
Abstract
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has put tremendous pressure on healthcare systems. Most transcatheter aortic valve implantation (TAVI) centres have adopted different triage systems and procedural strategies to serve highest-risk patients first and to minimise the burden on hospital logistics and personnel. We therefore assessed the impact of the COVID-19 pandemic on patient selection, type of anaesthesia and outcomes after TAVI.
Methods
We used data from the Netherlands Heart Registration to examine all patients who underwent TAVI between March 2020 and July 2020 (COVID cohort), and between March 2019 and July 2019 (pre-COVID cohort). We compared patient characteristics, procedural characteristics and clinical outcomes.
Results
We examined 2131 patients who underwent TAVI (1020 patients in COVID cohort, 1111 patients in pre-COVID cohort). EuroSCORE II was comparable between cohorts (COVID 4.5 ± 4.0 vs pre-COVID 4.6 ± 4.2, p = 0.356). The number of TAVI procedures under general anaesthesia was lower in the COVID cohort (35.2% vs 46.5%, p < 0.001). Incidences of stroke (COVID 2.7% vs pre-COVID 1.7%, p = 0.134), major vascular complications (2.3% vs 3.4%, p = 0.170) and permanent pacemaker implantation (10.0% vs 9.4%, p = 0.634) did not differ between cohorts. Thirty-day and 150-day mortality were comparable (2.8% vs 2.2%, p = 0.359 and 5.2% vs 5.2%, p = 0.993, respectively).
Conclusions
During the COVID-19 pandemic, patient characteristics and outcomes after TAVI were not different than before the pandemic. This highlights the fact that TAVI procedures can be safely performed during the COVID-19 pandemic, without an increased risk of complications or mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
-
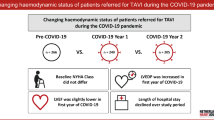
The clinical characteristics of patients undergoing transcatheter aortic valve implantation (TAVI) during the COVID-19 pandemic (COVID cohort) were comparable to those of patients undergoing TAVI during the pre-COVID-19 era (pre-COVID cohort).
-
The percentage of TAVI procedures performed using general anaesthesia was lower in the COVID cohort, with more transaxillary and fewer transapical TAVIs in the COVID cohort compared to the pre-COVID cohort.
-
TAVI procedures can be safely performed amid the COVID-19 pandemic, without an increased risk of complications or mortality.
-
The COVID-19 pandemic might have accelerated the shift towards more TAVI procedures with local anaesthesia/conscious sedation, a trend which was already observed before this ongoing pandemic.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has put tremendous pressure on healthcare systems worldwide, leading to the deferment of large numbers of elective procedures [1, 2]. Patients with symptomatic severe aortic stenosis (AS) have a poor prognosis if left untreated, with an annual mortality of approximately 50% [3].
Transcatheter aortic valve implantation (TAVI) is an established, minimally invasive treatment option in patients with severe AS, a condition which is found in a predominantly elderly, vulnerable population with serious comorbidities. Postponement of this potentially life-saving procedure is associated with a risk of sudden cardiac death or irreversible cardiac deterioration. Previous literature reported a ‘waiting list’ mortality rate of 23.3% and 27.5% at 6 and 12 months, respectively, in patients awaiting TAVI [4]. Data from the UK TAVI Registry demonstrated a significant decrease in TAVI activity following the COVID-19 outbreak with an estimated 5000 patients with severe AS not receiving treatment (either surgical aortic valve replacement (SAVR) or TAVI) during the period March to November 2020 [5].
Multiple position statements have been published on when to perform TAVI for symptomatic severe AS amid the COVID-19 crisis [6,7,8,9]. However, the risks of adverse events caused by postponement of these interventions should be balanced against the risks of contracting COVID-19 when hospitalised for this high-risk cardiovascular intervention [10]. Also, most TAVI centres have adopted different triage systems and different procedural strategies during the COVID-19 pandemic, aiming to serve highest-risk patients first and to minimise the burden on hospital logistics and personnel [11].
We previously reported on the safety and feasibility of a continued TAVI programme during the COVID-19 pandemic in our own centre [10]. Here we present data from the Netherlands Heart Registration (NHR), a nationwide registry in which data on all cardiac interventions performed in the Netherlands are collected. We studied whether the implementation of a different triage system during the COVID-19 pandemic led to a different ‘case mix’ of TAVI patients. We also assessed whether the COVID-19 pandemic, with its associated reduction in the number of available intensive care unit (ICU) beds and anaesthesiologists, has led to a shift from general anaesthesia to local anaesthesia. Finally, we studied whether the outcomes in terms of complications and mortality after TAVI were different during the COVID-19 pandemic as compared to the pre-COVID-19 era.
Methods
Data collection
In the NHR, data on all cardiac interventions performed in the Netherlands are registered by all Dutch heart centres. Data are reported per site and collected on a yearly basis. During the study period, 15 of these hospitals performed TAVI procedures (Table S1, Electronic Supplementary Material). Data are collected on patient characteristics, procedural characteristics and outcome variables [12]. Data collection and registration are performed by the participating centres in a secure online environment. A waiver of consent for the NHR data registration was obtained from the Medical Ethics Committee. The study was conducted in accordance with the guiding principles of the Declaration of Helsinki. In order to obtain data for research purposes, the data request must be reviewed and approved by the NHR [13]. Only data necessary to answer the prespecified research questions are provided. To prevent identification of centre-specific data, requested variables are provided for all TAVI centres together.
Population and design
In this nationwide, retrospective multicentre study, we examined all patients who underwent a TAVI procedure for symptomatic severe AS between March 2020 and July 2020 (COVID cohort), and between March 2019 and July 2019 (pre-COVID cohort). We specifically selected these 5‑month periods since the period from March 2020 to July 2020 comprised the first COVID-19 wave in the Netherlands [14]. The maximum follow-up duration of 150 days was determined by the period between final data extraction and the date of the TAVI procedure of the last patient included in the COVID cohort.
Procedure
All centres performed TAVI according to their respective local protocols. Type of TAVI device, valve size and TAVI access were left to the operator’s discretion. The TAVI procedure was performed using general anaesthesia or local anaesthesia with or without conscious sedation.
Endpoints
The primary endpoint was mortality at 150 days. Secondary endpoints included procedural mortality (defined as mortality within 72 h after the intervention), mortality at 30 days, stroke during hospitalisation, major vascular complications according to Valve Academic Research Consortium (VARC) criteria [15], permanent pacemaker implantation and aortic valve reintervention within 150 days.
Statistical analysis
Categorical variables are presented as number with percentage. Continuous variables are presented as mean with standard deviation or median with interquartile range (IQR), depending on distribution. Categorical variables were compared using the chi-square or Fisher’s exact test, as appropriate. Continuous variables were compared using Student’s t-test or Mann-Whitney U test, as appropriate. Survival was estimated by means of Kaplan-Meier analysis and was compared with the use of the log-rank test. A p-value of < 0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics software version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
We examined a total of 2131 patients, of whom 1020 underwent a TAVI procedure between March 2020 and July 2020 (COVID cohort) and 1111 underwent a TAVI procedure between March 2019 and July 2019 (pre-COVID cohort). Of the 1020 patients treated with TAVI in the COVID cohort, 38 (3.7%) were initially planned for SAVR. Baseline characteristics are shown in Tab. 1. Mean age was 79.2 ± 6.9 years and 54.2% of patients were men. The majority of baseline characteristics did not differ between the two time periods, but exceptions were previous aortic valve surgery (COVID 5.1% vs pre-COVID 3.2%, p = 0.032), extracardiac arterial pathology (15.7% vs 19.6%, p = 0.019), previous stroke (13.2% vs 10.2%, p = 0.029) and left ventricular ejection fraction (49.8% vs 50.8%, p = 0.028). EuroSCORE II was comparable (COVID 4.5 ± 4.0 vs pre-COVID 4.6 ± 4.2, p = 0.356). New York Heart Association class was lower in the COVID cohort, whereas the proportion of emergent TAVI procedures was higher in the COVID cohort (COVID 0.6% vs pre-COVID 0%, p = 0.012).
Procedural characteristics
Details about procedural characteristics are provided in Tab. 2. A total of 875 (41.1%) TAVI procedures were performed using general anaesthesia, with a significantly lower proportion in the COVID cohort as compared to the pre-COVID cohort (35.2% vs 46.5%, p < 0.001) (Fig. 1). The transfemoral approach was predominantly used (85.8%), followed by the transaxillary (6.0%), direct transaortic (4.9%) and transapical (3.2%) approaches. The transaxillary approach was used more frequently in the COVID cohort (7.8% vs 4.4%, p = 0.001) and the transapical approach less frequently (2.2% vs 4.1%, p = 0.013) when compared to the pre-COVID cohort.

Type of anaesthesia used
Clinical outcomes
Clinical outcomes are presented in Tab. 3. Median duration of hospitalisation was 4 (IQR 3–7) days, which was comparable between the two groups. The incidences of stroke during hospitalisation (COVID 2.7% vs pre-COVID 1.7%, p = 0.134), major vascular complications within 30 days (2.3% vs 3.4%, p = 0.170), permanent pacemaker implantation (10.0% vs 9.4%, p = 0.634), aortic valve reintervention within 30 days (0.2% vs 0.3%, p = 1.000) and aortic valve reintervention within 150 days (0.5% vs 0.7%, p = 0.754) did not differ significantly between the two time periods. Procedural mortality (COVID 0.9% vs pre-COVID 1.0%, p = 0.853), 30-day mortality (2.8% vs 2.2%, p = 0.359) and 150-day mortality (5.2% vs 5.2%, p = 0.993) were comparable between the two groups. Fig. 2 depicts the Kaplan-Meier survival curves.

Kaplan-Meier survival curves
Discussion
In this nationwide cohort study, we compared the patient characteristics, procedural characteristics and clinical outcomes of a patient cohort undergoing TAVI amid the COVID-19 pandemic to a cohort undergoing TAVI in the same time period a year before (pre-COVID-19).
The key findings can be summarised as follows. First, regarding case mix changes, mean EuroSCORE II was similar (COVID 4.5 vs pre-COVID 4.6) in both cohorts. Second, the percentage of TAVI procedures performed using general anaesthesia was lower in the COVID cohort (35.2% vs 46.5%), with more transaxillary and fewer transapical TAVIs in the COVID cohort compared to the pre-COVID cohort (7.8% vs 4.4% and 2.2% vs 4.1%, respectively). Third, the 30-day and 150-day mortality in the two cohorts was comparable (COVID 2.8% and 5.2% vs pre-COVID 2.2% and 5.2%, respectively) with a comparable complication rate (i.e. stroke, major vascular complication, permanent pacemaker implantation and aortic valve reintervention).
Our data support the hypothesis that TAVI procedures can be safely performed amid this global crisis, with mortality and complication rates comparable to the pre-COVID era. These findings are consistent with previous research reporting on the safety and feasibility of a continued TAVI programme during the COVID-19 pandemic, without an increased risk of complications or mortality [16, 17].
The EuroSCORE II, a risk score used to predict 30-day mortality, did not differ between the two time periods. This indicates that, although a different triage system was adopted by most centres in the Netherlands at the height of the COVID-19 pandemic, factors other than the EuroSCORE (e.g. patient symptomatology and echocardiographic features) are used for triage.
During the COVID-19 pandemic, general anaesthesia has been used less frequently than during the reference period. A plausible explanation might be that the ICU capacity was mainly reserved for COVID-19 patients needing endotracheal intubation and ventilation. In addition, as a result of the established safety of local anaesthesia protocols in the literature [18], the increased adoption of local anaesthesia/conscious sedation may also have been observed independent of this pandemic. The majority of TAVI procedures are performed using a transfemoral approach, which facilitates the use of local anaesthesia/conscious sedation instead of general anaesthesia. The increased use of local anaesthesia/conscious sedation was not accompanied by an increase in adverse clinical outcomes, which is in line with previous reports [18, 19].
Some centres have introduced a nurse-led TAVI approach in selected transfemoral TAVI patients, in which the catheterisation laboratory nurse administers local anaesthesia [11]. In order to further reduce the burden on hospital logistics and personnel, a same-day discharge approach can be used in carefully selected patients following uncomplicated TAVI, achieving similar 30-day outcomes to those with a next-day discharge [20].
It might be expected that some surgical candidates would be treated with TAVI instead of SAVR, resulting in a larger decrease in SAVRs than in TAVIs in the COVID cohort. However, this is not supported by the relatively low number of TAVI patients (3.7%) that were initially planned for SAVR. Also, in the NHR handbook published online, the total numbers of TAVIs and SAVRs performed in 2019 and 2020 are provided [21].
The total numbers of TAVI procedures in 2019 and 2020 were 2791 and 2539, respectively, showing a decrease of 9.0%. Regarding SAVR, the respective total numbers in 2019 and 2020 were 1365 and 1268, corresponding to a decrease of 7.1%. Thus, the percentage decrease in the total number of procedures performed in 2020 (COVID year) was not higher for SAVR than for TAVI.
Limitations
First, all data were collected in the NHR. The Dutch Society of Cardiology and Dutch Society of Cardiothoracic Surgery determine on an annual basis which variables must be provided by TAVI centres, thus limiting the data we can provide in the present study. The number of mandatory outcome variables is relatively small, and therefore some VARC-3-related endpoints are missing (e.g. data on bleeding complications and rehospitalisation) [15]. Second, we only have cumulative data rather than data specifically related to individual TAVI centres. Therefore, inter-hospital differences could not be assessed. Third, since we only had access to data regarding TAVI, data regarding SAVR are lacking in our analysis. Finally, data on long-term follow-up were not yet available for the present analysis.
Future perspectives
Although the number of COVID-19 vaccine doses administered globally is as high as 11.3 billion, and the number of fully vaccinated persons has passed 4.5 billion [22], there is a continuous risk of (re)infection. In the case of increasing COVID-19 admissions, the strain on healthcare systems can potentially be diminished by using a same-day discharge approach in selected TAVI patients [20]. The problem of a relative unavailability of ICU capacity during future COVID-19 waves can be solved by using a minimalist TAVI [23] or nurse-led TAVI approach with only local anaesthesia [11].
Conclusion
In conclusion, we have demonstrated that the case mix of patients undergoing TAVI during the COVID-19 pandemic did not differ substantially from that before this crisis. While the number of TAVI procedures in both cohorts was nearly the same, a significantly lower percentage of patients underwent the TAVI procedure under general anaesthesia, with more transaxillary and fewer transapical TAVIs compared to the situation pre-COVID-19. The outcomes in terms of complications and mortality after TAVI during the COVID-19 pandemic are comparable to those in the pre-COVID-19 era.
References
Søreide K, Hallet J, Matthews JB, et al. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. Br J Surg. 2020;107(10):1250–61.
Gaudino M, Chikwe J, Hameed I, Robinson NB, Fremes SE, Ruel M. Response of cardiac surgery units to COVID-19: an internationally-based quantitative survey. Circulation. 2020;142(3):300–2.
Kapadia SR, Leon MB, Makkar RR, et al. 5‑year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385(9986):2485–91.
Malaisrie SC, McDonald E, Kruse J, et al. Mortality while waiting for aortic valve replacement. Ann Thorac Surg. 2014;98(5):1564–70. discussion 70–71.
Martin GP, Curzen N, Goodwin AT, et al. Indirect impact of the COVID-19 pandemic on activity and outcomes of transcatheter and surgical treatment of aortic stenosis in England. Circ Cardiovasc Interv. 2021;14(5):e10413.
Tay EL, Hayashida K, Chen M, et al. Transcatheter aortic valve implantation during the COVID-19 pandemic: clinical expert opinion and consensus statement for Asia. J Card Surg. 2020;35(9):2142–6.
Shah PB, Welt FGP, Mahmud E, et al. Triage considerations for patients referred for structural heart disease intervention during the COVID-19 pandemic: an ACC/SCAI position statement. JACC Cardiovasc Interv. 2020;13(12):1484–8.
Tanguturi VK, Lindman BR, Pibarot P, et al. Managing severe aortic stenosis in the COVID-19 era. JACC Cardiovasc Interv. 2020;13(16):1937–44.
Lauck S, Forman J, Borregaard B, et al. Facilitating transcatheter aortic valve implantation in the era of COVID-19: recommendations for programmes. Eur J Cardiovasc Nurs. 2020;19(6):537–44.
Rooijakkers MJP, Li WWL, Wollersheim L, et al. Transcatheter aortic valve replacement during the COVID-19 pandemic: a Dutch single-center analysis. J Card Surg. 2021;36(1):48–55.
Vendrik J, de Boer J, Zwiers W, et al. Ongoing transcatheter aortic valve implantation (TAVI) practice amidst a global COVID-19 crisis: nurse-led analgesia for transfemoral TAVI. Neth Heart J. 2020;28(7–8):384–6.
NHR Handboeken & overige documenten. https://nederlandsehartregistratie.nl/handboeken/. Accessed 28 Apr 2022.
Wetenschappelijk beleid van de NHR. http://nederlandsehartregistratie.nl/wp-content/uploads/2022/01/NHR-wetenschappelijk-beleid_versie-6.0.pdf. Accessed 28 Apr 2022.
RIVM Coronadashboard. https://coronadashboard.rijksoverheid.nl/landelijk/positief-geteste-mensen. Accessed 28 Apr 2022.
Généreux P, Piazza N, Alu MC, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J. 2021;42(19):1825–57.
Adlam D, Chan N, Baron J, Kovac J. Aortic stenosis in the time of COVID-19: development and outcomes of a rapid turnaround TAVI service. Catheter Cardiovasc Interv. 2021;98(3):e478–82.
Valdebenito M, Massalha E, Barbash IM, et al. Transcatheter aortic valve implantation during the COVID-19 Pandemic. Am J Cardiol. 2021;145:97–101.
Thiele H, Kurz T, Feistritzer HJ, et al. General versus local anesthesia with conscious sedation in transcatheter aortic valve implantation: the randomized SOLVE-TAVI trial. Circulation. 2020;142(15):1437–47.
Feistritzer HJ, Kurz T, Stachel G, et al. Impact of anesthesia strategy and valve type on clinical outcomes after transcatheter aortic valve replacement. J Am Coll Cardiol. 2021;77(17):2204–15.
Perdoncin E, Greenbaum AB, Grubb KJ, et al. Safety of same-day discharge after uncomplicated, minimalist transcatheter aortic valve replacement in the COVID-19 era. Catheter Cardiovasc Interv. 2021;97(5):940–7.
NHR Rapportage 2021. https://nederlandsehartregistratie.nl/wp-content/uploads/2021/09/NHR-Rapportage-2021-090921.pdf. Accessed 28 Apr 2022.
WHO Coronavirus (COVID-19) dashboard. https://covid19.who.int/. Accessed 20 Apr 2022.
Denimal T, Delhaye C, Piérache A, et al. Feasibility and safety of transfemoral transcatheter aortic valve implantation performed with a percutaneous coronary intervention-like approach. Arch Cardiovasc Dis. 2021;114(8–9):537–49.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M.J.P. Rooijakkers, W.W.L. Li, N.A. Stens, M.M. Vis, P.A.L. Tonino, L. Timmers, N.M. Van Mieghem, P. den Heijer, S. Kats, P.R. Stella, V. Roolvink, H.W. van der Werf, M.G. Stoel, C.E. Schotborgh, G. Amoroso, F. Porta, F. van der Kley, M.H. van Wely, H. Gehlmann, L.A.F.M. van Garsse, G.S.C. Geuzebroek, M.W.A. Verkroost, J.M. Mourisse, N.M. Medendorp and N. van Royen declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rooijakkers, M.J.P., Li, W.W.L., Stens, N.A. et al. Transcatheter aortic valve implantation amid the COVID-19 pandemic: a nationwide analysis of the first COVID-19 wave in the Netherlands. Neth Heart J 30, 503–509 (2022). https://doi.org/10.1007/s12471-022-01704-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12471-022-01704-9