
Abstract
Introduction
Gonorrhea, caused by Neisseria gonorrhoeae (NG), is the second most common bacterial sexually transmitted infection (STI). Rates of antimicrobial resistance to standard care are increasing worldwide, with many antibiotic classes now ineffective against NG. Gepotidacin is a first-in-class, bactericidal, triazaacenaphthylene antibiotic that inhibits bacterial DNA replication by inhibition of two enzymes, where a single target-specific mutation does not significantly impact susceptibility. Gepotidacin confers activity against NG, including most strains resistant to marketed antibiotics. Here, we describe the design of a phase 3 clinical trial (EAGLE-1; NCT04010539) evaluating gepotidacin for the treatment of uncomplicated urogenital gonorrhea.
Methods
This phase 3, randomized, multicenter, sponsor-blinded, noninferiority study across six countries is comparing the efficacy of gepotidacin with ceftriaxone plus azithromycin in 400 patients with uncomplicated urogenital gonorrhea (microbiological intent-to-treat population) and assessing the safety of gepotidacin in approximately 600 patients (intent-to-treat population). Eligible participants 12 years of age or older with clinical suspicion of urogenital gonococcal infection and a NG-positive urogenital sample and/or purulent discharge are randomized 1:1 to receive oral gepotidacin (2 × 3000 mg 10–12 h apart) or ceftriaxone (500 mg, intramuscular) plus azithromycin (1 g, oral). The primary endpoint is culture-confirmed bacterial eradication of NG from the urogenital site at the test-of-cure (days 4–8) visit.
Planned Outcomes
This trial was designed in accordance with US Food and Drug Administration (2015) and European Medicines Agency (2011) guidance, particularly the primary endpoint and microbiological evaluability requirements. This study will help characterize the risk–benefit profile of gepotidacin for treating uncomplicated urogenital gonorrhea. Gepotidacin is an important potential treatment for gonorrhea to help address the urgent unmet need of multidrug resistance and the increasingly limited number of oral treatment options.
Trial Registration
ClinicalTrials.gov identifier, NCT04010539.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Antimicrobial resistance rates of Neisseria gonorrhoeae are increasing worldwide. |
There is an urgent unmet need for new oral treatment options for patients with uncomplicated urogenital gonorrhea. |
We describe the design of a phase 3 clinical trial to evaluate gepotidacin for the treatment of uncomplicated urogenital gonorrhea in adolescent and adult female and male participants. |
This study will evaluate the risk–benefit profile of gepotidacin as a novel oral treatment option for uncomplicated urogenital gonorrhea. |
Introduction
Gonorrhea, caused by the Gram-negative bacterium Neisseria gonorrhoeae (NG), is a common sexually transmissible infection (STI). Unless treated early, gonorrhea can lead to reproductive tract complications such as pelvic inflammatory disease, ectopic pregnancy, and infertility, and can also facilitate the transmission and acquisition of human immunodeficiency virus [1, 2]. Gonorrhea is the second most common bacterial STI, and the rate of infection is rising rapidly worldwide. In the USA, the Centers for Disease Control and Prevention (CDC) reported that rates of gonorrhea infection in 2018 had increased by 82.6% since a historic low in 2009 [3]. The World Health Organization (WHO) estimated that 82.4 million people were newly infected with NG in 2020 [4]. Between 2013 and 2019, diagnoses of gonorrhea in England rose by 128% to 70,922, the largest annual number ever reported [5]. The increase in international travel in the recent years may be contributing to the spread of gonorrhea [6].
Gonorrhea is curable when treated with antibiotics. However, antimicrobial resistance (AMR) of NG has increased recently, rendering many classes of antibiotics, including fluoroquinolones and oral cephalosporins, ineffective against drug-resistant strains [7]. NG is now classed as a multidrug-resistant pathogen [4, 8,9,10].
NG that is resistant to previously recommended treatment options is rising [11]. In 2019, the CDC estimated that more than 550,000 infections caused by antibiotic-resistant NG occur in the USA each year, and they have identified drug-resistant NG as an urgent threat to public health, with an increase of 124% each year in the number of infections caused by drug-resistant NG [12]. Global surveillance of NG by the WHO in 2017–2018, which included data from 73 countries, showed widespread AMR [13]. Specifically, ciprofloxacin resistance was extremely high (present in all reporting countries), resistance to azithromycin was reported in 84% of countries and rapidly increasing, and resistance to ceftriaxone and cefixime was emerging (in 31% and 47% of countries, respectively) [4, 13, 14]. Over time, resistance to the above first-line therapies, and other historical treatments (e.g., fluoroquinolones, macrolides such as azithromycin, and β-lactams such as penicillin and tetracycline) has increased, and now the CDC recommends 500 mg intramuscular ceftriaxone as the sole effective treatment for gonorrhea [12, 15]. However, as shown by the WHO surveillance study and more recent data, there is an increasing chance that resistance to this drug may be encountered in clinical practice [16, 17]. The possibility of using older antibiotics to treat patients with NG that is resistant to ceftriaxone has been raised but co-resistances are common in such strains [10]. It is of concern that dual-antimicrobial regimens (e.g., mainly ceftriaxone and azithromycin) might not be effective in the long term or an affordable solution in resource-limited systems; hence, this treatment recommendation has been removed from some national guidelines [11, 18]. The WHO has warned that, without new treatments, some gonorrhea infections could become untreatable due to the high levels of AMR [13, 16, 19].
Gepotidacin is a first-in-class, bactericidal, triazaacenaphthylene antibiotic that inhibits bacterial DNA replication by inhibition of two enzymes, where a single target-specific mutation does not significantly impact susceptibility [20,21,22]. The activity of gepotidacin appears specific to bacterial topoisomerases, by interacting with the GyrA subunit of bacterial DNA gyrase and the ParC subunit of bacterial topoisomerase IV in Escherichia coli, with in vitro studies showing little effect on human topoisomerase IIα [20, 21]. The mechanism of action of gepotidacin differs from other novel antibiotics including zoliflodacin, a spiropyrimidinetrione antimicrobial that blocks DNA gyrase (GyrB) [23].
Here, we describe the rationale and design for an ongoing randomized, comparator-controlled, sponsor-blinded, phase 3 clinical trial [Efficacy of Antibacterial Gepotidacin Evaluated (EAGLE)-1; NCT04010539] of gepotidacin versus intravenous (IV) ceftriaxone plus oral azithromycin as control for the treatment of uncomplicated urogenital infection caused by NG in adolescent and adult female and male participants.
Gepotidacin
Preclinical Studies
In vitro studies demonstrated that gepotidacin confers activity against most strains of target pathogens, such as Escherichia coli, Staphylococcus saprophyticus, and NG, including those resistant to established antimicrobial classes [24,25,26].
Clinical Studies
Gepotidacin has been evaluated in phase 2 studies for the treatment of acute bacterial skin and skin structure infections (IV administration) [27], uncomplicated urogenital gonorrhea (oral administration) [28], and uncomplicated urinary tract infection (uUTI; oral administration) [29]. A phase 3 study to evaluate oral gepotidacin for the treatment of uncomplicated urogenital gonorrhea (NCT04010539) is currently ongoing, while one phase 3 trial of oral gepotidacin for uUTI is ongoing (NCT05630833) and two have recently been completed (NCT04020341 and NCT04187144) [30].
Dose Justification
In the current study, gepotidacin will be administered as 2 × 3000 mg oral doses, with the two doses administered 10–12 h apart. The safety and tolerability of oral gepotidacin have been evaluated in phase 1 (healthy volunteers) studies and a phase 2 (patients with uncomplicated urogenital gonorrhea) study [28, 30]. In the phase 2 study, single oral doses of 1500 and 3000 mg gepotidacin were both ≥ 95% efficacious (bacterial eradication) against urogenital NG, with no unexpected safety signals at either dose. However, three participants failed therapy at the urogenital body site [all with a baseline NG isolate with a gepotidacin minimum inhibitory concentration (MIC) of 1 µg/mL and a pre-existing D86N substitution in the parC gene] and resistance to gepotidacin emerged in two isolates during this study, indicating the need for a higher dose in the phase 3 study. Bacterial eradication was 100% when the ratio of the area under the unbound plasma concentration–time curve over 24 h (fAUC0–24) to the MIC was ≥ 48, and all microbiological failures were associated with fAUC0–24/MIC values of ≤ 24 [28, 31, 32]. Due to the limited number of isolates from the phase 2 study with the pre-existing single-step mutation (D86N in parC), an in vitro hollow fiber infection model was developed to determine the level of gepotidacin exposure needed to prevent the development of resistance in NG. Results showed that total daily doses of ≥ 4500 mg would be sufficient [32, 33]. Compared with 1 × 3000 mg dose used in the phase 2 study, administration of 2 × 3000 mg oral doses was expected to provide twofold higher systemic exposures, thereby increasing efficacy against NG isolates with higher gepotidacin MIC values and reducing the risk of developing on-therapy resistance [32]. In addition, the available clinical data and population pharmacokinetics modeling suggested that the proposed phase 3 dose would have a similar safety profile to that of a single 3000 mg dose [34].
Safety
To date, oral and/or IV gepotidacin has been investigated in 18 completed clinical studies [27,28,29,30, 34,35,36,37,38,39], while two phase 3 studies are ongoing: one a study in uUTI in Japan (NCT05630833) and the other the study described herein in urogenital gonorrhea. Adverse events (AEs) in the published studies were generally nonserious and mild to moderate in intensity. Gastrointestinal (GI) effects, including nausea, diarrhea, abdominal pain, and flatulence, were the most common AEs reported (data on file). In a study assessing 2 × 3000 mg doses of gepotidacin 12 h apart in healthy adult and 6 h apart in healthy adolescent volunteers, 77% of participants experienced an AE, 62% experienced diarrhea, and 31% had abdominal discomfort [34]. The GI effects of gepotidacin appear dose related, with reduced incidence at 1500 mg compared with 3000 mg daily doses. The occurrence of GI-related AEs may also be reduced by taking gepotidacin with food [34, 40].
Oral doses of gepotidacin up to 1500 mg twice daily have been associated with only one drug-related serious AE (SAE; dysarthria) [27, 39]. Mild concentration-dependent QT (QTc) prolongation has been observed with gepotidacin, but has not translated into medically significant changes or AEs [28, 29, 37]. Gepotidacin has been shown in vitro to be a rapidly reversible inhibitor of acetylcholinesterase within the clinical plasma concentration range [32, 37]. The selection of gepotidacin doses with geometric mean peak concentration (Cmax) < 14 μg/mL, per the dose selected for EAGLE-1, is expected to minimize the likelihood of QT prolongation and acetylcholinesterase inhibition. Overall, non-GI AEs of gepotidacin have mostly been mild, and associated with Cmax levels higher than those that typically occur with the proposed phase 3 dosing.
Efficacy
The efficacy of gepotidacin was evaluated in a phase 2, randomized, multicenter, open-label, dose-ranging study in adults with uncomplicated urogenital gonorrhea caused by NG [28, 31, 32]. Participants were stratified by gender and sexual orientation and randomly assigned to receive a single oral dose of gepotidacin, either 1500 mg or 3000 mg. Both doses were successful, with urogenital NG eradication rates of 29/30 (97%) and 37/39 (95%) for the 1500 mg and 3000 mg gepotidacin doses, respectively. Three participants failed therapy and two developed resistance to gepotidacin, as described earlier.
Methods
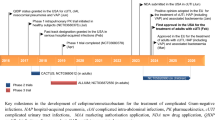
EAGLE-1 is a phase 3, open-label (sponsor-blinded), parallel-group, multicenter, comparator-controlled, noninferiority study in adolescent and adult participants (Fig. 1), with study sites in Australia, Germany, Mexico, Spain, the UK, and the USA. The study aims to compare the efficacy and safety of oral gepotidacin with intramuscular ceftriaxone plus oral azithromycin for the treatment of uncomplicated urogenital gonorrhea caused by NG. The study design follows the US Food and Drug Administration (FDA) Guidance for Industry for developing drug treatments for uncomplicated gonorrhea [41] and the European Medicines Agency (EMA) Guideline on the Evaluation of Medicinal Products indicated for treatment of bacterial infections [42], with a noninferiority margin of −10%.

Study design. aRefer to inclusion criteria (Supplementary Material) for details regarding urogenital gonococcal infection eligibility requirements. bStratification will be performed before randomization to ensure that treatment groups are balanced with regard to sex and sexual orientation combination and age. cStudy treatment will be administered under open-label conditions. All doses of oral study treatment should always be taken after food consumption and with water. dParticipants randomly assigned to gepotidacin will self-administer their second dose (3000 mg) as an outpatient 10–12 h after the first dose; however, for participants who weigh < 50 kg or have moderate renal impairment, the second dose should be taken approximately 12 h after the first dose. eParticipants will return to the study site any time from days 14 to 21 for a follow-up visit. The investigator and/or study site staff should make every effort to ensure a participant returns for this visit. If it is determined that a participant is unable to return to the study site, the follow-up visit assessments may be completed via telephone, with the exception of assessments requiring sample collection for laboratory testing
Study Populations
Participants must be ≥ 12 years of age at the time of signing the informed consent/assent and have a body weight > 45 kg. Eligible participants must have a clinical suspicion of a urogenital gonococcal infection (which can include sexual contact within the past 14 days with a partner who had a confirmed gonococcal infection) with or without pharyngeal and/or rectal gonococcal infection. Also required is one of the following: (1) purulent yellow, green, or white urethral discharge (male participants) or abnormal cervical or vaginal mucopurulent discharge upon physical examination (female participants); (2) a positive culture for NG up to 5 days before screening (as long as the participant has not received any treatment for this infection); (3) a Gram (or equivalent) stain (urogenital specimen) positive for intracellular Gram-negative diplococci up to 5 days before screening (as long as the participant has not received any treatment for this infection); or (4) a prior positive nucleic acid amplification test (NAAT) assay for NG up to 7 days before screening (as long as the participant has not received any treatment for this infection). All participants must be willing to either abstain from anal, oral, and vaginal sexual intercourse or use condoms for all forms of sexual intercourse from the baseline visit through to the test-of-cure visit. Participants are excluded if they have specific renal, urogenital, cardiac, or hepatic medical conditions; are immunocompromised; require medication that may be impacted by inhibition of acetylcholinesterase; have a body mass index ≥ 40 kg/m2 or ≥ 35.0 kg/m2 with obesity-related health conditions; have any condition that may interfere with the absorption, distribution, metabolism, or excretion of gepotidacin; have received treatment with other systemic antibiotics or antifungals within 1 week before study entry; were previously enrolled in a gepotidacin study; or are pregnant. For further details of the exclusion criteria, please see the Supplementary Material.
Participants are stratified by sex and sexual orientation: men who have sex with men or are bisexual; men who have sex with women; and women. Stratification by age (12–17 years; ≥ 18–65 years; > 65 years) is also being implemented.
Study Procedures
The schedule of activities is depicted in Table 1. At baseline (study day 1), participants are randomly assigned to receive gepotidacin or ceftriaxone plus azithromycin. The first dose of gepotidacin (3000 mg) is administered orally at the study site during the baseline visit, and the second dose (also 3000 mg, oral) is taken in an outpatient setting 10–12 h later. For participants who weigh < 50 kg or have moderate renal impairment [defined as creatinine clearance of ≥ 30–59 mL/min (per renal artery pressure)], the second dose will be taken approximately 12 h after the first dose. Ceftriaxone (1 × intramuscular 500 mg dose) plus azithromycin (1 × oral 1 g dose) are administered at the study site during the baseline visit.
Safety and microbiological assessments will be conducted at the baseline visit, test-of-cure visit (days 4–8) and follow-up visit (days 14–21) as outlined in the schedule of activities. Per FDA guidance, microbiological success is defined as culture-confirmed eradication of NG at the respective body site observed at the test-of-cure visit (days 4–8).
Participants whose baseline NAAT results are positive for Chlamydia trachomatis (CT) and/or Mycoplasma genitalium (MG) infection are treated for these conditions according to local standard of care at or after the test-of-cure visit (once all the study procedures of this visit have been completed). At study entry, any participant suspected or confirmed to have a CT infection will not be allowed to enroll in the study if, per the investigator’s judgment, standard-of-care treatment for this infection cannot be safely postponed until the test-of-cure visit.
Measurements—Samples for Microbiological Analysis
At the baseline visit, a pretreatment urogenital swab specimen will be obtained from all participants for Gram stain and bacteriological culture for NG for local laboratory culture with subsequent confirmation of identification at the central laboratory. In addition, urine or swab samples will be collected for central laboratory and local laboratory NAATs for NG and CT as well as MG (central laboratory only). Baseline pretreatment pharyngeal and rectal swab specimens will also be obtained from participants consenting to these samples being taken, for NG bacteriological local laboratory culture and central laboratory NG and CT NAATs. At the test-of-cure visit, specimens from all body sites collected at baseline will be collected with the exception of the MG NAAT. Gram stain will only be conducted on urogenital specimens. At the follow-up visit, pharyngeal specimens will be obtained for NG local laboratory bacteriological culture and central laboratory NAAT testing only if participants had a positive central laboratory NAAT assay for pharyngeal NG at both the baseline and test-of-cure visits. If patients are positive for MG by NAAT at the baseline visit from the urogenital site, a urogenital specimen will be collected at the follow-up visit for MG central laboratory NAAT testing. NAAT outcomes are exploratory endpoints and do not form the primary or secondary endpoints. Local laboratories are utilized for NG bacterial culturing to ensure that the culture is conducted within 24 h of specimen collection from the patient; NG is fastidious, and viability may be compromised beyond 24 h of specimen collection. All of the NG isolates recovered at the local laboratory will be frozen and shipped to a central laboratory for confirmation of identification, susceptibility testing, and molecular analysis.
Planned Outcomes
The primary efficacy endpoint for this study is culture-confirmed bacterial eradication of NG from the urogenital body site (i.e., microbiological success) at the test-of-cure visit. Secondary efficacy endpoints include culture-confirmed bacterial eradication of NG from the rectal and/or pharyngeal body sites (i.e., microbiological success) at the test-of-cure visit. Details of safety endpoints, including NAAT testing, can be found in the Supplementary Material.
Adverse Events
All reported AEs and SAEs are coded using Medical Dictionary for Regulatory Activities and summarized by system organ class and preferred terms. The severity of each AE is determined by the investigator according to the US National Institute of Allergy and Infectious Diseases Division of Microbiology and Infectious Diseases criteria for adult toxicity assessment [43]. Predefined AEs of special interest for this study are cardiovascular events, GI events, Clostridioides difficile events, and AEs potentially related to acetylcholinesterase inhibition.
Data Analysis
This study is designed to demonstrate noninferiority of gepotidacin to ceftriaxone plus azithromycin dual therapy for the primary efficacy endpoint. Gepotidacin will be declared noninferior to treatment with ceftriaxone plus azithromycin if the lower limit of the two-sided 95% confidence interval (CI) for the difference between the microbiological success rate of gepotidacin and ceftriaxone plus azithromycin at the test-of-cure visit is above the noninferiority limit of −10.0% [44]. Superiority of gepotidacin will be declared if the lower end of the CI is above 0%. The Miettinen and Nurminen [45] method will be used for the primary analysis, stratified by sex and sexual orientation (men who have sex with men, men who have sex with women, or females). The intent-to-treat (ITT) population is defined as all participants randomly assigned to study treatment. The primary analysis will be conducted on the microbiological-ITT (micro-ITT) population, which includes all participants in the ITT population who receive at least one dose of study treatment and have confirmed NG isolated that is ceftriaxone-susceptible from baseline culture of their urogenital specimen.
Approximately 620 participants will be randomized to achieve approximately 400 participants (200 per treatment group) in the micro-ITT population.
Assuming a 90% microbiological success rate for both treatment groups, a sample size of 400 micro-ITT participants will provide approximately 91% power to demonstrate noninferiority of gepotidacin to ceftriaxone plus azithromycin with a 0.025 one-sided significance level and a −10% noninferiority margin.
Strengths and Limitations
Given its unique mechanism of action, gepotidacin may represent an important step towards effective oral treatment for patients with urogenital gonorrhea infections caused by AMR NG [26]. The study described here (EAGLE-1) will help characterize the risk–benefit profile of gepotidacin in the treatment of uncomplicated urogenital gonorrhea. The primary endpoint of the study is culture-confirmed bacterial eradication of NG at the test-of-cure visit, which is consistent with previous studies in uncomplicated gonorrhea and with FDA and regulatory guidance [41, 42]. Results of NAATs were included as exploratory endpoints as they are the standard of care in clinical practice and would be supportive of the culture results [15]. However, this study was not designed to analyze efficacy on the basis of NAATs as nucleic acids can remain viable up to 15 days post clearance of the infection [46].
The EAGLE-1 study commenced in October 2019 and continued during the COVID-19 pandemic. This placed additional challenges on data collection and study processes. Some of these challenges were mitigated by protocol amendments. Every effort was made to adhere to protocol-specified procedures, including follow-up assessments. However, there was a need to minimize the amount of time patients spent in the clinic. Hence, where local regulations permitted, electronic consent and remote collection of study-related data were utilized. In addition, additional study questions on sexual history/behavior may have deterred some potential participants from enrolling in the study.
The comparator antibiotics (ceftriaxone and azithromycin) were standard of care in many countries at the time the study began enrolling. However, treatment practices have since been updated. For example, azithromycin is no longer recommended in the UK or the USA due to increased resistance rates [42, 47]. Treatment with ceftriaxone and azithromycin is still recommended in Australia, Spain, Germany, and Mexico, where there are also EAGLE-1 sites, although these countries recommend different doses. It was decided to continue with 500 mg ceftriaxone and 1 g azithromycin as the comparator regimen throughout this study.
In EAGLE-1, gepotidacin is administered as a total dose of 6000 mg, split into two doses of 3000 mg, 10–12 h apart. Compared with the current standard of care for urogenital gonorrhea of intramuscular ceftriaxone plus azithromycin, gepotidacin may be more suitable for patients with a needle phobia, who prefer oral administration, or who have an allergy to cephalosporins, while an orally administered treatment option will aid in reducing patient waiting time in the healthcare facility (time needed to wait for a nurse to administer injection, and post-injection wait), as well as clinician workload.
Ethics
These studies are conducted in accordance with the protocols and consensus ethical principles derived from international guidelines including the Declaration of Helsinki and Council for International Organizations of Medical Sciences International Ethical Guidelines, International Council on Harmonization Good Clinical Practice Guidelines, and applicable laws and regulations. Protocol and amendments, informed consent form/adolescent assent form/eConsent (if applicable), investigator’s brochure, and other relevant documents (e.g., advertisements) were submitted to an institutional review board/independent ethics committee (IRB/IEC) by the investigator and reviewed and approved by the IRB/IEC before the study was initiated. The master IRB was Advarra Institutional Review Board (Columbia, MD, USA), while study sites outside the USA used their appropriate local IRB/IEC. Adolescent patients will only be enrolled at study sites where investigators have experience in this population and if allowed per the study site’s institutional ethics committees and local country/national regulatory guidelines; enrollment will be contingent upon such approvals.
Dissemination
AMR is an increasing challenge among patients with gonorrhea, with NG becoming resistant to nearly all currently available antibiotics recommended in guidelines for treatment. The phase 3 trial presented here will advance our understanding of the potential for using the novel antibiotic gepotidacin to treat uncomplicated urogenital gonorrhea. With its unique mechanism of action, gepotidacin may help address the urgent future unmet need for new and effective oral treatment options for urogenital gonorrhea infections caused by AMR NG.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
St Cyr S, Barbee L, Workowski KA, Bachmann LH, Pham C, Schlanger K, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1911–6. https://doi.org/10.15585/mmwr.mm6950a6.
Kirkcaldy RD, Weston E, Segurado AC, Hughes G. Epidemiology of gonorrhoea: a global perspective. Sex Health. 2019;16:401–11. https://doi.org/10.1071/SH19061.
Centers for Disease Control and Prevention. Sexually transmitted disease surveillance. Available at: https://www.cdc.gov/std/stats18/STDSurveillance2018-full-report.pdf. Accessed May 2023.
World Health Organization. Gonorrhoea: latest antimicrobial global surveillance results and guidance for vaccine development published. Available at: https://www.who.int/news/item/22-11-2021-gonorrhoea-antimicrobial-resistance-results-and-guidance-vaccine-development. Accessed May 2023.
Merrick R, Cole M, Pitt R, Enayat Q, Ivanov Z, Day M, et al. Antimicrobial-resistant gonorrhoea: the national public health response, England, 2013 to 2020. Euro Surveill. 2022;27:2200057. https://doi.org/10.2807/1560-7917.ES.2022.27.40.2200057.
Vicente-de-la-Cruz MLM, Giesen C, Díaz-Menéndez M. International travels and transmission of multidrug resistant Neisseria gonorrhoeae in Europe: a systematic review. Travel Med Infect Dis. 2022;49:102401. https://doi.org/10.1016/j.tmaid.2022.102401.
World Health Organization. Multi-drug resistant gonorrhoea. Available at: https://www.who.int/news-room/fact-sheets/detail/multi-drug-resistant-gonorrhoea. Accessed May 2023.
Yang F, Liu J, Gu Y, Jiao R, Yan J, Gao S, et al. Antimicrobial activity of auranofin, cannabidivarin, and tolfenamic acid against multidrug-resistant Neisseria gonorrhoeae. Microbiol Spectr. 2022;10:e0395222. https://doi.org/10.1128/spectrum.03952-22.
Green LR, Cole J, Parga EFD, Shaw JG. Neisseria gonorrhoeae physiology and pathogenesis. Adv Microb Physiol. 2022;80:35–83. https://doi.org/10.1016/bs.ampbs.2022.01.002.
Fifer H, Livermore DM, Uthayakumaran T, Woodford N, Cole MJ. What’s left in the cupboard? Older antimicrobials for treating gonorrhoea. J Antimicrob Chemother. 2021;76:1215–20. https://doi.org/10.1093/jac/dkaa559.
Bodie M, Gale-Rowe M, Alexandre S, Auguste U, Tomas K, Martin I. Addressing the rising rates of gonorrhea and drug-resistant gonorrhea: There is no time like the present. Can Commun Dis Rep. 2019;45:54–62. https://doi.org/10.14745/ccdr.v45i23a02.
Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2019. Available at: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf. Accessed May 2023.
Unemo M, Lahra MM, Escher M, Eremin S, Cole MJ, Galarza P, et al. WHO global antimicrobial resistance surveillance for Neisseria gonorrhoeae 2017–18: a retrospective observational study. Lancet Microbe. 2021;2:e627–36. https://doi.org/10.1016/S2666-5247(21)00171-3.
Ewers EC, Curtin JM, Ganesan A. Challenges in managing gonorrhea and new advances in prevention. Infect Dis Clin North Am. 2023;37:223–43. https://doi.org/10.1016/j.idc.2023.02.004.
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70:1–187. https://doi.org/10.15585/mmwr.rr7004a1.
Day M, Pitt R, Mody N, Saunders J, Rai R, Nori A, et al. Detection of 10 cases of ceftriaxone-resistant Neisseria gonorrhoeae in the United Kingdom, December 2021 to June 2022. Euro Surveill. 2022;27:2200803. https://doi.org/10.2807/1560-7917.Es.2022.27.46.2200803.
Yan J, Chen Y, Yang F, Ling X, Jiang S, Zhao F, et al. High percentage of the ceftriaxone-resistant Neisseria gonorrhoeae FC428 clone among isolates from a single hospital in Hangzhou, China. J Antimicrob Chemother. 2021;76:936–9. https://doi.org/10.1093/jac/dkaa526.
Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clin Microbiol Rev. 2014;27:587–613. https://doi.org/10.1128/cmr.00010-14.
Yuan Q, Shi S, Dai Y, Jiang M, Jiang P, Xu D, et al. Surveillance of the antimicrobial susceptibility and molecular characteristics of Neisseria gonorrhoeae isolates collected in Changsha China from 2016 to 2021. Jpn J Infect Dis. 2022. https://doi.org/10.7883/yoken.JJID.2022.532.
Gibson EG, Bax B, Chan PF, Osheroff N. Mechanistic and structural basis for the actions of the antibacterial gepotidacin against Staphylococcus aureus gyrase. ACS Infect Dis. 2019;5:570–81. https://doi.org/10.1021/acsinfecdis.8b00315.
Bax BD, Chan PF, Eggleston DS, Fosberry A, Gentry DR, Gorrec F, et al. Type IIA topoisomerase inhibition by a new class of antibacterial agents. Nature. 2010;466:935–40. https://doi.org/10.1038/nature09197.
Oviatt A, Huang J, Ingraham K, Chan PF, Osheroff N. Biochemical and genetic evidence that gepotidacin demonstrates well-balanced dual targeting against DNA gyrase and topoisomerase IV in Escherichia coli. ECCMID 2022; 2022 23–26 April; Lisbon, Portugal.
Morgan H, Lipka-Lloyd M, Warren AJ, Hughes N, Holmes J, Burton NP, et al. A 2.8 Å structure of Zoliflodacin in a DNA cleavage complex with Staphylococcus aureus DNA gyrase. Int J Mol Sci. 2023;24:1634. https://doi.org/10.3390/ijms24021634.
Biedenbach DJ, Bouchillon SK, Hackel M, Miller LA, Scangarella-Oman NE, Jakielaszek C, et al. In vitro activity of gepotidacin, a novel triazaacenaphthylene bacterial topoisomerase inhibitor, against a broad spectrum of bacterial pathogens. Antimicrob Agents Chemother. 2016;60:1918–23. https://doi.org/10.1128/aac.02820-15.
Mushtaq S, Vickers A, Sadouki Z, Cole M, Fifer H, DaNascimento V, et al. In vitro activities of gepotidacin, a novel triazaacenaphthylene topoisomerase IV and DNA gyrase inhibitor, against Gram-negative bacteria and Staphylococcus saprophyticus. ECCMID 2019; 2019; Amsterdam, The Netherlands.
Jacobsson S, Golparian D, Scangarella-Oman N, Unemo M. In vitro activity of the novel triazaacenaphthylene gepotidacin (GSK2140944) against MDR Neisseria gonorrhoeae. J Antimicrob Chemother. 2018;73:2072–7. https://doi.org/10.1093/jac/dky162.
O’Riordan W, Tiffany C, Scangarella-Oman N, Perry C, Hossain M, Ashton T, et al. Efficacy, safety, and tolerability of gepotidacin (GSK2140944) in the treatment of patients with suspected or confirmed Gram-positive acute bacterial skin and skin structure infections. Antimicrob Agents Chemother. 2017;61:e02095-16. https://doi.org/10.1128/aac.02095-16.
Taylor SN, Morris DH, Avery AK, Workowski KA, Batteiger BE, Tiffany CA, et al. Gepotidacin for the treatment of uncomplicated urogenital gonorrhea: a phase 2, randomized, dose-ranging, single-oral dose evaluation. Clin Infect Dis. 2018;67:504–12. https://doi.org/10.1093/cid/ciy145.
Overcash JS, Tiffany CA, Scangarella-Oman NE, Perry CR, Tao Y, Hossain M, et al. Phase 2a pharmacokinetic, safety, and exploratory efficacy evaluation of oral gepotidacin (GSK2140944) in female participants with uncomplicated urinary tract infection (acute uncomplicated cystitis). Antimicrob Agents Chemother. 2020;64:e00199-e220. https://doi.org/10.1128/aac.00199-20.
Perry C, Hossain M, Powell M, Raychaudhuri A, Scangarella-Oman N, Tiffany C, et al. Design of two phase III, randomized, multicenter studies comparing gepotidacin with nitrofurantoin for the treatment of uncomplicated urinary tract infection in female participants. Infect Dis Ther. 2022;11:2297–310. https://doi.org/10.1007/s40121-022-00706-9.
Scangarella-Oman NE, Hossain M, Dixon PB, Ingraham K, Min S, Tiffany CA, et al. Microbiological analysis from a phase 2 randomized study in adults evaluating single oral doses of gepotidacin in the treatment of uncomplicated urogenital gonorrhea caused by Neisseria gonorrhoeae. Antimicrob Agents Chemother. 2018;62:e01221-18. https://doi.org/10.1128/AAC.01221-18.
Scangarella-Oman NE, Hossain M, Perry CR, Tiffany C, Powell M, Swift B, et al. Dose selection for a phase III study evaluating gepotidacin (GSK2140944) in the treatment of uncomplicated urogenital gonorrhoea. Sex Transm Infect. 2022;99:64–9. https://doi.org/10.1136/sextrans-2022-055518.
VanScoy BD, Scangarella-Oman NE, Fikes S, Min S, Huang J, Ingraham K, et al. Relationship between gepotidacin exposure and prevention of on-therapy resistance amplification in a Neisseria gonorrhoeae hollow-fiber in vitro infection model. Antimicrobial Agents Chemother. 2020;64:e00521–20. https://doi.org/10.1128/AAC.00521-20.
Barth A, Hossain M, Brimhall DB, Perry CR, Tiffany CA, Xu S, et al. Pharmacokinetics of oral formulations of gepotidacin (GSK2140944), a triazaacenaphthylene bacterial type II topoisomerase inhibitor, in healthy adult and adolescent participants. Antimicrob Agents Chemother. 2022;66:e0126321. https://doi.org/10.1128/AAC.01263-21.
Hossain M, Tiffany C, Tao Y, Barth A, Marbury TC, Preston RA, et al. Pharmacokinetics of gepotidacin in subjects with normal hepatic function and hepatic impairment. Clin Pharmacol Drug Dev. 2021;10:588–97. https://doi.org/10.1002/cpdd.913.
Hossain M, Tiffany C, Raychaudhuri A, Nguyen D, Tai G, Alcorn H Jr, et al. Pharmacokinetics of gepotidacin in renal impairment. Clin Pharmacol Drug Dev. 2020;9:560–72. https://doi.org/10.1002/cpdd.807.
Hossain M, Zhou M, Tiffany C, Dumont E, Darpo B. A phase I, randomized, double-blinded, placebo- and moxifloxacin-controlled, four-period crossover study to evaluate the effect of gepotidacin on cardiac conduction as assessed by 12-lead electrocardiogram in healthy volunteers. Antimicrob Agents Chemother. 2017;61:e02385–16. https://doi.org/10.1128/AAC.02385-16.
Negash K, Andonian C, Felgate C, Chen C, Goljer I, Squillaci B, et al. The metabolism and disposition of GSK2140944 in healthy human subjects. Xenobiotica. 2016;46:683–702. https://doi.org/10.3109/00498254.2015.1112933.
Wagenlehner F, Perry CR, Hooton TM, Scangarella-Oman NE, Millns H, Feng H, et al. Efficacy and safety of oral gepotidacin in the treatment of uncomplicated urinary tract infection: results of two randomised, multicentre phase 3 trials (EAGLE-2 and EAGLE-3). ECCMID; 2023; Copenhagen, Denmark.
Tiffany CA, Hossain M, McDonald M, Dumont EF. Effect of food on safety, tolerability and pharmacokinetics in healthy volunteers > 65 years following multiple doses of GSK2140944, a novel bacterial topoisomerase inhibitor. In: 55th Interscience conference of antimicrobial agents and chemotherapy; 2015. September 17–21 San Diego, CA, USA.
Food and Drug Administration. Uncomplicated gonorrhea: developing drugs for treatment. Guidance for industry. 2015. https://www.fda.gov/files/drugs/published/Uncomplicated-Gonorrhea--Developing-Drugs-for-Treatment.pdf.
UK Health Security Agency. Managing incidents of ceftriaxone-resistant Neisseria gonorrhoeae in England. https://www.gov.uk/government/publications/ceftriaxone-resistant-neisseria-gonorrhoeae-incident-management/managing-incidents-of-ceftriaxone-resistant-neisseria-gonorrhoeae-in-england Accessed May 2023.
US Department of Health and Human Services NIoH, National Institute of Allergy and Infectious Diseases, Division of AIDS. Division of AIDS (DAIDS) table for grading the severity of adult and pediatric adverse events, corrected version 2.1. [July 2017]. https://rsc.niaid.nih.gov/sites/default/files/daidsgradingcorrectedv21.pdf. Accessed May 2023.
Food and Drug Administration. Non-inferiority clinical trials to establishing effectiveness. https://www.fda.gov/media/78504/download. Accessed May 2023.
Base SAS® 9.4 Procedures Guide: Statistical Procedures, Second Edition. https://support.sas.com/documentation/cdl/en/procstat/66703/PDF/default/procstat.pdf. pp 177–8.
Barbee LA, Soge OO, Khosropour CM, LeClair A, Golden MR. Time to clearance of Neisseria gonorrhoeae RNA at the pharynx following treatment. J Clin Microbiol. 2022;60:e0039922. https://doi.org/10.1128/jcm.00399-22.
Centers for Disease Control and Prevention. Gonorrhea treatment and care. Available at: https://www.cdc.gov/std/gonorrhea/treatment.htm. Accessed May 2023.
Medical Writing, Editorial, and Other Assistance
Medical writing support, under the guidance of the authors, was provided by Natasha Tracey, PhD, and Alexia Tsakaneli, PhD, of Ashfield MedComms, an Inizio company, and was funded by GSK. The authors would like to thank Pharmaceutical Product Development (PPD), part of Thermo Fisher Scientific, for its role in running the clinical trials.
Funding
This study, including study design, data collection, analysis, and interpretation, and medical writing and submission support for the manuscript, was funded by GSK (study 116577; NCT04010539), who also paid the Rapid Service Fee. Studies were also supported in whole or in part with federal funds from the Office of the Assistant Secretary for Preparedness and Response, Biomedical Advanced Research and Development Authority (HHSO100201300011C).
Author information
Authors and Affiliations
Contributions
All authors had access to the study data, take responsibility for the accuracy of the analysis, contributed to data interpretation, reviewed, and contributed to the content of the manuscript, and had authority in the decision to submit the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Caroline R. Perry, Nicole E. Scangarella-Oman, Helen Millns, William Flight, Sally Gatsi, Charles Jakielaszek, and Salim Janmohamed are employees of, and shareholders in, GSK. David A. Lewis is employed by Western Sydney Local Health District and has no disclosures to declare.
Ethical Approval
These studies are conducted in accordance with the protocols and consensus ethical principles derived from international guidelines including the Declaration of Helsinki and Council for International Organizations of Medical Sciences International Ethical Guidelines, International Council on Harmonization Good Clinical Practice Guidelines, and applicable laws and regulations. Protocol and amendments, informed consent form/adolescent assent form/eConsent (if applicable), investigator’s brochure, and other relevant documents (e.g., advertisements) were submitted to an institutional review board/independent ethics committee (IRB/IEC) by the investigator and reviewed and approved by the IRB/IEC before the study was initiated. The master IRB was Advarra Institutional Review Board (Columbia, MD, USA), while study sites outside the USA used their appropriate local IRB/IEC. Adolescent patients will only be enrolled at study sites where investigators have experience in this population and if allowed per the study site’s institutional ethics committees and local country/national regulatory guidelines; enrollment will be contingent upon such approvals.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Perry, C.R., Scangarella-Oman, N.E., Millns, H. et al. Efficacy and Safety of Gepotidacin as Treatment of Uncomplicated Urogenital Gonorrhea (EAGLE-1): Design of a Randomized, Comparator-Controlled, Phase 3 Study. Infect Dis Ther 12, 2307–2320 (2023). https://doi.org/10.1007/s40121-023-00862-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-023-00862-6