
Abstract
An early invasive strategy in patients who have acute coronary syndrome without ST-elevation (NSTE-ACS) can improve clinical outcome in high-risk subgroups. According to the current guidelines of the European Society of Cardiology (ESC), the majority of NSTE-ACS patients are classified as “high-risk”. We propose to prioritise patients with a global registry of acute coronary events (GRACE) risk score >140 over patients with isolated troponin rise or electrocardiographic changes and a GRACE risk score <140. We also acknowledge that same-day transfer for all patients at a high risk is not necessary in the Netherlands since the majority of Dutch cardiology departments are equipped with a catheterisation laboratory where diagnostic coronary angiography is routinely performed in NSTE-ACS patients. Therefore, same-day transfer should be restricted to true high-risk patients (in addition to those NSTE-ACS patients with very high-risk (VHR) criteria) in centres without coronary angiography capabilities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute coronary syndrome without ST-elevation (NSTE-ACS) represents a broad spectrum of diagnoses, ranging from unstable angina to myocardial infarction with considerable myocardial damage. A routine invasive strategy (coronary angiography within 24–72 h) has been shown to improve clinical outcomes when compared with a selectively invasive strategy (coronary angiography in case of refractory angina and/or inducible ischaemia by non-invasive stress testing [1]). Therefore, the 2015 European Society of Cardiology (ESC) NSTE-ACS guidelines and the 2018 ESC Myocardial revascularisation guidelines endorse an invasive strategy in moderate-risk to high-risk patients, while highlighting the role of risk stratification in the decision process [1, 2]. The timing of an invasive strategy should be based on individual patient risk factors, such as haemodynamic instability, refractory symptoms or clinical characteristics such as diabetes or renal failure (Fig. 1). The current ESC guidelines advise an immediate invasive strategy in patients with ‘very-high characteristics’, such as haemodynamic instability or refractory angina (Fig. 1). An early (<24 h) invasive strategy is recommended in patients with a global registry of acute coronary events (GRACE) risk score >140, dynamic ST-segment and T‑wave (ST-T) changes or a typical rise-and-fall in cardiac troponin. Moreover, the ESC guidelines recommend a “same-day transfer” to a centre for percutaneous coronary intervention (PCI) in these high-risk patients.
The current paper discusses the evidence and limitations of these recommendations for an early invasive strategy, as well as specific comments on the Dutch situation.

Selection of the 2015 ESC guidelines’ recommendations for invasive coronary angiography and revascularisation in NSTE-ACS. (aClass of recommendation, bLevel of evidence. NSTE-ACS non-ST-elevation acute coronary syndromes, MI myocardial infarction, GRACE global registry of acute coronary events, eGFR estimated glomerular filtration rate, LVEF left ventricular ejection fraction, PCI percutaneous coronary intervention, CABG coronary artery bypass grafting)
Background
The Timing of Intervention in Acute Coronary Syndromes (TIMACS) trial, which was published in 2009, was the largest trial thus far randomising a total of 3,031 patients to coronary angiography <24 h versus >36 h after randomisation [3]. The study was not able to demonstrate an overall benefit of an invasive strategy with regard to the primary composite endpoint of death, myocardial infarction or stroke at six months. However, in a prespecified analysis of high-risk patients with a GRACE risk score >140 (one third of patients), an early invasive strategy did confer a significant reduction of the primary endpoint (hazard ratio [HR] 0.65, confidence interval [CI] 0.48–0.89, p = 0.006). Other randomised controlled trials showed variable results and were not able to demonstrate a consistent benefit of an early invasive strategy [4,5,6,7,8,9].
Several subsequent meta-analyses have shown a benefit in terms of recurrent or refractory ischaemia and length of hospital stay associated with an early invasive strategy compared with a delayed invasive strategy [10,11,12]. Results of an early strategy on mortality and non-fatal myocardial infarction are less consistent in studies [10,11,12,13,14].
Li et al. conducted a systematic review and meta-analysis and found a significant reduction in both refractory ischaemia and mortality associated with early invasive strategy versus delayed invasive strategy, but no reduction in myocardial infarction [15]. Another meta-analysis of randomised controlled trials based on individual patient data by Jobs et al. did not demonstrate an overall mortality benefit associated with an early invasive strategy [16]. However, in a prespecified analysis in patients with elevated biomarkers at baseline, a mortality benefit was found. In addition, in subgroups of patients with diabetes, age >75 years and a GRACE risk score >140 a mortality benefit was observed, although tests for interaction were inconclusive. The effect observed in this meta-analysis was still largely driven by the results of the TIMACS trial, which, together with the ELISA‑3, made up 65% of all patients. Furthermore, this meta-analysis included a substantial proportion of ‘older’ studies (range 2000–2016), during which time frame substantial developments were achieved with respect to pharmacotherapy and the availability of high-sensitive troponin essays.
Very recently, the Very Early veRsus Deferred Invasive evaluation using Computerized Tomography (VERDICT) trial was published [17]. Patients with a clinical suspicion of NSTE-ACS were included, based on either new electrocardiographic (ECG) changes compatible with myocardial ischaemia, or positive cardiac troponin. The primary endpoint of all-cause death, non-fatal recurrent myocardial infarction, hospital admission for refractory myocardial ischaemia or hospital admission for heart failure did not differ between the early invasive group (coronary angiography with possible revascularisation <12 h) versus the delayed invasive group (angiography with possible revascularisation in 48–72 h). However, among patients with a GRACE risk score >140, a reduction of the primary endpoint was observed (HR 0.81, 95% CI 0.67–1.01, p-value for interaction = 0.023). This result is consistent with the TIMACS trial, however, it is not known which separate endpoint drove this outcome difference.
Data regarding possible sex differences in early invasive strategy are scarce. Several studies suggest that an early invasive strategy is beneficial in women with NSTE-ACS, but not in low-risk women (i.e. negative biomarkers) [18, 19]. However, another study suggested caution in extrapolating the results from men to women in the context of choosing a therapeutic strategy in ACS [20].
Recommendations
In general, an early invasive strategy in selected patients seems to result in better outcomes than a delayed invasive strategy. In selected high-risk subgroups, a mortality reduction is suggested. Therefore, it is vital to identify those patients at high risk who might benefit from such a strategy. Not surprisingly, clinical characteristics in the GRACE risk calculator such as cardiac arrest, signs of heart failure and haemodynamic instability have the largest impact.
The “high-risk” criteria as listed in the present ESC guidelines seem to overestimate the risk. Apart from a GRACE risk score >140, patients with isolated troponin rise or ST‑T changes classify as “high-risk” as well. Arguably, the risk of these latter two groups is lower than the risk of patients with a GRACE risk score >140. This is in part a result of the availability of more sensitive troponin tests, whereas most trials were performed before these high-sensitivity troponin assays became the clinical standard in Europe. It is not clear to what extent these highly sensitive assays might impact the applicability of the currently available study results, but it is possible that a substantial number of NSTE-ACS patients in current practice would previously have been classified as having unstable angina.
In our opinion, the strongest evidence for an early invasive strategy is in patients with a GRACE risk score >140. For patients with positive cardiac markers or ST‑T changes but with a GRACE risk score <140 (who comprise the majority of NSTE-ACS patients in contemporary practice) no compelling evidence exists that such patients should undergo coronary angiography within 24 h. Importantly, the VERDICT trial, which was a large trial including such patients with either positive biomarkers or ST‑T changes did not show an overall benefit of an invasive strategy. This study was published after the introduction of the 2015 and 2018 ESC guidelines.
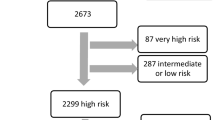
Importantly, as the current guidelines criteria identify the majority of contemporary NSTE-ACS as “high-risk”, there is a risk of losing sight of the true high-risk patients. This may lead to a policy of not prioritising the true high-risk patients undergoing invasive coronary angiography within 24 h. As it is key to identify the true high-risk patients and based on the available evidence, we recommend prioritising patients with a GRACE risk score >140 (including clinical parameters such as heart failure, arrest and haemodynamic instability) over patients with isolated positive troponin or isolated ST‑T changes.
Transfer to a PCI centre
The 2015 NSTE-ACS guidelines recommend a ‘same-day transfer’ to a PCI centre for high-risk patients based on the aforementioned criteria. For the Dutch situation, this is—in our opinion—not a necessity, as discussed before in a position paper by members of the Dutch Society for Cardiology Acute Coronary Syndrome working group [21, 22]. The evidence for an invasive strategy stems primarily from studies investigating the timing of coronary angiography—and not timing of revascularisation necessarily.
The Dutch situation is markedly different from that in many other European countries since the majority of Dutch cardiology departments are equipped with a catheterisation laboratory where diagnostic coronary angiography is routinely performed in NSTE-ACS patients. After diagnostic angiography, patients are discussed in a heart team and based on patient characteristics and coronary anatomy a prioritisation can be made for the transfer to an interventional centre for those suitable for PCI or coronary artery bypass grafting (CABG).
When coronary angiography is not available in the admitting centre or is not possible for other reasons, transfer within 24 h to a PCI centre may be considered. However, urgent (same-day) transfer should be restricted to high-risk patients with a GRACE risk score >140 or with very-high-risk criteria as mentioned in the ESC guidelines (Fig. 1). We advocate regional arrangements to be made between hospitals without 24/7 angiography capacities and local PCI centres.
Recommendations
-
Identification of high-risk NSTE-ACS patients is important and can improve outcomes if coronary angiography is performed within 24 h in order to determine an appropriate revascularisation strategy.
-
According to the current ESC guidelines, the majority of NSTE-ACS patients are classified as ‘high-risk’. Based on currently available evidence, we propose to prioritise patients with a GRACE risk score >140 over patients with isolated troponin rise or ECG changes and a GRACE risk score <140.
-
In centres without coronary angiography capabilities, same-day transfer to a PCI centre should be considered in true high risk patients with a GRACE risk score >140 or other unstable characteristics
References
Neumann F, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165.
Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267–315.
Metha SR, Granger CB, Boden WE. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360:2165–75.
van ’t Hof AW, de Vries ST, et al. A comparison of two invasive strategies in patients with non-ST elevation acute coronary syndromes: results of the Early or Late Intervention in unStable Angina (ELISA) pilot study. 2b/3a upstream therapy and acute coronary syndromes. Eur Heart J. 2003;24(15):1401–5.
Neumann F, Kastrati A, Pogatsa-Murray G, et al. Evaluation of prolonged antithrombotic pretreatment (“cooling-off” strategy) before intervention in patients with unstable coronary syndromes: a randomized controlled trial. J Am Med Assoc. 2003;290:1593–9.
Montalescot G, Cayla G, Collet J, et al. Immediate vs delayed intervention for acute coronary syndromes: a randomized clinical trial. J Am Med Assoc. 2009;302:947–54.
Badings EA, The SHK, Dambrink JE, et al. Early or late intervention in high-risk non-ST-elevation acute coronary syndromes: results of the ELISA‑3 trial. EuroIntervention. 2013;20(9):54–61.
Milosevic A, Vasiljevic-Pokrajcic Z, Milasinovic D, et al. Immediate Versus Delayed Invasive Intervention for Non-STEMI Patients: the RIDDLE-NSTEMI study. JACC Cardiovasc Interv. 2016;9:541–9.
de Winter RJ, Windhausen F, Cornel JH. Early invasive versus selectively invasive management for acute coronary syndromes. N Engl J Med. 2005;353:1095–104.
Katritsis DG, Siontis GCM, Kastrati A, et al. Optimal timing of coronary angiography and potential intervention in non-ST-elevation acute coronary syndromes. Eur Heart J. 2011;32:32–40.
Milasinovic D, Milosevic A, Marinkovic J, et al. Timing of invasive strategy in NSTE-ACS patients and effect on clinical outcomes: a systematic review and meta-analysis of randomized controlled trials. Atherosclerosis. 2015;241:48–54.
Bonello L, Laine M, Puymirat E, et al. Timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes and clinical outcomes: an updated meta-analysis. JACC Cardiovasc Interv. 2016;9:2267–76.
Navarese EP, Gurbel PA, Andreotti F, et al. Optimal timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes: a systematic review and meta-analysis. Ann Intern Med. 2013;158:261–70.
Rajpurohit N, Garg N, Garg R, et al. Early versus delayed percutaneous coronary intervention for patients with non-ST segment elevation acute coronary syndrome: a meta-analysis of randomized controlled clinical trials. Catheter Cardiovasc Interv. 2013;81:223–31.
Li Y, Zhang Z, Xiong X, et al. Immediate/early vs. delayed invasive strategy for patients with non-ST-segment elevation acute coronary syndromes: a systematic review and meta-analysis. Front Physiol. 2017;8:952.
Jobs A, Mehta SR, Montalescot G, et al. Optimal timing of an invasive strategy in patients with non-ST-elevation acute coronary syndrome: a meta-analysis of randomised trials. Lancet. 2017;390:737–46.
Kofoed KF, Kelbæk H, Hansen PR, et al. Early versus standard care invasive examination and treatment of patients with non-ST-segment elevation acute coronary syndrome. Circulation. 2018;138:2741–50.
O’Donoghue M, Boden WE, Braunwald E, et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction: a meta-analysis. J Am Med Assoc. 2008;300:71–80.
Elgendy IY, Mahmoud AN, Mansoor H, Bavry AA. Early invasive versus initial conservative strategies for women with non-ST-elevation acute coronary syndromes: a nationwide analysis. Am J Med. 2017;130:1059–67.
Cenko E, Ricci B, Kedev S, et al. Invasive versus conservative strategy in acute coronary syndromes: the paradox in women’s outcomes. Int J Cardiol. 2016;222:1110–5.
Damman P, van ’t Hof AW, Ten Berg JM, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: comments from the Dutch ACS working group. Neth Heart J. 2017;25:181–5.
Arslan F, Voskuil M. The management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: early invasive strategy for all? Neth Heart J. 2017;25:170–2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J.W. Jukema/his department has received research grants from and/or was speaker (with or without lecture fees) at meetings, including CME accredited meetings, sponsored by Amgen, Astra-Zeneca, Biotronik, Boston Scientific, Daiichi Sankyo, Lilly, Medtronic, Merck-Schering-Plough, Pfizer, Sanofi Aventis, The Medicine Company, the Netherlands Heart Foundation, CardioVascular Research the Netherlands (CVON), the Interuniversity Cardiology Institute of the Netherlands and the European Community Framework KP7 Programme. B. Zwart, J.M. ten Berg, A.W. van ’t Hof, P.A.L. Tonino, Y. Appelman, A.H. Liem, F. Arslan, J. Waltenberger, R.J. de Winter and P. Damman declare that they have no competing interests.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Zwart, B., ten Berg, J.M., van ’t Hof, A.W. et al. Indications for an early invasive strategy in NSTE-ACS patients. Neth Heart J 28, 131–135 (2020). https://doi.org/10.1007/s12471-019-01337-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12471-019-01337-5