axial length, and SSI. In Model 3, only age [coefficient 0.005, 95% confidence interval (CI) 0.003–0.007, p < 0.001] and GCC defect extended beyond the parafoveal area (coefficient 0.079, 95% CI 0.021–0.138, p = 0.008), were significant factors associated with logMAR BCVA, but not parafoveal inner retinal thickness and presence of pRNFL defect. The correlation between logMAR BCVA and different retinal neural parameters are also illustrated in Fig. 4.

Illustrations of the association between logarithm of the minimum angle of resolution best-corrected visual acuity (logMAR BCVA) and different retinal neural parameters among the 120 eyes. A Scatterplot of peripapillary retinal nerve fiber layer (pRNFL) thickness. B Scatterplot of ganglion cell complex (GCC) thickness. C Scatterplot of GCC global loss volume (GLV). D Scatterplot of GCC focal loss volume (FLV). E 2-D plot of pRNFL defects. F 2-D plot of GCC defects
In subgroup analysis, GCC defects extending beyond the parafoveal area was present in 32/96 phakic eyes and 8/24 pseudophakic eyes, and the factor showed an association with worse logMAR BCVA in both subgroups (p = 0.006 and p = 0.009, respectively) (Fig. 5).

Logarithm of the minimum angle of resolution best-corrected visual acuity (LogMAR BCVA) between eyes with and without ganglion cell complex (GCC) defects extending beyond the parafoveal area in phakic and pseudophakic subgroups. The p values were calculated by independent sample t tests. Error bars the standard error in each category
Discussion
Our study has demonstrated that decreased GCC thickness over the central macula is common among patients with CKD. Overall, 283/447 (63%) eyes had parafoveal or perifoveal GCC defects. Among them, 70/283 (25%) eyes presented prominent GCC defects extending beyond the parafoveal area (Fig. 2). We found that only Group 3, but not Group 2, showed worse BCVA than Group 1. Age and GCC defects extending beyond the parafoveal area were independently connected with BCVA in the backward stepwise regression. CRT, parafoveal full retinal thickness, and parafoveal outer retinal thickness were not associated with BCVA.
Human retina contains approximately 1.5 million RGCs responsible for signal transduction to the brain in the visual process, and about 50% of RGCs are located within 4.5 mm of the foveal center [7, 15]. RGC loss is a hallmark of glaucoma [7,8,9,10,11], but can also occur in other ocular diseases, such as DR [16, 17] and pathologic myopia [18]. Reduction of RGCs has also been reported in systemic conditions, such as aging [11], neurodegenerative diseases [19], hypertension [20,21,22], and CKD [4, 6, 23]. Prior studies also found that the severity of RGC loss increased with more advanced stages of CKD [4,5,6, 23].
Visual acuity is one of the most important outcomes in ophthalmic research, and one of the functional outcomes that patients care the most about. Although a good correlation between RGC loss and visual field changes has been demonstrated in both ocular and systemic diseases [7, 24, 25], the influence of RGC loss in BCVA was more controversial. Most structural–functional correlation studies have been conducted for glaucoma [7,8,9,10]. In those studies, central RGCs and central vision were commonly well preserved until late stage [11]. Therefore, the correlation between RGCs related to OCT parameters and visual acuity were usually weak [26]. However, Kobayashi et al. still found a good relationship between BCVA and GCC thickness in open-angle glaucoma when the central papillomacular bundle was involved [27].
There have been limited data that addressed the impact of RGC loss on visual acuity in systemic diseases other than diabetes mellitus [17]. Theoretically, visual acuity decline could be expected if macular RGC loss was prominent. For an example, a study in multiple sclerosis found that GCC or GCL + IPL thicknesses was strongly correlated with BCVA and visual disability [25]. Our data also supported that the loss of GCC over central macula was common and might associate with visual acuity decline in CKD. All quantitative parameters derived from GCC, including GCC thickness, GCC GLV, and GCC FLV, were significantly associated with BCVA in linear regression.
Our study suggested that visual acuity could be well preserved in patients in early stages of GCC loss, and may start to decline after GCC loss over the central macula becomes prominent in patients with CKD. This observation is consistent with prior studies that showed that a time lag could exist between structural change and functional deterioration in early glaucoma [8, 9]. Approximately 25–35% loss of RGCs may have occurred before significant defects appeared on visual field exam [10]. Kim et al. plotted logMAR BCVA against GCC thickness in 186 patients with open-angle glaucoma, and noticed that a second-order polynomial model fit better than the linear model [28], which shows that functional loss might occur after structural damage accumulates past a certain threshold.
Although both the quantitative and qualitative parameters derived from GCC were significantly associated with BCVA, we used qualitative parameters in the backward stepwise regression to facilitate clinical application. Currently, most OCT machines are capable of reliably measuring RGC-related parameters, such as macular RNFL, GCL + IPL, and GCC, over macula [7, 11]. Qualitative parameters, i.e., whether the loss of RGCs or GCC was confined to or had extended beyond the parafovea, could be easily and rapidly determined by different OCT machines.
In clinical practice, macular thinning can be frequently observed in patients with CKD [4,5,6], but these patients may have a wide range of BCVA. Our study found a significant association between logMAR BCVA and parafoveal inner retinal thickness, but logMAR BCVA was not associated with CRT or parafoveal full retinal thickness. This implies that macular thinning, if determined by full retinal thickness, might have a low discriminative power in predicting visual acuity decline in patients with CKD.
pRNFL-derived parameters were significantly associated with BCVA. However, pRNFL defects were not significant in the backward stepwise regression when the GCC-derived parameter occurred simultaneously. Both pRNFL and GCC were biomarkers for retinal neurodegeneration, but GCC parameters reflect the RGC loss over the macula, while pRNFL reflects the RGC loss over both the macula and the peripheral retina [29, 30]. A study on low-tension glaucoma revealed that new paracentral field defects were more likely to be associated with macular GCL + IPL progression than with pRNFL progression [31]. This supports the argument that GCC loss over the macula may play a more important role in central visual function decline.
Only one eye from each patient was used for analysis in this study. We identified 172 patients with both eyes eligible for our study. However, further analysis showed that 73% (Table S1 in Supplementary Materials) and 88% (Table S2 in Supplementary Materials) of patients had concordant GCC defect and pRNFL defect classifications in both eyes, respectively. The retinal neural parameters were also correlated between the two eyes (Table S3 in Supplementary Materials). One possible reason may be that both eyes could be similarly affected by the same systemic conditions. Delicate matching and comparison among the three groups highlighted the influence of GCC defects in this study. Since it could be a concern that large numbers of eyes were abandoned during matching and eye selection, a sensitivity analysis has been performed using generalized estimating equation models that include all eligible eyes in Groups 1–3 (i.e., 413 eyes). The results were similar to those in Table 2, except that parafoveal inner retinal thickness became insignificant (Table S4 in Supplementary Materials). The results of this sensitivity analysis were compatible with the main findings of this study.
Patients with CKD had a higher risk of cataract and were more likely to require cataract surgery [2, 3]. The subgroup analysis in this study showed a trend of worse BCVA in eyes with GCC defects extending beyond the parafoveal area in both phakic and pseudophakic subgroups. Therefore, before cataract surgery, the extensiveness of GCC defects may provide useful information for the prediction of surgical outcomes, and for the selection of appropriate intraocular lens for patients with CKD. Pseudophakic patients had worse visual acuity than phakic patients (Fig. 5), because they were older (mean age 68.5 ± 5.8 and 61.6 ± 10.7, respectively). However, this would not interfere with our main findings because age was well-matched among the groups with different GCC defects.
The mechanism of retinal neurodegeneration in CKD is yet to be determined. Possible pathogenesis may involve comorbid systemic diseases, such as diabetes mellitus and hypertension, and CKD-related pathways, such as increased neurotoxin, oxidative stress, and chronic inflammation [32, 33]. Eyes with DR were not included in this study because DR is associated with macular edema or macular ischemia risk. Eyes with DR may have different pathogenesis in visual loss [17, 34]. Our cohort had a high proportion (84%) of patients with hypertension, which was similar to other CKD studies [1, 35]. The individual effect of hypertension and CKD was difficult to examine in most studies because these two diseases are highly associated with each other [1, 35]. In our cohort, the findings from the high proportion of hypertensive patients may not only facilitate our results’ application to the real-world but also could potentially be extrapolated to hypertensive population complicated with CKD.
The limitations of this study are addressed as follows. First, visual field and microperimetry exams may detect central visual function deterioration in earlier stages, but were not performed in our study. Second, the case number was small in each group. Further large-scale studies are required to confirm our findings. Third, our findings are not applicable to patients with ocular diseases, such as glaucoma, macular pucker, retinal vessel occlusion, and DR, due to their impact on GCC measurement. Fourth, the fluid status in dialysis patients could affect ocular parameters, but was not available in this study. However, our study was strengthened by its delicate matching between groups, with age, sex, axial length, lens status, and cataract grading being well balanced in each group. Therefore, the between-group differences were more likely attributed to these factors under investigation.
Conclusions
Our study demonstrates that macular thinning measured by CRT or parafoveal full retinal thickness may have a low discriminative power in determining BCVA. However, parafoveal inner retinal thickness, pRNFL-derived parameters, and GCC-derived parameters were associated with BCVA in patients with CKD. GCC defects extending beyond the parafoveal area were associated with worse BVCA in both phakic and pseudophakic eyes.
References
Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl. 2011;2022(12):7–11.
Nusinovici S, Sabanayagam C, Teo BW, Tan GSW, Wong TY. Vision impairment in CKD patients: epidemiology, mechanisms, differential diagnoses, and prevention. Am J Kidney Dis. 2019;73:846–57.
Zhu Z, Liao H, Wang W, Scheetz J, Zhang J, He M. Visual impairment and major eye diseases in chronic kidney disease: the national health and nutrition examination survey, 2005–2008. Am J Ophthalmol. 2020;213:24–33.
Wu IW, Sun CC, Lee CC, et al. Retinal neurovascular changes in chronic kidney disease. Acta Ophthalmol. 2020;98:e848–55.
Jung S, Bosch A, Ott C, et al. Retinal neurodegeneration in patients with end-stage renal disease assessed by spectral-domain optical coherence tomography. Sci Rep. 2020;10:5255.
Prakasam RK, Gotze A, von Keyserlingk S, et al. Spectral-domain optical coherence tomography for determination of retinal thickness in pediatric patients with mild-to-moderate chronic kidney disease: a cross-sectional study. Curr Eye Res. 2019;44:206–11.
Scuderi G, Fragiotta S, Scuderi L, Iodice CM, Perdicchi A. Ganglion cell complex analysis in glaucoma patients: What can it tell us? Eye Brain. 2020;12:33–44.
Zhang X, Loewen N, Tan O, et al. Predicting development of glaucomatous visual field conversion using baseline fourier-domain optical coherence tomography. Am J Ophthalmol. 2016;163:29–37.
Medeiros FA, Lisboa R, Weinreb RN, Liebmann JM, Girkin C, Zangwill LM. Retinal ganglion cell count estimates associated with early development of visual field defects in glaucoma. Ophthalmology. 2013;120:736–44.
Kerrigan-Baumrind LA, Quigley HA, Pease ME, Kerrigan DF, Mitchell RS. Number of ganglion cells in glaucoma eyes compared with threshold visual field tests in the same persons. Invest Ophthalmol Vis Sci. 2000;41:741–8.
Mohammadzadeh V, Fatehi N, Yarmohammadi A, et al. Macular imaging with optical coherence tomography in glaucoma. Surv Ophthalmol. 2020;65:597–638.
Yeung L, Wu IW, Sun CC, et al. Early retinal microvascular abnormalities in patients with chronic kidney disease. Microcirculation. 2019;26: e12555.
Stevens PE, Levin A, Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group M. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158:825–30.
Chylack LT Jr, Wolfe JK, Singer DM, et al. The lens opacities classification system III. The longitudinal study of cataract study group. Arch Ophthalmol. 1993;111:831–6.
Smith CA, Chauhan BC. Imaging retinal ganglion cells: enabling experimental technology for clinical application. Prog Retin Eye Res. 2015;44:1–14.
Gong X, Wang W, Li W, et al. Association between renal function and retinal neurodegeneration in chinese patients with type 2 diabetes mellitus. Ann Transl Med. 2021;9:560.
Kim K, Kim ES, Yu SY. Longitudinal relationship between retinal diabetic neurodegeneration and progression of diabetic retinopathy in patients with type 2 diabetes. Am J Ophthalmol. 2018;196:165–72.
Salehi MA, Nowroozi A, Gouravani M, Mohammadi S, Arevalo JF. Associations of refractive errors and retinal changes measured by optical coherence tomography: a systematic review and meta-analysis. Surv Ophthalmol. 2022;67:591–607.
Satue M, Obis J, Rodrigo MJ, et al. Optical coherence tomography as a biomarker for diagnosis, progression, and prognosis of neurodegenerative diseases. J Ophthalmol. 2016;2016:8503859.
Lee SH, Lee WH, Lim HB, Jo YJ, Kim JY. Thicknesses of central macular, retinal nerve fiber, and ganglion cell inner plexiform layers in patients with hypertension. Retina. 2019;39:1810–8.
Lim HB, Lee MW, Park JH, Kim K, Jo YJ, Kim JY. Changes in ganglion cell-inner plexiform layer thickness and retinal microvasculature in hypertension: an optical coherence tomography angiography study. Am J Ophthalmol. 2019;199:167–76.
Akay F, Gundogan FC, Yolcu U, Toyran S, Tunc E, Uzun S. Retinal structural changes in systemic arterial hypertension: an oct study. Eur J Ophthalmol. 2016;26:436–41.
Chow JY, She PF, Pee XK, Wan Muda WN, Catherine Bastion ML. Comparison of peripapillary retinal nerve fiber layer and macular thickness in non-diabetic chronic kidney disease and controls. PLoS ONE. 2022;17: e0266607.
Mohammadzadeh V, Rabiolo A, Fu Q, et al. Longitudinal macular structure-function relationships in glaucoma. Ophthalmology. 2020;127:888–900.
Walter SD, Ishikawa H, Galetta KM, et al. Ganglion cell loss in relation to visual disability in multiple sclerosis. Ophthalmology. 2012;119:1250–7.
Bambo MP, Güerri N, Ferrandez B, et al. Evaluation of the macular ganglion cell-inner plexiform layer and the circumpapillary retinal nerve fiber layer in early to severe stages of glaucoma: correlation with central visual function and visual field indexes. Ophthalmic Res. 2017;57:216–23.
Kobayashi W, Kunikata H, Omodaka K, et al. Correlation of papillomacular nerve fiber bundle thickness with central visual function in open-angle glaucoma. J Ophthalmol. 2015;2015: 460918.
Kim JH, Lee HS, Kim NR, Seong GJ, Kim CY. Relationship between visual acuity and retinal structures measured by spectral domain optical coherence tomography in patients with open-angle glaucoma. Invest Ophthalmol Vis Sci. 2014;55:4801–11.
Cull GA, Reynaud J, Wang L, Cioffi GA, Burgoyne CF, Fortune B. Relationship between orbital optic nerve axon counts and retinal nerve fiber layer thickness measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53:7766–73.
Fortune B, Hardin C, Reynaud J, et al. Comparing optic nerve head rim width, rim area, and peripapillary retinal nerve fiber layer thickness to axon count in experimental glaucoma. Invest Ophthalmol Vis Sci. 2016;57:OCT404-12.
Marshall HN, Andrew NH, Hassall M, et al. Macular ganglion cell-inner plexiform layer loss precedes peripapillary retinal nerve fiber layer loss in glaucoma with lower intraocular pressure. Ophthalmology. 2019;126:1119–30.
Wong CW, Wong TY, Cheng CY, Sabanayagam C. Kidney and eye diseases: Common risk factors, etiological mechanisms, and pathways. Kidney Int. 2014;85:1290–302.
Amdur RL, Feldman HI, Dominic EA, et al. Use of measures of inflammation and kidney function for prediction of atherosclerotic vascular disease events and death in patients with ckd: findings from the cric study. Am J Kidney Dis. 2019;73:344–53.
Byeon SH, Chu YK, Lee H, Lee SY, Kwon OW. Foveal ganglion cell layer damage in ischemic diabetic maculopathy: correlation of optical coherence tomographic and anatomic changes. Ophthalmology. 2009;116:1949-59.e8.
Kalantar-Zadeh K, Jafar TH, Nitsch D, Neuen BL, Perkovic V. Chronic kidney disease. Lancet. 2021;398:786–802.
Acknowledgements
The authors thank Bio-Statistical Consultation Center of Chang Gung Memorial Hospital, Keelung, for the support with statistical analysis. We thank the participants of the study.
Funding
This study is supported by grants from the Ministry of Science and Technology of Taiwan (MOST 109-2314-B-182A-025-). The journal’s Rapid Service Fee was covered by the Chang Gung Memorial Hospital. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author Contributions
Chi-Chin Sun was responsible for review protocol, collecting data, interpreting results, and writing the report. I-Wen Wu was responsible for review protocol, collecting data, interpreting results, and writing the report. Chin-Chan Lee was responsible for review protocol, collecting data, and provided feedback on the report. Chun-Fu Liu was responsible for collecting data, interpreting results, and provided feedback on the report. Yu-Tze Lin was responsible for screening potentially eligible subjects, collecting data, and creating figures. Ling Yeung was responsible for designing the study, review protocol, analyzing data, interpreting results, creating tables and writing the report.
Disclosures
Chi-Chin Sun, I-Wen Wu, Chin-Chan Lee, Chun-Fu Liu, Yu-Tze Lin, and Ling Yeung have nothing to disclose.
Compliance with Ethics Guidelines
This study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments. The original two studies were approved by the Chang Gung Memorial Hospital Institutional Review Board (IRB Nos: 201602022B0 and 201702074A3, respectively) and an informed consent has been provided by each participant. A separate approval (IRB No.: 202200738B0) has been obtained from the same Institutional Review Board for this post hoc analysis and the inform consent requirement was waived for this study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sun, CC., Wu, IW., Lee, CC. et al. Retinal Neurodegeneration and Visual Acuity Decline in Patients with Chronic Kidney Disease. Ophthalmol Ther 12, 909–923 (2023). https://doi.org/10.1007/s40123-022-00635-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00635-3