
Abstract
Introduction
Highly active antiretroviral therapy (HAART) is effective and well tolerated, but hepatotoxicity is relatively common. Different non-invasive methods are available for detecting liver fibrosis in patients with chronic liver disease.
Methods
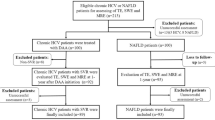
Patients who were HIV positive and who had given their informed consent were included in this cross-sectional study. Transient elastography [FibroScan® (FS); Echosens], serum hyaluronic acid (HA), Hepascore (HS), Fibrosis-4 (FIB-4), and aspartate aminotransferase to platelet ratio index (APRI) were used to detect liver fibrosis in the patients. The agreement between FS and the other methods was evaluated. To observe the hepatotoxicity of HAART, patients with chronic viral hepatitis B or C were excluded by detection of hepatitis B surface antigens and hepatitis C virus antibodies. Patients with chronic alcohol intake were excluded by measuring carbohydrate-deficient transferrin (CDT). FS correlation with the duration of therapy with protease inhibitors (PI), nucleoside reverse transcriptase inhibitors (NRTI), and non-nucleoside reverse transcriptase inhibitors (NNRTI) was evaluated.
Results
Overall, 203 patients were included in the study. The agreement between the different tests ranged from 64% to 77%: FS vs. HA, 72%; FS vs. APRI, 74%; FS vs. HS, 77%; and FS vs. FIB-4, 64%. After excluding patients with chronic hepatitis B or C and elevated CDT, 153 patients remained for studying the hepatotoxicity of HAART. A significant correlation of FS with the duration of medication intake was observed for PIs (P = 0.026; r = 0.18). NRTI and NNRTI therapy duration did not correlate with FS.
Conclusions
The agreement between FS and other tests ranged from 64% to 77%. A significant correlation was found between liver stiffness and the duration of therapy with PIs, which underlines the known hepatotoxicity of this substance group.
Funding
Heinz-Ansmann Foundation.
Similar content being viewed by others


Introduction
Highly active antiretroviral therapy (HAART) has dramatically changed the course of HIV infection, with a decrease in morbidity and mortality derived from classical opportunistic infections [1–3]. Abnormal liver function tests are common and may be caused by HIV itself, hepatitis viruses, systemic opportunistic infections, malignancies, and drug-induced hepatotoxicity [4–7]. There are four major classes of HAART: nucleoside reverse transcriptase inhibitors (NRTI), non-nucleoside reverse transcriptase inhibitors (NNRTI), protease inhibitors (PI), and integrase inhibitors.
Hepatotoxicity, liver enzyme elevation, and drug interactions are significant problems in patients with HIV who are on HAART [8, 9]. In patients commencing antiretroviral therapy, 14–20% will experience elevations of liver enzymes and 2–10% will require interruption of antiretroviral therapy due to severe hepatic injury and a marked elevation of liver enzymes [10, 11]. There are multiple pathogenetic mechanisms involved in hepatotoxicity, including direct drug toxicity, immune reconstitution in the presence of hepatitis C virus (HCV) and/or hepatitis B virus (HBV) co-infections, hypersensitivity reactions with liver involvement, and mitochondrial toxicity [12]. Other pathogenetic pathways may be involved, such as insulin resistance caused by several antiretrovirals, which may contribute to the development of steatohepatitis. The relationship between drug toxicity and the development of liver fibrosis or liver cirrhosis is still unclear.
Different non-invasive methods have been described to detect liver fibrosis or liver cirrhosis. Most of these scores use serum markers [13]. In the past few years, transient elastography [FibroScan® (FS); Echosens] has gained an important role in the detection of liver fibrosis. FS is a simple, non-invasive method of assessing liver fibrosis by measuring liver stiffness [14]. A good correlation has been found between the stage of liver fibrosis and the measured liver stiffness [15–17].
In this study, the authors compared different non-invasive methods of detecting liver fibrosis/cirrhosis in patients who were HIV positive. Furthermore, to identify the drug classes that are associated with liver damage the duration of medication intake was correlated with the results of FS.
Methods
Patients
Patients who were HIV positive and who had given their informed consent were included into this cross-sectional study performed at the University of Düsseldorf, Germany. Diagnosis of HIV infection was confirmed by detection of HIV antibodies by western blot. The clinical stage of HIV infection was classified according to the revised Centers for Disease Control and Prevention (CDC) staging system. The study protocol was approved by the ethics committee of the University of Düsseldorf.
Liver Stiffness Measured by FS
Details of the technical background and examination procedure have been described previously [14]. Patients had been fasting for at least 8 h when FS was performed. Blood tests were taken just before performance of FS. The tip of the probe transducer was placed on the skin between the rib bones and the level of the right lobe of the liver. The measurement depth was between 25 and 65 mm below the skin surface. Ten measurements were performed with success rates of at least 60% and the interquartile range did not exceed 30% of the median value. The results were expressed in kiloPascal (kPa). The median value was taken as representative. A good correlation has been established with Metavir scores as follows: F0–F1, <7.1 kPa; F2–F3, 7.1–12.5 kPa; and F4, >12.5 kPa [16].
Aspartate Aminotransferase to Platelet Ratio Index
The aspartate aminotransferase (AST) to platelet ratio index (APRI) was calculated using the formula APRI = AST level/(upper limit of normal [ULN]) × 100/platelet count (109/L) and categorized according to cutoffs defined by Wai et al. [18]: <0.5, no significant fibrosis; 0.5–1.5 fibrosis; <1.5, cirrhosis).
Hyaluronic Acid
Hyaluronic acid (HA) levels (ng/ml) were assessed in serum samples, stored at −80 °C, using a commercially available enzyme-linked immunosorbent assay (Corgenix, Broomfield, CO, USA). The following previously published [19] HA cutoff values were used: <75 ng/ml, no significant fibrosis; 75–110 ng/ml, fibrosis; >110 ng/ml, cirrhosis.
Hepascore
The Hepascore (HS) was calculated from the following equation: y/(1 + y); where y = exp[−4.185818 − (0.0249 × age) + (0.7464 × sex) + (1.0039 × α2-macroglobulin) + (0.0302 × HA) + (0.0691 × bilirubin) − (0.0012 × gamma-glutamyl transpeptidase (GGT)]; with age in years, male sex = 1, female sex = 0, α2-macroglobulin in g/L, HA in μg/L, bilirubin in μmol/L, and GGT in U/L [20]. The following HS cutoff values were used: <0.5, no fibrosis; 0.5–0.85, fibrosis; >0.85, cirrhosis.
Carbohydrate-Deficient Transferrin
Carbohydrate-Deficient Transferrin (CDT) was taken as a marker for increased alcohol intake. CDT performed best as an alcohol biomarker in comparison with other biomarkers, with a sensitivity of 67% and specificity of 71% for detecting an average consumption of more than 40 g per day versus less [21].
Fibrosis-4
The Fibrosis-4 (FIB-4) values were calculated automatically using the formula: age (years) × AST [U/L]/(platelets [109/L] × (ALT [U/L])1/2), in which the age of the patient was the age at the time of measurement liver stiffness. The following FIB-4 cutoff values were used: <1.45, no fibrosis; 1.45–3.25, fibrosis; >3.25, cirrhosis [22].
Body Mass Index
Body mass index (BMI) was calculated using the following equation: weight (kg)/[height (m)]2.
Serological Testing of HBV and HCV
The qualitative analysis of HCV-RNA was tested by a commercial polymerase chain reaction assay (Amplicor HCV Amplification 2.0, Roche Diagnostics, Indianapolis, IN, USA). The quantitative analysis of HCV-RNA was made by a commercial assay (HCV-TaqMan (in-house); limit of detection 250 U/ml). Hepatitis B surface antigen (HBs-Ag) as a serologic marker of HBV infection was detected by a commercial immunoassay (Axsym HBs-Ag, Abbott Laboratories, North Chicago, IL, USA).
Statistical Analysis
Data were entered in SPSS (version 11.0, SPSS Inc., Munich, Germany). A χ 2 or Fisher’s exact test (F test) was used for the comparison of categorical variables, and a Mann–Whitney test was used for the comparison of continuous variables. The correlation study between therapy duration and liver stiffness was done by Pearson’s test; patients with signs of hepatitis or cholestasis were not included in this analysis. To compare the agreement between the different tests of fibrosis/cirrhosis, a kappa statistic was performed. A logistic regression was performed to identify independent factor that was associated with the increase of liver stiffness. The significance level was set at 0.05 and all P values were two tailed.
Results
A total of 203 (148 men and 55 women, mean age 47 ± 11 years) consecutive patients who were HIV positive were enrolled in the study. Patients’ characteristics are shown in Table 1. Fifty-one patients were at HIV stage CDC A, 69 patients were at stage CDC B, and 83 patients were at stage CDC C.
FS was successfully performed (at least 60% success rate) in 188 (93%) of the 203 patients. The following frequencies of fibrosis grades were observed: no significant fibrosis (FS <7.1 kPa), 160 (85%) patients; fibrosis (FS 7.1–12.5 kPa), 25 (13%) patients; and cirrhosis (FS >12.5 kPa), 3 (2%) patients (Table 2).
APRI was available for 180 patients. APRI values indicating the grade of fibrosis showed the following results: no significant fibrosis (APRI <0.5), 128 (71%) patients; fibrosis (APRI 0.5–1.5), 47 (26%) patients; and cirrhosis (APRI >1.5), 5 (3%) patients.
Serum samples for detection of HA were available for 184 patients. The following grade of fibrosis/cirrhosis was associated with the measured HA levels: no significant fibrosis (HA <75 ng/ml), 143 (77%) patients; fibrosis (HA 75–110 ng/ml), 18 (10%) patients; and cirrhosis (HA >110 ng/ml), 23 (13%) patients.
All parameters for calculation of the HS were available for 147 patients. HS showed the following frequencies: no significant fibrosis (HS <0.5), 119 (81%) patients; fibrosis (HS 0.5–0.85), 13 (9%) patients; and cirrhosis (HS >0.85), 15 (10%) patients.
FIB-4 was available for 187 patients. FIB-4 values indicating the grade of fibrosis showed the following results: no significant fibrosis (FIB-4 <1.45), 116 (62%) patients; fibrosis (FIB-4 1.45–3.25), 61 (33%) patients; and cirrhosis (FIB-4 >3.25), 10 (5%) patients.
To study agreement between FS and the other tests, a kappa statistical procedure was performed. A total of 184 patients underwent liver stiffness measurement and HA was detected concomitantly. The stage of fibrosis agreed in 132 (72%) patients (κ = 0.2). A consistent result was found in 133 (74%) of the 180 patients who underwent both FS and APRI (κ = 0.33). A similar percentage was observed by the comparison between FS and HS. Both methods of fibrosis/cirrhosis detection were performed in 147 patients. The same stage of fibrosis/cirrhosis was detected in 113 (77%) of these patients (κ = 0.35). A total of 180 patients underwent liver stiffness measurement and FIB-4 was detected concomitantly. The stage of fibrosis agreed in 115 (64%) patients (κ = 0.19).
To investigate the influence of HAART on the liver stiffness, the liver stiffness was correlated with the duration (months) of medication for each substance group (NRTI, NNRT, and PI). Based on the fact that only four patients received integrase inhibitors, this substance group was not correlated with FS. All patients with any positive marker for HBV (HBs-Ag positive, n = 11) or HCV (hepatitis C virus antibody positive, n = 16; HCV-RNA positive, n = 8) infection were excluded. CDT was taken as a marker for increased alcohol intake. Patients with a CDT above the ULN (2.5%) were also excluded. A total of 153 patients remained for the analysis. Liver stiffness was below 7.1 kPa in 134 (87.7%) patients, was between 7.1 and 12.5 kPa in 18 (11.7%) patients, and was above 12.5 kPa in one patient (0.6%). Statistical analyses were only done between patients with a liver stiffness below 7.1 kPa and patients with a liver stiffness between 7.1 and 12.5 kPa (Table 3).
Therapy duration with each substance group was correlated with the measured liver stiffness. Therapy duration with PI ranged from 0 to 124 months (mean 28 ± 31 months). Liver stiffness showed a positive, statistically significant correlation with the duration of PI intake (r = 0.18; P = 0.026; Table 4). Therapy duration of NRTI (mean 55 ± 44 months; range 0–188 months; r = 0.044; P = 0.59) and NNRTI (mean 24 ± 28 months; range 0–105 months; r = −0.6; P = 0.461) did not correlate with liver stiffness. No significant correlation could be observed between liver stiffness and age (P = 0.25), sex (P = 0.12), race (P = 0.13 for white patients vs. black patients), or BMI (P = 0.22), so these factors could be excluded as being confounding. To identify therapy duration with PI as an independent factor for the increase of liver stiffness, a logistic regression was performed including the factors BMI, age, sex, race, and therapy duration with PI. Therapy duration was the only factor that was significantly associated with liver stiffness [P = 0.049; 95% confidence interval (CI) 0.056–0.964].
Discussion
HAART has dramatically changed the course of HIV infection, and has decreased the morbidity and mortality derived from classical opportunistic infections [23]. Therapy is effective in most cases and well tolerated in a substantial proportion of patients, but adverse events, such as hypersensitivity reactions and hepatotoxicity, are relatively common [24, 25]. Therapy with PIs is more often associated with liver enzyme elevation than with NRTIs or NNRTIs. Long-term effects of HAART in developing liver fibrosis/cirrhosis have not been sufficiently studied. This may in part be explained by the fact that liver biopsy is the gold standard for the detection of liver fibrosis/cirrhosis, but is an invasive method with associated complications [26]. Furthermore, to study the development of liver fibrosis under HAART, repeated liver biopsies are difficult to justify due to the associated risk and discomfort. Different non-invasive methods are available to detect liver fibrosis/cirrhosis. Being aware that these tests were predominantly evaluated in patients with hepatitis C or alcoholic liver disease, these easy-to-handle tests were used to detect HAART-associated liver fibrosis. Moreover, the agreement between different non-invasive methods (FS, HS, HA, and APRI) were compared. FS is not reliable in patients who are not fasting, with acute hepatitis, or cholestasis [27–29]. Taking this into account, only patients who were fasting and had no sign of acute hepatitis or cholestasis were included in the current study.
A total of 203 patients were included in this cross-sectional analysis. In the first step, the extent of agreement between the different tests was compared. Based on the fact that FS has been evaluated in liver diseases of different origin, FS was chosen as the reference. The comparison between the methods showed a comparable stage of fibrosis in 64% to 77% of patients. This comparison between these methods is limited by the fact that HS, HA, FIB-4, and APRI are not designed to assess fatty liver disease. An excellent correlation has been shown for non-alcoholic fatty liver disease and FS [30].
To study the role of the different substance groups (PI, NRTI, and NNRTI) in developing liver fibrosis/cirrhosis, FS was correlated with the duration of medication intake for each group. Because of the limited number of patients who received integrase inhibitors, the effect of this substrate group could not be studied. Additional factors, which may lead to liver fibrosis/cirrhosis, were largely eliminated by excluding patients with chronic HBV or HCV infection and patients with evidence of chronic alcohol abuse. A total of 153 patients remained for this analysis. We found a significant correlation of the liver stiffness with the duration of PI intake, but not with the duration of NTRI or NNRTI intake. To exclude age, sex, race, and BMI as confounding factors a multivariable analysis including these factors was performed. All these factors could be excluded as relevant factors for hepatotoxicity.
Hepatotoxicity is a well-recognized side effect of PI therapy with over 50% of patients developing asymptomatic mild elevation of transaminases [31]. In some series, up to 10–20% developed severe hepatotoxicity with liver enzyme elevation above 5 times the ULN [31]. Sulkowski et al. [31] observed severe (liver enzyme elevation above 3 times the ULN) hepatotoxicity in 31 (10.4%) of 298 patients (95% CI 7.2–14.4%) [31]. Transaminases usually rise after 3 months of therapy and will return to normal over the next 3–5 months in most cases; however, approximately 10% remain persistently elevated [32].
The histological pattern observed in patients with PI hepatotoxicity is variable without definite pathognomonic features. Features include bile duct injury and proliferation, hepatocellular necrosis, and Mallory bodies. Ballooning of hepatocytes, Kupffer cell activation, and peri-cellular fibrosis in zone 3 have recently been described as features of PI hepatotoxicity [33–35]. Different mechanisms of hepatotoxicity such as mitochondrial damage, hypersensitivity reactions, and inhibition of several cytochrome P450 isoforms may be involved. The PIs, in particular ritonavir, are potent inhibitors of cytochrome P450 and thus may alter plasma levels of drugs that share the same routes of metabolism [36]. Dose-dependent hepatotoxicity may result from toxic levels of drugs whose clearance is reduced. The results of the current study underline the hepatotoxicity of PIs and the association of long-term drug use with the development of liver fibrosis. This correlation has to be investigated in a longer prospective study. The acceptance of repeated measurements with the non-invasive methods can be improved, so that prospective studies to detect drug induced hepatotoxicity can be performed. The weakness of the current study is that it is a cross-sectional study. All patients underwent FS once, so that possible progression of the liver stiffness could not be detected. Furthermore, possible factors like co-medication intake such as statin or antihypertensive drugs were not considered. Switches to other antiretroviral therapy regimes were also not incorporated.
Hepatotoxicity is a serious complication in patients taking HAART. Here, an agreement of the stage of liver fibrosis/cirrhosis in 64% to 77% using different non-invasive methods was demonstrated. After exclusion of known factors which can trigger liver fibrosis/cirrhosis, a correlation of FS with the duration of PI intake was observed. FS can be used to detect the development of liver fibrosis/cirrhosis in patients taking HAART, particularly in patients receiving a therapy regime that includes PI.
Conclusion
The agreement between FS and the other tests was 64% to 77%. A significant correlation was found for liver stiffness and the duration of therapy with PI, which underlines the known hepatotoxicity of this substance group. Patients receiving PI should be monitored to detect hepatotoxicity and avoid long-term complications such as liver cirrhosis. FS is a simple method of assessing liver fibrosis and can be used in regular clinical routine.
References
Lohse N, Hansen AB, Gerstoft J, Obel N. Improved survival in HIV-infected persons: consequences and perspectives. J Antimicrob Chemother. 2007;60:461–3.
Palella FJ Jr, Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34.
Borrell C, Rodríguez-Sanz M, Pasarín MI, et al. AIDS mortality before and after the introduction of highly active antiretroviral therapy: does it vary with socioeconomic group in a country with a National Health System? Eur J Public Health. 2006;16:601–8.
Boesecke C, Cooper DA. Toxicity of HIV protease inhibitors: clinical considerations. Curr Opin HIV AIDS. 2008;3:653–9.
Cooper CL. HIV antiretroviral medications and hepatotoxicity. Curr Opin HIV AIDS. 2007;2:466–73.
Chihrin S, Antoniou T, Raboud J, et al. Risk factors for grade 3–4 liver enzyme elevation in HIV and hepatitis C coinfected patients on combination antiretroviral therapy. AIDS Patient Care STDS. 2007;21:469–78.
Torti C, Lapadula G, Casari S, et al. Incidence and risk factors for liver enzyme elevation during highly active antiretroviral therapy in HIV-HCV co-infected patients: results from the Italian EPOKA-MASTER Cohort. BMC Infect Dis. 2005;5:58.
Abrescia N, D’Abbraccio M, Figoni M, Busto A, Maddaloni A, De Marco M. Hepatotoxicity of antiretroviral drugs. Curr Pharm Des. 2005;11:3697–710.
Kontorinis N. Dieterich D hepatotoxicity of antiretroviral therapy. AIDS Rev. 2003;5:36–43.
Dore G. Antiretroviral therapy-related hepatotoxicity: predictors and clinical management. J HIV Ther. 2003;8:96–100.
Sulkowski MS. Management of hepatic complications in HIV-infected persons. J Infect Dis. 2008;197:S279–93.
Núñez M. Hepatotoxicity of antiretrovirals: incidence, mechanisms and management. J Hepatol. 2006;44:S132–9.
Gressner AM, Gao CF, Gressner OA. Non-invasive biomarkers for monitoring the fibrogenic process in liver: a short survey. World J Gastroenterol. 2009;15:2433–40.
Sandrin L, Fourquet B, Hasquenoph JM, et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29:1705–13.
Erhardt A, Lorke J, Vogt C, et al. Transient elastography for diagnosing liver cirrhosis [in German]. Dtsch Med Wochenschr. 2006;131:2765–9.
Castera L, Vergniol J, Foucher J, et al. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology. 2005;128:343–50.
Foucher J, Chanteloup E, Vergniol J, et al. Diagnosis of cirrhosis by transient elastography (FibroScan): a prospective study. Gut. 2006;55:403–8.
Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26.
Guéchot J, Serfaty L, Bonnand AM, Chazouillères O, Poupon RE, Poupon R. Prognostic value of serum hyaluronan in patients with compensated HCV cirrhosis. J Hepatol. 2000;32:447–52.
Adams LA, Bulsara M, Rossi E, et al. Hepascore: an accurate validated predictor of liver fibrosis in chronic hepatitis C infection. Clin Chem. 2005;51:1867–73.
McDonald H, Borinskya S, Kiryanov N, Gil A, Helander A, Leon DA. Comparative performance of biomarkers of alcohol consumption in a population sample of working-aged men in Russia: the Izhevsk Family Study. Addiction. 2013;108:1579–89.
Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43:1317–25.
Kim JH, Psevdos G Jr, Gonzalez E, Singh S, Kilayko MC, Sharp V. All-cause mortality in hospitalized HIV-infected patients at an acute tertiary care hospital with a comprehensive outpatient HIV care program in New York City in the era of highly active antiretroviral therapy (HAART). Infection. 2013;41:545–51.
Prosperi MC, Fabbiani M, Fanti I, et al. Predictors of first-line antiretroviral therapy discontinuation due to drug-related adverse events in HIV-infected patients: a retrospective cohort study. BMC Infect Dis. 2012;12:296.
Casado JL. Liver toxicity in HIV-infected patients receiving novel second-generation nonnucleoside reverse transcriptase inhibitors etravirine and rilpivirine. AIDS Rev. 2013;15:139–45.
Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med. 2001;344:495–500.
Mederacke I, Wursthorn K, Kirschner J, et al. Food intake increases liver stiffness in patients with chronic or resolved hepatitis C virus infection. Liver Int. 2009;29:1500–6.
Millonig G, Reimann FM, Friedrich S, et al. Extrahepatic cholestasis increases liver stiffness (FibroScan) irrespective of fibrosis. Hepatology. 2008;48:1718–23.
Sagir A, Erhardt A, Schmitt M, Haussinger D. Transient elastography is unreliable for detection of cirrhosis in patients with acute liver damage. Hepatology. 2008;47:592–5.
Alkhouri N, Sedki E, Alisi A, et al. Combined paediatric NAFLD fibrosis index and transient elastography to predict clinically significant fibrosis in children with fatty liver disease. Liver Int. 2013;33:79–85.
Sulkowski MS, Thomas DL, Chaisson RE, Moore RD. Hepatotoxicity associated with antiretroviral therapy in adults infected with human immunodeficiency virus and the role of hepatitis C or B virus infection. JAMA. 2000;283:74–80.
Wit FW, Weverling GJ, Weel J, Jurriaans S, Lange JM. Incidence of and risk factors for severe hepatotoxicity associated with antiretroviral combination therapy. J Infect Dis. 2002;186:23–31.
Akhtar MA, Mathieson K, Arey B, et al. Hepatic histopathology and clinical characteristics associated with antiretroviral therapy in HIV patients without viral hepatitis. Eur J Gastroenterol Hepatol. 2008;20:1194–204.
Bruno R, Sacchi P, Maiocchi L, Patruno S, Filice G. Hepatotoxicity and antiretroviral therapy with protease inhibitors: a review. Dig Liver Dis. 2006;38:363–73.
Orenstein R, Tsogas N. Looking beyond highly active antiretroviral therapy: drug-related hepatotoxicity in patients with human immunodeficiency virus infection. Pharmacotherapy. 2002;22:1468–78.
Yeh RF, Gaver VE, Patterson KB, et al. Lopinavir/ritonavir induces the hepatic activity of cytochrome P450 enzymes CYP2C9, CYP2C19, and CYP1A2 but inhibits the hepatic and intestinal activity of CYP3A as measured by a phenotyping drug cocktail in healthy volunteers. J Acquir Immune Defic Syndr. 2006;42:52–60.
Acknowledgments
This study was supported by the Heinz-Ansmann Foundation for AIDS research. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval of the version to be published.
Conflict of interest
Abdurrahman Sagir, Birgit Glaubach, Kurtulus Sahin, Dirk Graf, Andreas Erhardt, Mark Oette, and Dieter Häussinger declare no conflict of interest.
Compliance with ethics guidelines
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study. The study complies with current ethical considerations, and was approved by the ethical review committee (University Düsseldorf; study number 2701).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sagir, A., Glaubach, B., Sahin, K. et al. Transient Elastography for the Detection of Liver Damage in Patients with HIV. Infect Dis Ther 4, 355–364 (2015). https://doi.org/10.1007/s40121-015-0073-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-015-0073-y