
Abstract
Purpose
The costoclavicular block is a relatively novel alternative to the infraclavicular block. We aimed to determine the anatomical structures vulnerable to needle injury during a costoclavicular block.
Methods
The needle path consistent with a costoclavicular block approach was performed bilaterally on four lightly embalmed cadavers using ultrasound guidance. Careful dissection was performed with 18-G Tuohy needles in situ and photographs were taken.
Results
The needle penetrated the deltoid in six of eight cases and the pectoralis minor in three of eight cases. The subclavius tendon or its fascia were punctured in two of eight cases. The lateral cord was in contact with the needle in six procedures and punctured in three. The posterior cord was contacted in two instances, and the medial cord in one. In a single dissection, the needle was in contact with the medial antebrachial cutaneous nerve. The needle was close to the medial brachial cutaneous nerve in one case and close to the pectoral nerves in two of eight cases. While the cephalic vein and thoracoacromial artery were consistently nearby, there were no cases of vascular puncture.
Conclusion
We found that the needle path may be close to the medial antebrachial cutaneous nerve, medial brachial cutaneous nerve, and pectoral nerves but did not traverse any critical structures aside from the lateral cord. This suggests relative safety when compared with other approaches to the infraclavicular brachial plexus. Structures dans la trajectoire de l’aiguille du bloc de plexus brachial costoclaviculaire : une étude cadavérique
Résumé
Objectif
Le bloc costoclaviculaire est une alternative relativement nouvelle au bloc infraclaviculaire. Notre objectif était de déterminer quelles structures anatomiques étaient vulnérables aux lésions provoquées par l’aiguille pendant un bloc costoclaviculaire
Méthode
Nous avons simulé, sous échoguidage, une trajectoire d’aiguille correspondant à l’approche pour un bloc costoclaviculaire en bilatéral sur quatre cadavres légèrement embaumés. Une dissection minutieuse a ensuite été exécutée avec des aiguilles Tuohy 18-G laissées in situ et des photographies ont été prises.
Résultats
L’aiguille a pénétré le deltoïde dans six des huit cas et le muscle petit pectoral dans trois des huit cas. Le tendon sous-clavier ou son fascia ont été perforés dans deux des huit cas. Le cordon latéral a été en contact avec l’aiguille dans six interventions et perforé dans trois cas. Le cordon postérieur a été touché dans deux cas, et le cordon médial dans un cas. L’aiguille a touché le nerf cutané antébrachial médial dans une seule dissection. L’aiguille était proche du nerf cutané brachial médial dans un cas et proche des nerfs pectoraux dans deux des huit cas. Alors que la veine céphalique et l’artère thoraco-acromiale étaient toujours à proximité, il n’y a eu aucun cas de ponction vasculaire.
Conclusion
Nous avons constaté que la trajectoire de l’aiguille peut être à proximité du nerf cutané antébrachial médial, du nerf cutané brachial médial et du nerf pectoral, mais l’aiguille n’a pas traversé de structures critiques hormis le cordon latéral. Ceci suggère l’innocuité relative de ce type de bloc par rapport à d’autres approches du plexus brachial infraclaviculaire.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Infraclavicular brachial plexus block is often used for anesthesia and analgesia for elbow, forearm, and hand surgery.1 The traditional parasagittal (or coracoid) approach is not without risks: a steep insertion angle makes needle visualization challenging, the acromial branch of the thoracoacromial artery is vulnerable to puncture, and the lateral cord of the brachial plexus may lie in the needle path.2,3 The more recently introduced retroclavicular approach overcomes some of these disadvantages, but may place the suprascapular nerve and suprascapular vein at risk of needle damage.4
The first description of the costoclavicular brachial plexus block was published in 2015 by Karmakar et al.5 Their subsequent cadaver study showed a consistent arrangement of the cords and relative positions to the axillary artery within the costoclavicular space.6 The purported advantages of the costoclavicular approach are a shallow needle angle, a single injection point, and a reduction in required local anesthetic volume.7 A 2017 report detailed their success with the procedure and the consistent observed sonoanatomy with the costoclavicular block (CCB) in 30 patients undergoing hand or forearm surgery.7 A recent study described the spread of 20 mL methylene blue in cadavers after injection with the costoclavicular approach.8 Not surprisingly, the injectable spread was similar to what has been seen with other approaches to the infraclavicular region.8 Randomized controlled trials (RCTs) have shown either no difference in onset time and success rates9 or that the CCB results in faster onset and “readiness for surgery”.10 Nevertheless, given the novelty of the costoclavicular block, its safety profile remains unclear.
There are no published instances of neurologic injury due to a costoclavicular approach to the infraclavicular brachial plexus. Among five RCTs (232 patients)9,11,12,13,14 and two prospective cohort studies (87 patients),7,15 no patients were found to have residual sensory or motor deficits. Nevertheless, there were instances of vascular puncture (six patients), Horner’s syndrome (21 patients), and paresthesias (30 patients).9,12,13,15
To our knowledge, no cadaver study investigating the structures encountered by the needle during performance of the costoclavicular brachial plexus block exists. Our primary objective was to describe the anatomical structures penetrated by the needle during a CCB. The secondary aim was to make note of any critical structures close to the block needle.
Methods
This was a cadaver-based study where anatomical structures penetrated or adjacent to the needle were described following ultrasound-guided needle placement simulating a costoclavicular brachial plexus block. Following approval from the Dalhousie University Research Ethics Board, four lightly embalmed cadavers were independently selected by the manager of the Human Body Donation Program at Dalhousie University. This was a convenience sample rather than based on a sample size calculation aiming to represent all anatomical variations or a particular population. The sample was similar to that of other cadaver studies describing anatomy relevant to regional anesthesia techniques or spread of local anesthesia.4,8,16 Exclusion criteria included noted deformity or scarring of the shoulder or clavicular region. Reporting is consistent with the Anatomical Quality Assurance checklist.17 Dissections occurred between February and July of 2020.
Cadaver preparation
The four cadavers used in this study were lightly embalmed “surgical grade” cadavers. This technique has been described previously and results in supple tissue and excellent ultrasound images.4,18,19
Needle placement technique
All needle placements were performed by a regional anesthesia fellow (S.D.) with direct observation by an experienced regional anesthesiologist (V.U., J.B., K.K.). In each case, all observers agreed on the final needle placement prior to securing the needle. A SonoSite Edge (FUJIFILM SonoSite, Inc, Bothell, WA, USA) ultrasound machine in “resolution” mode and linear array transducer (7-13 MHz) were used to perform bilateral costoclavicular needle insertions on each cadaver using an 89-mm 18-G Arrow Tuohy needle (Arrow International, Reading, PA, USA). The needle was anchored in place by subsequent insertion of a 127-mm 22-G Arrow Quincke needle (Arrow International) through the Tuohy. An 18-G Tuohy was chosen because of its stiffness and the ability to pass another needle through it to limit needle movement during the dissection. Testing of this technique prior to performance revealed a snug fit between the needles following Quincke insertion making significant movement of the Tuohy needle unlikely.
The simulated CCB was performed as described by Li et al.7 The cadaver was placed supine with the ipsilateral arm abducted as much as possible (approximately 45°). The clavicle was palpated and the ultrasound probe placed just caudad to it in a transverse orientation. After identification of the axillary artery and the cords of the brachial plexus, the ultrasound view was optimized. Following achievement of optimal imaging and identification of the ideal needle path as agreed upon by two team members, the needle was inserted in-plane from a lateral to medial direction with the goal being insertion of the needle between the lateral and posterior cords of the brachial plexus (Electronic Supplementary Material [ESM] eFig. 1). Hydrodissection with normal saline was used to confirm needle placement. Following agreement that the needle was acceptably positioned, the needle was carefully braced while the spinal needle was gently inserted through the Tuohy needle. Both needles were left in place during the dissection process.
Cadaver dissection and examination
Dissections were performed by an experienced anatomist (R.S.). First, the skin cephalad to the clavicle was removed to reveal the trapezius, sternocleidomastoid, and brachial plexus emerging between the anterior and middle scalene muscles. The skin caudad to the clavicle was removed to reveal the deltoid, pectoralis major, and deltopectoral groove. Next, the pectoralis major was reflected to reveal the pectoralis minor. At this point, the cephalic vein and thoracoacromial artery were usually visible. Adipose and connective tissue were removed as needed to optimize the dissection field. The pectoralis minor was reflected, and as necessary, the cephalic vein, thoracoacromial artery and axillary vein were resected to allow identification of the brachial plexus and the needle tip. Following identification of the Tuohy’s tip, the anchoring Quincke needle was removed to allow for final photographs of the Tuohy’s position. Care was taken to ensure that the Tuohy remained in place. Further dissection was undertaken distally in the cadaver’s upper extremity as needed to definitively establish the identity of the nearby neural structures. For example, the lateral cord could be confirmed by following its course distally to its contribution to the median nerve in addition to the musculocutaneous nerve.
Results
Eight bilateral costoclavicular blocks and dissections were performed on four cadavers. None of the cadavers had scarring or deformity suggestive of previous shoulder or clavicle surgery. Cadaver 2 had a port implanted into the right axillary vein, but our block procedure did not appear to be affected. The demographic characteristics of the cadavers are described in Table 1.
In all four cadavers, we were able to identify the sonoanatomy relevant to the costoclavicular approach (pectoralis major, pectoralis minor, axillary artery adjacent to the brachial plexus cords, ribs, and pleura). The axillary vein was difficult to visualize given that it was collapsed in the cadavers. Visualization of other arteries was difficult because pulsatile flow was lacking; however, the axillary artery was universally identified sonographically. In all cases, a final needle position between the cords of the brachial plexus was confirmed by ultrasound visualization of the needle tip and hydrodissection with saline. Needle visualization, including demonstration of the tip position, was satisfactory in all cases. The dissection results are presented in Table 2.
Following insertion through the skin and subcutaneous tissues, the needle passed through the medial aspect of the deltoid muscle in six of eight approaches. In three of eight cases, the needle traversed the lateral aspect of the pectoralis minor muscle. In two of eight approaches, the needle passed through the subclavius tendon or its fascia. In one case, it was very difficult to pass the needle as described without hitting the coracoid process; some repositioning and needle redirection were required. In one instance, the cords of the brachial plexus surrounded the axillary artery rather than being adjacent to one another as per the classical description of the costoclavicular approach.
In three cases, the needle penetrated the lateral cord. In all other cases, the needle shaft or tip was in contact with the lateral cord. In one dissection, the needle tip was in contact with the medial cord after passing between the lateral and posterior cords (Fig. 1). Another dissection showed the needle to be contacting the medial antebrachial cutaneous nerve, while very close to the medial brachial cutaneous nerve (Fig. 2). Upon dissection, the medial cord was found to lie posterior (or deep) to the axillary artery (ESM eFig. 2). In two of eight instances, the needle path was close (< 2 cm) to the lateral and medial pectoral nerves. In four of eight cases the needle path was close to the deltoid branch of the thoracoacromial artery. Similarly, the cephalic vein was close to the needle path in six of eight cases. There were no instances of the needle puncturing vascular structures.

Needle between lateral and posterior cords, contacting medial cord. AA = axillary artery; Caud = caudad; LC = lateral cord; MC = medial cord; Med = medial; PC = posterior cord.

Needle in contact with lateral cord and medial antebrachial cutaneous nerve. Note that the two peripheral nerves are emerging from the medial cord, which is obscured in the photo. AA = axillary artery; ceph = cephalad; lat = lateral; LC = lateral cord; MAbC = medial antebrachial cutaneous nerve; MBC = medial brachial cutaneous nerve; TAA = thoracoacromial artery.
Discussion
The cadaver dissections in our study showed that there are important anatomical structures susceptible to needle injury during CCB. While clinical studies are required to establish the magnitude of safety and efficacy of novel blocks, cadaver studies such as this one contribute to anatomical understanding and guide techniques to minimize injury. Our study described the structures penetrated and in close proximity to the needle path during the performance of the costoclavicular approach to the infraclavicular brachial plexus. The intent was to establish biological plausibility of neurovascular injury.
The costoclavicular approach to the infraclavicular brachial plexus was originally proposed in 20155 as a solution to problems with the classical (i.e., parasagittal or coracoid) approach. Namely, the coracoid approach is associated with poor needle visualization due to steep angle of insertion. The lateral cord is in the needle path and the medial cord may be spared with a single injection.2,3,20 To perform the costoclavicular block, the patient is positioned supine with their arm abducted.7 The recommended ultrasound scanning method is to place the transducer on top of and parallel with the clavicle before sliding just caudad to the edge of the clavicle (Fig. 3).7 This view of the brachial plexus in the costoclavicular space is more proximal than in the coracoid approach. At this level, the lateral, posterior, and medial cords are tightly clustered lateral to the first part of the axillary artery (Fig. 4a). The needle is advanced from lateral to medial in-plane with the ultrasound transducer. In a previous cadaveric dissection of the costoclavicular space, it was noted that the cephalic vein and the thoracoacromial artery were both in close proximity to the needle path.6 Therefore, it is recommended that the practitioner scans laterally and caudal until the cephalic vein and thoracoacromial artery come into view (Fig. 4b and 4c).7 The transducer is then returned to its original position and the image is optimized after those vascular structures have been identified. In Karmakar et al.’s original description of the block, a final needle tip position between the tightly clustered cords was recommended.5,7 A cadaver study showed that injected dye mimicking a CCB stained all three trunks, divisions, all three cords, and the C7-T1 roots of the brachial plexus in five of five injections.8 In a clinical study, a single injection of 20 mL of local anesthetic resulted in complete sensory and motor blockade (median [interquartile range (IQR)] time of 30 [20-30] min and 20 [20-30] min, respectively).7 The same study found that the median [IQR] time to readiness for surgery was 10 [5-20] min.7 The median time to readiness was faster than the coracoid approach in a RCT.10 Two RCTs found that CCBs resulted in significantly lower incidence of diaphragmatic hemiparesis than supraclavicular blocks did (2.5-5% vs 40-45%, respectively).14,21 In the dye distribution study mentioned above, the suprascapular nerve was routinely stained.8 This may explain why a recent non-inferiority trial found that costoclavicular blocks resulted in equivalent pain scores as interscalene blocks after arthroscopic shoulder surgery.11

Relevant anatomy and ultrasound transducer position for performing a costoclavicular brachial plexus block.

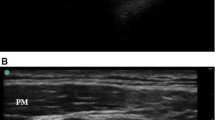
Sonoanatomy and paired representative illustrations of the critical structures identified during a costoclavicular brachial plexus block. A) Sonogram and illustration of the typical view during a costoclavicular block. Note that the cords are adjacent to one another lying lateral to the axillary artery. B) Moving the transducer in a caudal and lateral direction displays the cephalic vein overlying the brachial plexus. C) Further translation of the transducer brings the deltoid branch of the thoracoacromial artery into view.
In our study, the muscles penetrated by the needle varied somewhat, although the deltoid was traversed in six of the eight procedures. The pectoralis minor and subclavius were punctured less frequently. It is possible that penetrating less muscle reduces procedural pain as some groups have speculated previously.22 Nevertheless, a randomized trial found similar procedural pain scores between the costoclavicular and paracoracoid approaches.9 Similarly, there were no differences in procedural pain between the infraclavicular block and either supraclavicular or axillary blocks.22,23,24 The amount of muscle tissue traversed may influence the likelihood of catheter dislodgement. It has been suggested that passing through the pectoral muscles helped to prevent dislodgement.25
Our study identified neurovascular structures at risk of injury because of proximity to the needle path. This study confirmed the that deltoid branch of the thoracoacromial artery and the cephalic vein are close to the needle path. Vascular structures can easily be avoided using this approach, but it is advised that practitioners carefully interrogate the area prior to passing the needle. Colour or power doppler ultrasound may assist in identifying and avoiding vascular structures.26,27 Caution is required in the case of anticoagulated patients. The CCB is considered deep and moderately-compressible and provides limited ability to clinically visualize a hematoma; therefore, recommendations for intermediate risk blocks similar to other blocks in the infraclavicular region should be followed.28,29 Although the needle did not contact these structures in our dissections, we found that the needle path was in close proximity to the medial brachial cutaneous nerve and medial antebrachial cutaneous nerves in one case, and to the lateral and medial pectoral nerves in two cases. The medial brachial cutaneous nerves and the medial antebrachial cutaneous nerves were found to branch from the medial cord close to the needle end point of the block in one cadaver. The medial brachial cutaneous and medial antebrachial cutaneous nerves are most commonly branches of the medial cord, arising in the infraclavicular region.30 The lateral and medial pectoral nerves are branches of the lateral and medial cords, respectively, joined together by the ansa pectoralis.30 Performing the block in an awake patient with nerve stimulation may decrease the possibility of inadvertent nerve injury.31,32
In this study, the lateral cord was consistently in contact with the block needle. This is unsurprising since the block technique involves placing the needle between the lateral and posterior cords. Nevertheless, caution is warranted when injecting between the often tightly grouped cords in this approach. Analogously, intra-cluster injections at the supraclavicular brachial plexus were found to result in a 24% rate of inadvertent subperineural injections in a cadaver study.18 Adding nerve stimulation to ultrasound localization at low current and performance of the block on an alert patient who is advised to report paresthesias are two potential safety precautions. Although peripheral nerve stimulation cannot absolutely rule out subepineural position, stimulation < 0.2 mA reliably indicates intraneural needle position or needle-nerve contact.31,32 Whether similar clinical results can be achieved with injection outside of the bundle of cords warrants further study. A randomized trial compared a single injection to a double injection technique using a costoclavicular approach.12 The double injection resulted in a shorter onset time and longer anesthesia with similar performance time and procedural pain. Nevertheless, in both cases, local anesthesia was injected between the tightly grouped cords.12 A non-inferiority trial compared costoclavicular blocks using a double injection technique outside the group of cords to supraclavicular blocks.13 In that study, equivalent proportions of patients had complete sensory and motor blockade in each group.13 Time to onset of blockade was also equivalent; however, there was greater difficulty, worse needle visualization, more needle passes, and longer performance time in the costoclavicular group.13
The present study does have several limitations. Our sample size was limited to eight dissections, which makes the results susceptible to individual anatomical variation in the cadaver specimens. Anatomical variations are common within the human population, and any variation encountered here could be encountered in clinical practice.33 The cadavers were lightly embalmed, which made them less stiff than formalin-embalmed or fresh-frozen cadavers; however, the tissues were more stiff than in vivo conditions.34 We were not able to abduct the arms further than 45°, possibly because muscles cannot be fully lengthened in cadavers. This may have influenced the position of infraclavicular neurovascular structures relative to the clavicle.35 Tissues cannot be easily visualized in cadaver specimens because of edema, decreased tissue elasticity, and non-pulsatile, collapsed vasculature. This contributed to our needle not always being placed between the lateral and posterior cords as described by Li et al.7 A Tuohy needle was selected rather than an echogenic 22-G block needle typically used in single shot regional techniques. Despite the potential for decreased needle visualization, we were able to satisfactorily visualize the needle in all cases. Another limitation is that it is not possible to stimulate motor responses or receive information about paresthesias. These limitations may lead to increased instances of needle contact with critical structures and likely explain the three cases of lateral cord puncture we observed. Since the dissection proceeded through subsequent layers from superficial to deep, it is more difficult to judge the proximity of structures above and below the plane of dissection. Given that veins and arteries were more easily collapsible in cadaver models, this could lead to more vascular punctures. Nevertheless, this study did not attempt to estimate rates of puncture, rather only structures at risk of puncture. Lastly, the clinical implications of any injury are impossible to determine in cadavers.
Conclusion
The costoclavicular brachial plexus block is a relatively new technique described with the potential advantages of improved needle visualization due to a reduced angle of insonation compared with the coracoid approach, and avoidance of the acoustic shadow of the retroclavicular approach. We found that the needle path may be close to the cephalic vein, thoracoacromial artery, medial antebrachial cutaneous, medial brachial cutaneous, and pectoral nerves but did not traverse any critical structures apart from the lateral cord. This suggests relative safety compared with other approaches to the infraclavicular region of the brachial plexus. Future research should compare injection between the cords to double injection outside the cords in terms of effectiveness, safety, and patient comfort.
References
Chin KJ, Singh M, Velayutham V, Chee V. Infraclavicular brachial plexus block for regional anaesthesia of the lower arm. Anesth Analg 2010. DOI: https://doi.org/10.1213/ANE.0b013e3181dbac5d.
Kalagara HK, Uppal V, McKinlay S, Macfarlane AJ, Anderson K. Effect of body mass index on angle of needle insertion during ultrasound-guided lateral sagittal infraclavicular brachial plexus block. J Clin Anesth 2015; 27: 375-9.
Sutton EM, Bullock WM, Gadsden J. The retroclavicular brachial plexus block additional advantages. Reg Anesth Pain Med 2015; 40: 733-4.
Sancheti SF, Uppal V, Sandeski R, Kwofie MK, Szerb JJ. A cadaver study investigating structures encountered by the needle during a retroclavicular approach to infraclavicular brachial plexus block. Reg Anesth Pain Med 2018; 43: 752-5.
Karmakar MK, Sala-Blanch X, Songthamwat B, Tsui BC. Benefits of the costoclavicular space for ultrasound-guided infraclavicular brachial plexus block: description of a costoclavicular approach. Reg Anesth Pain Med 2015; 40: 287-8.
Sala-Blanch X, Reina MA, Pangthipampai P, Karmakar MK. Anatomic basis for brachial plexus block at the costoclavicular space: a cadaver anatomic study. Reg Anesth Pain Med 2016; 41: 387-91.
Li JW, Songthamwat B, Samy W, Sala-Blanch X, Karmakar MK. Ultrasound-guided costoclavicular brachial plexus block sonoanatomy, technique, and block dynamics. Reg Anesth Pain Med 2017; 42: 233-40.
Koyyalamudi V, Langley NR, Harbell MW, Kraus MB, Craner RC, Seamans DP. Evaluating the spread of costoclavicular brachial plexus block: an anatomical study. Reg Anesth Pain Med 2020; 46: 31-4.
Leurcharusmee P, Elgueta MF, Tiyaprasertkul W, et al. A randomized comparison between costoclavicular and paracoracoid ultrasound-guided infraclavicular block for upper limb surgery. Can J Anesth 2017; 64: 617-25.
Songthamwat B, Karmakar MK, Li JW, Samy W, Mok LY. Ultrasound-guided infraclavicular brachial plexus block: prospective randomized comparison of the lateral sagittal and costoclavicular approach. Reg Anesth Pain Med 2018; 43: 825-31.
Aliste J, Bravo D, Layera S, et al. Randomized comparison between interscalene and costoclavicular blocks for arthroscopic shoulder surgery. Reg Anesth Pain Med 2019. DOI: https://doi.org/10.1136/rapm-2018-100055.
Layera S, Aliste J, Bravo D, et al. Single- versus double-injection costoclavicular block: a randomized comparison. Reg Anesth Pain Med 2020; 45: 209-13.
Luo Q, Yao W, Chai Y, et al. Comparison of ultrasound-guided supraclavicular and costoclavicular brachial plexus block using a modified double-injection technique: a randomized non-inferiority trial. Biosci Rep 2020. DOI: https://doi.org/10.1042/bsr20200084.
Sivashanmugam T, Maurya I, Kumar N, Karmakar MK. Ipsilateral hemidiaphragmatic paresis after a supraclavicular and costoclavicular brachial plexus block: a randomised observer blinded study. Eur J Anaesthesiol 2019; 36: 787-95.
Sotthisopha T, Elgueta MF, Samerchua A, et al. Minimum effective volume of lidocaine for ultrasound-guided costoclavicular block. Reg Anesth Pain Med 2017; 42: 571-4.
Mayes J, Davison E, Panahi P, et al. An anatomical evaluation of the serratus anterior plane block. Anaesthesia 2016; 71: 1064-9.
Tomaszewski KA, Henry BM, Kumar Ramakrishnan P, et al. Development of the Anatomical Quality Assurance (AQUA) checklist: Guidelines for reporting original anatomical studies. Clin Anat 2017; 30: 14-20.
Retter S, Szerb J, Kwofie K, Colp P, Sandeski R, Uppal V. Incidence of sub-perineural injection using a targeted intracluster supraclavicular ultrasound-guided approach in cadavers. Brit J Anaesth 2019; 122: 776-81.
Szerb JJ, Greenberg JL, Kwofie MK, et al. Histological confirmation of needle tip position during ultrasound-guided interscalene block: a randomized comparison between the intraplexus and the periplexus approach. Can J Anesth 2015; 62: 1295-302.
Rodríguez J, Bárcena M, Taboada-Muñiz M, Lagunilla J, Alvarez J. A comparison of single versus multiple injections on the extent of anesthesia with coracoid infraclavicular brachial plexus block. Anesth Analg 2004; 99: 1225-30.
Oh C, Noh C, Eom H, et al. Costoclavicular brachial plexus block reduces hemidiaphragmatic paralysis more than supraclavicular brachial plexus block: retrospective, propensity score matched cohort study. Korean J Pain 2020; 33: 144-52.
Frederiksen BS, Koscielniak-Nielsen ZJ, Jacobsen RB, Rasmussen H, Hesselbjerg L. Procedural pain of an ultrasound-guided brachial plexus block: a comparison of axillary and infraclavicular approaches. Acta Anaesthesiol Scand 2010; 54: 408-13.
Yazer MS, Finlayson RJ, Tran DQ. A randomized comparison between infraclavicular block and targeted intracluster injection supraclavicular block. Reg Anesth Pain Med 2015; 40: 11-5.
Vazin M, Jensen K, Kristensen DL, et al. Low-volume brachial plexus block providing surgical anesthesia for distal arm surgery comparing supraclavicular, infraclavicular, and axillary approach: a randomized observer blind trial. Biomed Res Int 2016. DOI: https://doi.org/10.1155/2016/7094121.
Atchabahian A, Vandepitte C, Lopez AM. Ultrasound-Guided Infraclavicular Brachial Plexus Block. 2020. Available from URL: https://www.nysora.com/regional-anesthesia-for-specific-surgical-procedures/upper-extremity-regional-anesthesia-for-specific-surgical-procedures/anesthesia-and-analgesia-for-elbow-and-forearm-procedures/ultrasound-guided-infraclavicular-brachial-plexus-block/ (accessed March 2021).
Renes S, Clark L, Gielen M, Spoormans H, Giele J, Wadhwa A. A simplified approach to vertical infraclavicular brachial plexus blockade using hand-held Doppler. Anesth Analg 2008; 106: 1012-4.
Nagdev A, Hahn C. Color Doppler ultrasound-guided supraclavicular brachial plexus block to prevent vascular injection. West J Emerg Med 2014; 15: 703-5.
Tsui BC, Kirkham K, Kwofie MK, et al. Practice advisory on the bleeding risks for peripheral nerve and interfascial plane blockade: evidence review and expert consensus. Can J Anesth 2019; 66: 1356-84.
Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine. Evidence-Based Guidelines (Fourth Edition). Reg Anesth Pain Med 2018; 43: 263-309.
Netter FH. Atlas of Human Anatomy -. 6th ed. Philadelphia, PA: Elsevier Inc.; 2014 .
Neal JM, Barrington MJ, Brull R, et al. The second ASRA practice advisory on neurologic complications associated with regional anesthesia and pain medicine: Executie Summary 2015. Reg Anesth Pain Med 2015; 40: 401-30.
Neal JM. The role of nerve localization techniques in safety. In: Neal JM, Rathmell JP, editors. Complications in Regional Anesthesia and Pain Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2013. p. 188-95.
Emamhadi M, Chabok SY, Samini F, et al. Anatomical variations of brachial plexus in adult cadavers; a descriptive study. Arch Bone Jt Surg 2016; 4: 253-8.
Sawhney C, Lalwani S, Ray BR, Sinha S, Kumar A. Benefits and pitfalls of cadavers as learning tool for ultrasound-guided regional anesthesia. Anesth Essays Res 2017; 11: 3-6.
Auyong DB, Gonzales J, Benonis JG. The Houdini clavicle: arm abduction and needle insertion site adjustment improves needle visibility for the infraclavicular nerve block. Reg Anesth Pain Med 2010; 35: 403-4.
Author contributions
Jonathan Bailey contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Sean Donald contributed to acquisition, analysis, and interpretation of data and drafting the article. Kwesi Kwofie contributed to acquisition, analysis, and interpretation of data and revision of the article. Robert Sandeski contributed to acquisition of data and revision of the article. Vishal Uppal contributed to study conception and design; acquisition, analysis, and interpretation of data; and revision of the article.
Acknowledgements
The authors thank the individuals and families of those that generously donated their bodies to science.
Disclosures
None.
Funding statement
The authors thank the Dalhousie University Department of Anesthesia, Pain & Perioperative Medicine for their support of this study by means of a departmental grant.
Editorial responsibility
This submission was handled by Dr. Philip M. Jones, Deputy Editor-in-Chief, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
12630_2021_1990_MOESM1_ESM.pdf
Supplementary file 1 eFig. 1 Ultrasound image of costoclavicular block. AA, axillary artery; BP, brachial plexus. eFig 2 Needle in contact with lateral cord. AA, axillary artery; ceph, cephalad; lat, lateral; LC, lateral cord; MC, medial cord; PC, posterior cord. (PDF 3018 KB)
Rights and permissions
About this article

Cite this article
Bailey, J.G., Donald, S., Kwofie, M.K. et al. Critical structures in the needle path of the costoclavicular brachial plexus block: a cadaver study. Can J Anesth/J Can Anesth 68, 1156–1164 (2021). https://doi.org/10.1007/s12630-021-01990-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-021-01990-8