
Abstract
Purpose
Despite developments in both imaging and microbiological techniques, the final diagnosis of IE often remains challenging. In this single-center cohort study, we aimed to identify the specific indications for request of 18F-FDG-PET/CT in clinical practice and to evaluate the diagnostic benefit of this nuclear imaging technique.
Methods
A total of 235 patients with possible (n = 43) or definite (n = 192) IE according to the revised Duke criteria were prospectively studied from July 2013 until December 2016. Echocardiography was generally used as the primary cardiac imaging technique. All patients were treated by a multidisciplinary Endocarditis Team. Diagnostics with 18F-FDG-PET/CT were undertaken on request by at least one member of the multidisciplinary team when overall diagnostics were inconclusive.
Results
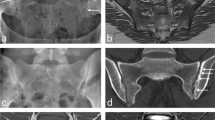
In 20 patients, 18F-FDG-PET/CT scan was performed for additional diagnostic evaluation. Hereof, 15 patients had a history of implanted cardiac prosthetic material. In six patients with definite IE, the use of 18F-FDG-PET/CT was helpful for further clarification of the diagnosis. In one patient with possible IE, the diagnosis could be reclassified to definite IE. In addition, one case of vertebral osteomyelitis as well as upper and lower leg abscesses and knee empyema were detectable as extracardiac foci. Furthermore, 18F-FDG-PET/CT leads to a modification of the management in five patients.
Conclusion
Our findings support the utility of 18F-FDG-PET/CT as an adjunctive diagnostic tool especially in the evaluation of prosthetic valve-/cardiac device-related IE and for the detection of extracardiac foci in some cases. However, due to remaining limitations also of this imaging technique, a multidisciplinary clinical evaluation still remains the essential basis for the diagnostic assessment.


Similar content being viewed by others


References
Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. 2016;387:882–93.
Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000–13: a secular trend, interrupted time-series analysis. Lancet. 2015;385:1219–28.
Cahill TJ, Baddour LM, Habib G, Hoen B, Salaun E, Pettersson GB, Schäfers HJ, Prendergast BD. Challenges in Infective Endocarditis. J Am Coll Cardiol. 2017;69:325–44.
Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Dulgheru R, El Khoury G, Erba PA, Iung B, Miro JM, Mulder BJ, Plonska-Gosciniak E, Price S, Roos-Hesselink J, Snygg-Martin U, Thuny F, Tornos Mas P, Vilacosta I, Zamorano JL, Document Reviewers, Erol Ç, Nihoyannopoulos P, Aboyans V, Agewall S, Athanassopoulos G, Aytekin S, Benzer W, Bueno H, Broekhuizen L, Carerj S, Cosyns B, De Backer J, De Bonis M, Dimopoulos K, Donal E, Drexel H, Flachskampf FA, Hall R, Halvorsen S, Hoen B, Kirchhof P, Lainscak M, Leite-Moreira AF, Lip GY, Mestres CA, Piepoli MF, Punjabi PP, Rapezzi C, Rosenhek R, Siebens K, Tamargo J, Walker DM. 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36:3075–128.
Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, Bashore T, Corey GR. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30:633–38.
Bruun NE, Habib G, Thuny F, Sogaard P. Cardiac imaging in infectious endocarditis. Eur Heart J. 2014;35:624–32.
Roque A, Pizzi MN, Cuéllar-Calàbria H, Aguadé-Bruix S. 18F-FDG-PET/CT angiography for the diagnosis of infective endocarditis. Curr Cardiol Rep. 2017;19:15.
Pizzi MN, Roque A, Fernández-Hidalgo N, Cuéllar-Calabria H, Ferreira-González I, Gonzàlez-Alujas MT, Oristrell G, Gracia-Sánchez L, González JJ, Rodríguez-Palomares J, Galiñanes M, Maisterra-Santos O, Garcia-Dorado D, Castell-Conesa J, Almirante B, Aguadé-Bruix S, Tornos P. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-fluordeoxyglucose positron emission tomography/computed tomography angiography: initial results at an infective endocarditis referral center. Circulation. 2015;132:1113–26.
Baddour LM, Wilson WR, Bayer AS, Fowler VG Jr, Tleyjeh IM, Rybak MJ, Barsic B, Lockhart PB, Gewitz MH, Levison ME, Bolger AF, Steckelberg JM, Baltimore RS, Fink AM, O’Gara P, Taubert KA, American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Stroke Council. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435–86.
Wang A, Gaca JG, Chu VH. Management considerations in infective endocarditis: a review. JAMA. 2018;320:72–83.
Habib G, Derumeaux G, Avierinos JF, Casalta JP, Jamal F, Volot F, Garcia M, Lefevre J, Biou F, Maximovitch-Rodaminoff A, Fournier PE, Ambrosi P, Velut JG, Cribier A, Harle JR, Weiller PJ, Raoult D, Luccioni R. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. J Am Coll Cardiol. 1999;33:2023–29.
Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service Am J Med. 1994;96:200–9.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Fleisher LA, Jneid H, Mack MJ, McLeod CJ, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70:252–89.
Kaura A, Byrne J, Fife A, Deshpande R, Baghai M, Gunning M, Whitaker D, Monaghan M, MacCarthy PA, Wendler O, Dworakowski R. Inception of the ‘endocarditis team’ is associated with improved survival in patients with infective endocarditis who are managed medically: findings from a before-and-after study. Open Heart. 2017;4:e000699. https://doi.org/10.1136/openhrt-2017-000699.
Saby L, Laas O, Habib G, Cammilleri S, Mancini J, Tessonnier L, Casalta JP, Gouriet F, Riberi A, Avierinos JF, Collart F, Mundler O, Raoult D, Thuny F. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol. 2013;61:2374–82.
Ricciardi A, Sordillo P, Ceccarelli L, Maffongelli G, Calisti G, Di Pietro B, Caracciolo CR, Schillaci O, Pellegrino A, Chiariello L, Andreoni M, Sarmati L. 18-Fluoro-2-deoxyglucose positron emission tomography-computed tomography: an additional tool in the diagnosis of prosthetic valve endocarditis. Int J Infect Dis. 2014;28:219–24.
Tlili G, Amraoui S, Mesguich C, Rivière A, Bordachar P, Hindié E, Bordenave L. High performances of (18)F-fluorodeoxyglucose PET-CT in cardiac implantable device infections: a study of 40 patients. J Nucl Cardiol. 2015;22(4):787–98.
Ambrosini V, Zompatori M, Fasano L, Nanni C, Nava S, Rubello D, Fanti S. (18)F-FDG PET/CT for the assessment of disease extension and activity in patients with sarcoidosis: results of a preliminary prospective study. Clin Nucl Med. 2013;38:e171–77.
Wollenweber T, Roentgen P, Schäfer A, Schatka I, Zwadlo C, Brunkhorst T, Berding G, Bauersachs J, Bengel FM. Characterizing the inflammatory tissue response to acute myocardial infarction by clinical multimodality noninvasive imaging. Circ Cardiovasc Imaging. 2014;7:811–18.
Scholtens AM, Verberne HJ, Budde RP, Lam MG. Additional heparin preadministration improves cardiac glucose metabolism suppression over low-carbohydrate diet alone in 18F-FDG PET imaging. J Nucl Med. 2016;57:568–73.
Acknowledgements
C.L. is supported by the German Centre for Infection Research (DZIF) and the Federal Joint Committee (G-BA, German Federal Ministry of Health). J.R. is supported by the German Centre for Infection Research (DZIF) and the German Research Foundation (DFG). G.F. has received research Grants from the German Federal Ministry of Education and Research (BMBF) 01KI1017 and 01KG0915 and is supported by the German Centre for Infection Research (DZIF).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
C.H. reports personal fees from MSD Sharp & Dohme and Pfizer, lecture fees from Actelion and travel grants from Actelion, Bayer, Orion Pharma and MSD Sharp & Dohme. G.M. received lecture fees from Pfizer, Novartis, Servier, ZOLL, Getinge and Orion Pharma. In the past 3 years, N. Jazmati has received payment for lectures from MSD Sharp & Dohme. C.L. has received honoraria for lectures or travel grants from Abbott, ViiV, Gilead, MSD, and Janssen. In the past 2 years, G.F. has received lecture fees from Bristol Myers Squibb, Janssen Cilag, Merck Sharp & Dohme and Pfizer, travel grants from Gilead and Janssen Cilag, research grants from Gilead, Janssen Cilag, Merck Sharp & Dohme and Roche. G.F. served on advisory boards of Janssen Cilag, Merck Sharp & Dohme, Merck Serono, Pfizer, Roche and Shionogi. In the last 3 years, N. Jung has received lecture fees from Labor Stein, Novartis, Gilead, Infectopharm and MSD and travel grants from Gilead, Novartis and Basilea.
Rights and permissions
About this article

Cite this article
Hohmann, C., Michels, G., Schmidt, M. et al. Diagnostic challenges in infective endocarditis: is PET/CT the solution?. Infection 47, 579–587 (2019). https://doi.org/10.1007/s15010-019-01278-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-019-01278-6