
Abstract
Background:
The oxazolidinone antibiotic linezolid has demonstrated efficacy in treating infections caused by methicillin-resistant Staphylococcus aureus (MRSA). In a retrospective analysis of two prospective randomized clinical trials in patients with nosocomial pneumonia (NP), initial therapy with linezolid produced significantly better clinical cure and survival rates than vancomycin in the subset of patients with documented MRSA infection. This study was designed to evaluate the economic impact of these clinical outcomes from the perspective of the German health care system to determine the use of these regimens in the light of limited resources and rising costs.
Methods:
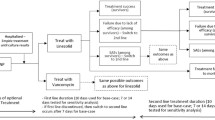
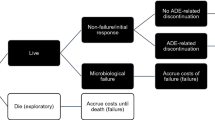
A decision–analytic model using clinical trial data was developed to examine the costs and outcomes of treatment with linezolid or vancomycin in hospitalized patients with NP caused by suspected MRSA. The model followed an average patient from initiation of empiric treatment until treatment success, death, or second-line treatment failure. Local treatment patterns and resource use were obtained from a Delphi panel. Costs were taken from published sources. Outcomes included total cost per patient, cost per additional cure, cost per death avoided, and cost per life-year gained.
Results:
The model calculated that linezolid was associated with an 8.7% higher cure rate compared with vancomycin (73.6% vs 64.9%, respectively). Average total costs per episode for linezolid- and vancomycin-treated patients were €12,829 and €12,409, respectively. Death rates were 13.2% lower with linezolid than with vancomycin (20.7% vs 33.9%), resulting in an average of 2.3 life-years gained per linezolid-treated patient in a 65-year-old cohort (14.0 life-years vs 11.7 life-years). With linezolid, incremental costs per death avoided and per patient cured were €3,171 and €4,813, respectively. The base case estimated a similar mean length of stay for both drugs (11.2 vs 10.8 days). One-way sensitivity analyses did not change the overall results.
Conclusion:
The model estimated a higher clinical cure (+8.7%) and survival (+13.2%) for linezolid compared with vancomycin at an incremental cost of €420 per treatment episode. The cost–benefit profile suggests that linezolid could be considered a cost-effective alternative to vancomycin in the treatment of patients with NP caused by suspected MRSA in Germany.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Richards MJ, Edwards JR, Culver DH, Gaynes RP: Nosocomial infections in combined medical-surgical intensive care units in the United States. Infect Control Hosp Epidemiol 2000; 21: 510–515.
Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Chanoin MH, Wolff M, Spencer RC, Hemmer M: The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA 1995; 274: 639–644.
Gastmeier P, Sohr D, Geffers C, Zuschneid I, Behnke M, Ruden H: Mortality in German intensive care units: dying from or with a nosocomial infection? Anasthesiol Intensivmed Notfallmed Schmerzther 2005; 40: 267–272.
Gastmeier P, Sohr D, Geffers C, Behnke M, Daschner F, Ruden H: Mortality risk factors with nosocomial Staphylococcus aureus infections in intensive care units: results from the German Nosocomial Infection Surveillance System (KISS). Infection 2005; 33: 50–55.
Gastmeier P, Geffers C, Sohr D, Schwab F, Behnke M, Ruden H: Surveillance of nosocomial infections in intensive care units. Current data and interpretations. Wien Klin Wochenschr 2003; 115: 99–103.
Diekema DJ, Pfaller MA, Schmitz FJ, Smayevsky J, Bell J, Jones RN, Beach M and the SENTRY Participants Group: Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997–1999. Clin Infect Dis 2001; 32: s114–s132.
European Antimicrobial Resistance Surveillance System (EARSS) Database: National Institute of Public Health and the Environment. RIVM, Department of Infectious Disease Epidemiology, Bilthoven, The Netherlands; 2005. Available at http://www.earss.rivm.nl/PAGINA/interwebsite/database.html
Gleason TG, Crabtree TD, Pelletier SJ, Raymond DP, Karchmer TB, Pruett TL, Sawyer RG: Prediction of poorer prognosis by infection with antibiotic-resistant gram-positive cocci than by infection with antibiotic-sensitive strains. Arch Surg 1999; 134: 1033–1040.
Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y: Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis 2003; 36: 53–59.
Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y: The impact of methicillin resistance in Staphylococcus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol 2005; 26: 166–174.
Shorr AF, Combes A, Kollef MH, Chastre J: Methicillin-resistant Staphylococcus aureus prolongs intensive care unit stay in ventilator-associated pneumonia, despite initially appropriate antibiotic therapy. Crit Care Med 2006; 34: 700–706.
American Thoracic Society Infectious Diseases Society of America Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 15: 388–416.
Stevens DL: The role of vancomycin in the treatment paradigm. Clin Infect Dis 2006; 42: S51–S57.
Deresinski S: Counterpoint: vancomycin and Staphylococcus aureus—an antibiotic enters obsolescence. Clin Infect Dis 2007; 44: 1543–1548.
Kollef MH, Rello J, Cammarata SK, Croos-Dabrera RV, Wunderink RG: Clinical cure and survival in Gram-positive ventilator-associated pneumonia: retrospective analysis of two double-blind studies comparing linezolid with vancomycin. Intensive Care Med 2004; 30: 388–394.
Wilcox M, Nathwani D, Dryden M: Linezolid compared with teicoplanin for the treatment of suspected or proven Gram-positive infections. J Antimicrob Chemother 2004; 53: 335–344.
Cepeda JA, Whitehouse T, Cooper B, Hails J, Jones K, Kwaku F, Taylor L, Hayman S, Shaw S, Kibbler C, Shulman R, Singer M, Wilson AP: Linezolid versus teicoplanin in the treatment of Gram-positive infections in the critically ill: a randomized, double-blind, multicentre study. J Antimicrob Chemother 2004; 53: 345–355.
Rubinstein E, Cammarata S, Oliphant T, Wunderink R and the Linezolid Nosocomial Pneumonia Study Group: Linezolid (PNU-100766) versus vancomycin in the treatment of hospitalized patients withnosocomial pneumonia: a randomized, double-blind, multicenter study. Clin Infect Dis 2001; 32: 402–412.
Wunderink RG, Cammarata SK, Oliphant TH, Kollef MH, and the Linezolid Nosocomial Pneumonia Study Group: Continuation of a randomized, double-blind, multicenter study of linezolid versus vancomycin in the treatment of patients with nosocomial pneumonia. Clin Ther 2003; 25: 980–992.
Wunderink RG, Rello J, Cammarata SK, Croos-Dabrera RV, Kollef MH: Linezolid vs vancomycin: analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest 2003; 124: 1789–1797.
French G: Linezolid. Int J Clin Pract 2001; 55: 59–63.
Paladino JA, Gudgel LD, Forrest A, Niederman MS: Cost-effectiveness of IV-to-oral switch therapy: azithromycin vs cefuroxime with or without erythromycin for the treatment of community-acquired pneumonia. Chest 2002; 122: 1271–1279.
Vinken AG, Li JZ, Balan DA, Rittenhouse BE, Willke RJ, Goodman C: Comparison of linezolid with oxacillin or vancomycin in the empiric treatment of cellulitis in US hospitals. Am J Ther 2003; 10: 264–274.
Vinken A, Li Z, Balan D, Rittenhouse B, Willkie R, Nathwani D: Economic evaluation of linezolid, flucloxacillin and vancomycin in the empirical treatment of cellulitis in UK hospitals: a decision analytical model. J Hosp Infect 2001; 49: S13–S24.
Zanetti G, Bally F, Greub G, Garbino J, Kinge T, Lew D, Romand JA, Bille J, Aymon D, Stratchounski L, Krawczyk L, Rubinstein E, Schaller MD, Chiolero R, Glauser MP, Cometta A, and the Cefepime Study Group: Cefepime versus imipenem-cilastatin for treatment of nosocomial pneumonia in intensive care unit patients: a multicenter, evaluator-blind, prospective, randomized study. Antimicrob Agents Chemother 2003; 47: 3442–3447.
Rote Liste® Service GmbH. Rote Liste. Available at: http://www.rote-liste.de. Accessed 27 Feb 2007.
Deutsche Krankenhausgesellschaft Tarif der Deutschen Krankenhausgesellschaft für die Abrechnung erbrachter Leistungen und fur die Kostenerstattung vom Artz an das Krankenhaus DKG-NT Band I. W. Kohlhammer Verlag, July 2005.
Einheitlicher Bewertungsmaßstab (EBM). Kassenärztliche Bundesvereinigung Berlin, erstellt am 22.03.2007 (V. 7.0).
Institut für das Entgeltsystem im Krankenhaus gGmbH. Abschlussbericht. Weiterentwicklung des G-DRG-Systems für das Jahr 2004. Klassifikation, Katalog und Bewertungsrelationen. Band II: Fallpauschalen-Katalog, Klinische Profile, Kostenprofile, 19 December 2003. Available at: http://inek.customer.msim.de/service/download/Projektbericht2003/Abschlussbericht_G-DRG_V2004_0312191400_BII.pdf. Accessed 1 Feb 2006.
Verband der Privaten Krankenversicherunge.V. Die Private Krankenversicherung. Zahlenbericht 2002/2003. Köln.
OECD Health Data 2002: a comparative analysis of 30 countries. Organisation for Economic Co-operation and Development (OECD), Paris. Available at: http://www.OECD.org
Shorr AF, Susla GM, Kollef MH: Linezolid for treatment of ventilator-associated pneumonia: a cost-effective alternative to vancomycin. Crit Care Med 2004; 32: 137–143.
Mullins CD, Kuznik A, Shaya FT, Obeidat NA, Levine AR, Liu LZ, Wong W: Cost-effectiveness analysis of linezolid compared with vancomycin for the treatment of nosocomial pneumonia caused by methicillin-resistant Staphylococcus aureus. Clin Ther 2006; 28: 1184–1198.
Grau S, Alvarez-Lerma F, del Castillo A, Neipp R, Rubio-Terres C: Cost-effectiveness analysis of the treatment of ventilator-associated pneumonia with linezolid or vancomycin in Spain. J Chemother 2005; 17: 203–211.
Jairath N, Weinstein J: The Delphi methodology (part one): a useful administrative approach. Can J Nurs Adm 1994; 7: 29–42.
Jairath N, Weinstein J: The Delphi methodology (part two): a useful administrative approach. Can J Nurs Adm 1994; 7: 7–20.
Simoens S: Using the Delphi technique in economic evaluation: time to revisit the oracle? J Clin Pharm Ther 2006; 31: 519–522.
Akins RB, Tolson H, Cole BR: Stability of response characteristics of a Delphi panel: application of bootstrap data expansion. BMC Med Res Methodol 2005; 5: 37.
Beyersmann J, Gastmeier P, Grundmann H, Bärwolff S, Geffers C, Behnke M, Rüden H, Schumacher M: Use of multistate models to assess prolongation of intensive care unit stay due to nosocomial infection. Infect Control Hosp Epidemiol 2006; 27: 493–499.
Dietrich ES, Demmler M, Schulgen G, Fekec K, Mast O, Pelz K, Daschner FD: Nosocomial pneumonia: a cost-of-illness analysis. Infection 2002; 30: 61–67.
Author information
Authors and Affiliations
Corresponding author
Additional information
Part of this manuscript was presented at the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 7th Annual European Congress in Hamburg, Germany, October 2004.
Rights and permissions
About this article
Cite this article
De Cock, E., Krueger, W.A., Sorensen, S. et al. Cost-Effectiveness of Linezolid vs Vancomycin in Suspected Methicillin-Resistant Staphylococcus aureus Nosocomial Pneumonia in Germany. Infection 37, 123–132 (2009). https://doi.org/10.1007/s15010-008-8046-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-008-8046-7