
Abstract
During the COVID-19 pandemic, schools rapidly changed from in-class instruction to remote learning. Parent involvement and management of the home learning situation was greatly emphasized, and this presented challenges and opportunities for parents of children with attention-deficit/hyperactivity disorder (ADHD). There was an urgent need for effective parent support in the home learning situation, particularly for parents of youth with ADHD. The current study implemented a behavioral parent training (BPT) program, an evidence-based intervention for childhood ADHD, modified to target home learning and be delivered via telehealth. The intervention was evaluated in a multiple baseline trial across families of youth with ADHD (n = 3). The primary outcome was daily, parent-reported academic engagement during home learning. Parents also completed daily ratings of their child’s respectful and disruptive behavior, and remote, home observations of academic tasks were recorded at baseline and post-treatment. Based on visual analysis of baseline, treatment and post-treatment daily ratings, two of the three participants had a positive response to treatment indicated by improved academic engagement. These findings provide preliminary support for the home-learning, telehealth-delivered BPT program in supporting families during the COVID pandemic.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The coronavirus pandemic (COVID-19) significantly and abruptly altered daily life, and the effects on youth, especially those with mental health and academic difficulties, are of particular concern. Community-level virus mitigation efforts such as quarantining, school closures, and social distancing, despite clear public health benefits and rationale, can have negative effects on families via reduced social support, limited educational opportunities, and increased overall stress (Larsen et al., 2021). Students with neurodevelopmental disorders, such as attention-deficit hyperactivity disorder (ADHD), may be particularly vulnerable to the negative effects of school closures. ADHD is the most common mental health disorder among elementary-age children with a prevalence rate of about 9% in the USA (Danielson et al., 2018). Children with ADHD have multifaceted, persistent difficulty with academics throughout development, and are at higher risk of high school drop-out than peers (Barkley et al., 2006; Kuriyan et al., 2013).
In the context of COVID-19, there is ample reason to be concerned about the academic engagement and performance of children with ADHD during home learning and hybrid schooling. Children with ADHD perform best in structured settings with clear routines and behavioral supports (Fabiano et al., 2007). Home learning is inherently less structured than going to a school building each day, following a prespecified and teacher-directed schedule of classes, participating in planned breaks such as recess, and following this daily routine with a consistent group of classmates. Further, the time management, planning, and organizational skills required for independent, home learning success in the face of the multitude of distractors at home are the very same skills that students with ADHD are known to struggle with (Booster et al., 2012; Langberg et al., 2013). In fact, many children with ADHD have experienced increased inattentive and hyperactive/impulsive symptom severity during pandemic lockdowns (Melegari et al., 2021; Shah et al., 2021; Wendel et al., 2020).
The evidence is not yet clear regarding the effects of school closures on the academic learning of elementary students and those with ADHD. Overall, elementary students had attenuated growth in mathematics and similar growth in reading in fall 2020 compared to the previous year (Kuhfeld et al., 2020). Authors caution, however, that learning loss may be underestimated as students with lower achievement scores in prior assessment points were more likely to be missing fall 2020 achievement data. Among elementary-age children with ADHD, differences in achievement growth were not found between a clinical cohort that experienced 3–4 months of home learning (2019–2020 cohort) compared to the cohort prior to COVID-19 (2018–2019; Lupas et al., 2021).
A key consideration and likely source of inter-student variability in remote learning/home learning success is parent management of daily academic engagement. Parents were burdened by the need to be more involved with remote learning (Misirli & Ergulec, 2021), and parents of students who required additional educational supports for the provision of learning were unlikely to have the capacity to help their child to the same degree as a skilled general or special education teacher (Joline et al., 2020; Masonbrink & Hurley, 2020). Parents of children with ADHD report significantly more difficulty with keeping their child engaged and on-task during home learning compared to parents of children without ADHD (Roy et al., 2022). Research has indicated that the lack of consistent routines during the COVID-19 school closures relates to increased difficulty with remote learning for individuals with ADHD (Becker et al., 2020). Parents of children with ADHD have also reported changes in their parenting such as increased irritability and yelling (Shah et al., 2021) during the pandemic.
Parents of children with ADHD are more in need of support than ever, and treatments should target the primary, immediate concerns of managing home learning and enhancing caregiver well-being to promote child academic engagement. Behavioral parent training (BPT), in which parents learn positive behavior support strategies and prudent behavioral consequence strategies, is an evidence-based treatment for ADHD that has been shown to improve parenting skills and child behavior (Evans et al., 2018; Fabiano et al., 2021; Pelham & Fabiano, 2008). BPT modified to target home learning via parent management of academics may be critical to alleviate the increased impairment among children with ADHD and to improve family functioning during COVID-19. Fortunately, BPT has been successfully adapted to target homework, a time-limited form of home learning, via incorporation of homework-management specific techniques in the Family School Success Program (Power et al., 2001). This program includes sessions focused on structuring the homework routine, setting homework goals, and providing reinforcement contingent on academic engagement during homework time. This program has been shown to improve homework performance (Merrill et al., 2017) and reduce homework problems (Power et al., 2012) among children with ADHD in controlled trials.
In addition to substantially increasing the parents’ role in education, the pandemic also necessitates telehealth-delivery when feasible. BPT has been successfully delivered via telehealth for families of children with ADHD with comparable efficacy to in-person treatment (DuPaul et al., 2018; Xie et al., 2013). We aim to combine academic-focused BPT with telehealth-delivery to meet the needs of families of children with ADHD during the pandemic. Results will inform future work to support parents of children with ADHD more broadly as remote schooling has continued sporadically due to quarantines (Cray & Ome, 2021), some parents home school their children, and families may have difficulty managing homework in an increasingly online world (managing multiple logins, message boards, and academic tools). This work will also be useful to therapists, school counselors, and other mental health providers supporting families who are often concerned about their child’s academic performance and behavior across school and home settings. Positive behavioral supports applied across settings can be the most beneficial for children (Fabiano et al., 2021; Smith et al., 2020). As children have returned to in-person learning, the current study may provide information about appropriate services to improve at-home behavioral supports and family-school partnership.
The current study is a multiple baseline trial examining the effects of home learning-focused BPT for parents of children with ADHD on child academic engagement or on-task behavior. Evidence-based BPT protocols targeting homework performance were modified (Merrill et al., 2017; Power et al., 2012) to accommodate telehealth delivery and address difficulties unique to home learning. Therapists provided the intervention individually via Zoom. Treatment included 7–10 sessions, and parent ratings of child academic engagement and behavior during home learning were provided daily. We hypothesized that home learning BPT would lead to improved child behavior during home learning captured via visual analysis of the level, variability, immediacy, and trend of academic engagement from the baseline to treatment phases with continued beneficial effects from the treatment to post-treatment phases. We also explored effects of the intervention on pre-post changes in observed parenting behavior, observed child behavior, and parent- and teacher-reported impairment. We expected that parent praise would increase, negative talk would decrease, and child compliance would increase from baseline to post-treatment.
Method
Participants
Participants were recruited from a clinic list of families interested in services for their children with ADHD. All study procedures were approved by the governing Institutional Review Board (IRB). Inclusion criteria were (1) a DSM-5ADHD diagnosis, (2) currently in kindergarten through 5th grade, and 3) currently home learning at least one day per week. Diagnoses were established following recommended methods of combining parent and teacher ratings of ADHD, oppositional defiant disorder (ODD), and conduct disorder (CD) symptoms (disruptive behavior disorders rating scale [DBD; Pelham et al., 1992]) and impairment (IRS; Fabiano et al., 2006) and semi-structured parent clinical interview (Pelham et al., 2005; Massetti et al., 2003). Exclusion criteria were (1) meeting criteria for autism spectrum disorder severity level 2 or 3 based on clinical interview and (2) IQ below 70 measured by Wechsler Abbreviated Scale of Intelligence-Second Edition (Wechsler, 2011). Other diagnoses were not assessed. Five families completed the phone screen, and all five parent–child dyads completed IRB-approved consent and assent documents. Of those families, two completed baseline measures and daily measures during the baseline period but dropped out prior to treatment. For one family, the child (9-year-old, White, non-Hispanic/Latinx male) was starting in-person schooling, and the parent-reported feeling too overwhelmed due to increased work demands. The other family (8-year-old, White, non-Hispanic-Latinx female) did not provide a rationale for discontinuing prior to treatment. We therefore present information on the remaining three participants.
Participant 1
‘Alex,’ was a 9-year-old, White, non-Hispanic/Latinx male in the 4th grade with IQ and achievement scores in the average range. He met diagnostic criteria for ADHD, predominately inattentive presentation and was not receiving psychoactive medication during this study. Alex was home learning five days per week, and his mother was primarily responsible for managing home learning. At baseline, his mother reported that he was experiencing clinically significant impairment during home learning, e.g., “His academic progress has been impacted greatly. He’s distracted and his work is falling behind which leads to a lot of fighting with us.” Alex’s mother was 39 years old and did not have a job outside of the home. His parents were married, and their highest education was a graduate degree. Alex had a 7-year-old sister who was also learning at home. Author BMM provided treatment.
Participant 2
‘Sophia,’ was a 9-year-old White, non-Hispanic/Latinx female in 4th grade with an IQ in the superior range. Her achievement scores in Spelling and Word Reading were in the above average range, and her Numerical Operations achievement score was in the average range. She met criteria for ADHDFootnote 1, combined presentation, and ODD. She was not receiving psychoactive medication during this study. Sophia was home learning two to three days per week, and her mother was primarily responsible for home learning. Her mother reported significant problems with home learning, noting “She does not like to do her work at home. She argues constantly with me. She will forget to write assignments down in her agenda and then later will not remember what to do.” Sophia’s mother was 44 and was employed working from home. Sophia’s parents were living together, and their highest education was a bachelor’s degree. Sophia had one 13-year-old sister. Author WJM provided treatment.
Participant 3
‘Olivia,’ was a 7-year-old, White, non-Hispanic/Latinx female in 3rd grade. Her IQ was in the average range. Her Numerical Operations achievement score was in the average range and her achievement scores in Spelling and Word Reading were in the below average range. She met diagnostic criteria for ADHD, combined presentation and was not receiving psychoactive medication. Olivia was home learning five days per week, and her mother was primarily responsible for managing home learning. Olivia’s mother reported clinically significant impairment during home learning, noting that Olivia “…does not seem to be able to function independently in relation to school. She is disorganized, unmotivated, unable to sustain attention… [which] leads to outbursts, physical lashing out, crying, frustration, and negative self-image.” Olivia’s mother was 43, was not employed outside of the home, and had volunteer commitments. Olivia’s parents were living together, and their highest education was a graduate degree. Olivia had a 7-year-old sister who was home learning and a 4-year-old brother at home. Author BMM provided treatment.
Setting
The current study takes place within the context of New York State COVID-19 mitigation efforts. This included school closures and immediate modification to remote instruction for all grades in March 2020. During the summer of 2020, the New York State Department of Health determined that six-feet of physical distancing would be required for all classrooms, resulting in an immediate determination among school districts that a remote or hybrid remote return to school in the fall of 2020 would be necessary, as typical classroom space precluded all students and educators being in the room with the six-feet distancing requirement. Thus, the students included in the study were in districts that utilized a hybrid instruction approach of in-school attendance within a reduced class size for some of the school days and home instruction for the alternate days (Sophia) or all remote instruction (Alex, Olivia). This study took place from November 2020 to March 2021.
Procedures
The current study utilized a multiple baseline design across subjects to examine the impact of home learning-focused BPT on child behavior and academic engagement during home learning. All study procedures were completed via telehealth, electronic surveys, or survey-link text messaging via Twilio and REDCap hosted at Florida International University (Harris et al., 2019). Families completed rating scales and recorded parent–child interaction observations prior to the baseline phase and after treatment. The direct behavior rating (DBR; discussed below) was sent to parents via text one to three times daily on home learning days based on the home learning schedule for each family. Home learning could include online classes, online class work, or worksheets/reading assignments that the teacher assigned to be completed during a typical school day (in other words, not assigned as traditional homework). For the rating to be sent, children had to have been scheduled for continuous home learning for the previous 60 min. Together with the parent, study investigators determined the best time to send ratings at least once and up to three times on home learning days. The stability of the DBR daily averages for each participant was examined during the baseline phase. The BPT program was initiated for each family when their baseline data demonstrated a stable, impaired trend or a linear, worsening trend. A stable trend was defined as at least three consecutive data points within 10 points of each other. Following BPT, DBRs were collected daily for 6 days to allow for comparison between baseline and post-treatment functioning. This study meets What Works Clearinghouse standards without reservations due to having three participants complete the two study phases, at least five data points per phase, and adequate reliability on repeated daily measures (Kratochwill et al., 2010).
Behavioral Parent Training for Home Learning
The BPT program consisted of 7–10 sessions based on the Family School Success Program (FSS; Power et al., 2001, 2012) parent sessions and general BPT content (Chronis-Tuscano et al., 2021). See Table 1 for session topics and sessions attended by each parent. The program included a focus on positive reinforcement, antecedent controls (routines, clear expectations), setting small academic engagement and behavioral goals during the learning period, and providing access to preferred activities contingent upon meeting goals (i.e., completing school work). FSS includes sessions targeting parent management of homework time that were modified to address home learning. The following specific modifications were made: 1) psychoeducation included information about ADHD and potential home learning problems, 2) the homework routine was expanded to include the entire home learning day, 3) instead of a ‘homework kit,’ families were encouraged to develop a ‘home learning kit’ that included their online learning usernames and passwords and other necessary materials, and 4) behavioral examples provided to illustrate concepts were focused on home learning whenever feasible. Lastly, an optional session focused on parent stress and coping (Chronis-Tuscano et al., 2021) was offered due to the unprecedented stress associated with a global pandemic and abrupt transition to home learning. This session focused on problem-solving to increase the use of social support, behavioral activation, and other coping strategies. Parents attended individual sessions with a Ph.D. level psychology trainee (BMM or WJM) under the supervision of a licensed clinical psychologist.
Measures
Daily Ratings
The direct behavior rating (DBR) measures Academic Engagement, Disruptive Behavior, and Respectful Behavior on 0–100 scale indicating the percent of time the child exhibited the behavior in the previous 60 min (see https://dbr.education.uconn.edu). Academic engagement was defined as “actively or passively participating in the class activity. For example: writing, raising his/her hand, answering a question, talking about a lesson, listening to the teacher/parent, reading silently, or looking at instructional materials." Disruptive behavior was defined as “student action that interrupts regular school or learning activity. For example: out of seat, fidgeting, playing with objects, acting aggressively, talking/yelling about things that are unrelated to instruction/ home learning.” Respectful behavior was defined as “compliant and polite behavior in response to adult direction and/or interactions with peers and adults. For example: follows teacher or parent direction, positive response to adult request, verbal or physical disruption without a negative tone/connotation.” These definitions were discussed with parents during enrollment and provided on the electronic DBR form each time it was completed. The DBR is generalizable across settings, raters, and activities and has been used to monitor progress in intervention research and multiple baseline studies (Chafouleas et al., 2009; Christ et al., 2009, 2010; Fabiano et al., 2017). There is considerable psychometric support for the reliability and validity of DBR as an assessment tool (Briesch et al., 2010; Christ et al., 2010; Miller et al., 2018; Riley-Tillman et al., 2010).
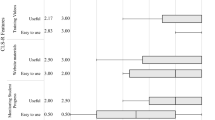
Participating parents completed the DBR one to three times daily on days that the child was home learning, and daily DBR averages are reported (Fig. 1). DBRs were collected during the baseline phase, treatment phase, and post-treatment phase. DBRs were sent at pre-specified, individualized times for each family based on the child’s home learning schedule to maximize consistency.

Multiple baseline graph of parent-report direct behavior ratings (DBR) of Academic Engagement on home learning days. Parents completed the DBR one to three times daily on home learning days only, and averages on each home learning day are shown. Alex’s parent completed an average of 1.77 DBRs per home learning day (mode = 2), Sophia’s parent completed an average 2.68 per day (mode = 3), and Olivia’s parent completed an average of 2.44 DBRs per day (mode = 3). A graph by date can be found in supplemental materials
To assess reliability, parents also completed the DBR modified to assess the observation period (i.e., 15 min instead of 60 min) following structured observations (see description of parent–child observations below). Two masked observers completed the same, time-modified DBR after viewing recorded observations, and reliability between observers and parents was examined using two-way, mixed effects intraclass correlation coefficients (ICC) where ICCs between 0.5 and 0.75 indicate moderate reliability and ICCs above 0.75 indicate good reliability (Koo & Li, 2016). Based on the DBR ratings from recorded parent–child interactions at pre- and post-treatment, DBR items had moderate to good reliability between parents and observers (academically engaged, ICC = 0.75; respectful, ICC = 0.72; disruptive, ICC = 0.86).
Parent–Child Observed Interactions
Prior to the baseline phase and after treatment, parents and children completed a video-recorded, 15-min observation of an academic activity in which the child writes a story with the parent’s assistance. Parents were instructed to make sure the story was written neatly and in complete sentences as if it were being turned in for an assignment. Video-taped interactions were coded by two trained, masked observers (each had a bachelor’s degree) using the Dyadic Parent Child Interaction Coding System- 3rd edition (DPICS-III; Eyberg & Robinson, 1983; Eyberg, et al., 2009). The DPICS is an observational system used to measure child behavior (e.g., noncompliance) and parent behavior (e.g., commands, praise). Assessments of inter-observer reliability indicated acceptable agreement (mean r’s of 0.91 and 0.92 for the parent and child coding categories, respectively; Eyberg, et al., 1994). The DPICS has been used as an outcome in multiple studies of parent training and has demonstrated sensitivity to measuring outcomes for elementary school-aged children (Chronis-Tuscano et al., 2008, 2010; Danforth et al., 1991).
Coded variables of interest include child compliance and noncompliance and parent commands (indirect commands + direct commands), negative talk, and praise (labeled praise + unlabeled praise). Percent compliance was calculated by dividing compliance by opportunities for compliance (i.e., compliance + noncompliance). One-way, random effects ICCs indicated good reliability for negative talk (ICC = 0.86), praise (ICC = 0.90), compliance (ICC = 0.87), and noncompliance (ICC = 0.96) and moderate reliability for commands (ICC = 0.73). Observers also completed the DBR and an overall item measuring parental warmth and responsiveness from 0% (poor) to 100% (great) during the observation period. One-way, random effects ICCs indicated moderate to good reliability between observers for DBR items (academically engaged ICC = 0.72; respectful ICC = 0.83; disruptive ICC = 0.92) and parental warmth (ICC = 0.89). Due to high ICCs and full double coding, outcomes were averaged across observers. Reliability between observers and parents is reported above.
Parent and Teacher Report
The Impairment Rating Scale (IRS; Fabiano et al., 2006) asks parents and teachers to rate the severity of the child’s problems and need for treatment and/or special services in important functional domains (i.e., relationship with peers, relationship with the teacher(s), academic progress, classroom functioning, self-esteem, overall). Scores on the measure range from zero (Not a problem/Definitely does not need treatment or special services) to six (Extreme problem/ Definitely needs treatment or special services) with scores of 3 or greater indicating clinically meaningful impairment in a domain. Test–retest reliability estimates range from 0.60-0.89 over a period of six months (Fabiano et al., 2006). Ratings on the IRS predict mental health or school services, and there is evidence of convergent and discriminant validity on the measure (Fabiano et al., 2006). An item measuring impairment during home learning was added to the parent IRS for the current study (“How your child’s problems affect his or her academic progress during home learning”), resulting in 8 parent-report items and 7 teacher-report items. Parents and teachers completed the IRS at baseline and post-intervention. Parents completed the Therapy Attitude Inventory (TAI; Brestan et al., 1999) after treatment. The TAI is a 10-item scale measure satisfaction with the treatment outcomes and treatment process. Items are rated on a 1 to 5 scale with lower numbers indicating dissatisfaction or negative outcomes and higher numbers indicating satisfaction and positive outcomes. Scores are added together with a minimum of 10 and a maximum of 50. The TAI has excellent reliability and has been shown to relate to changes in observed and reported child behavior after BPT (Brestan et al., 1999).
Planned Analyses
Visual analysis was first conducted to evaluate level, immediacy, variability, trend and overlap in baseline, treatment, and post-treatment data for each participant. Tau-U was evaluated to detect effects in this single case design study (via online calculator; Vannest et al., 2016). Tau-U is a nonparametric correlation statistic that summarizes within-phase and between-phase trends in small sample sizes and provides a metric of non-overlap between the baseline phase and post-treatment phase, controlling for significant baseline trends when present. Tau-U has been shown to relate to expert visual analysis of multiple baseline graphs (Wolfe et al., 2019).
Results
Treatment Adherence, Fidelity, and Acceptability
Average session length was 51.84 min (SD = 9.74 min). Audio-recorded sessions were coded for fidelity to session content with 94% of planned content being discussed in each session and minimal variability across therapists or participants (BMM 94.45%, WJM 94.30% fidelity). All parents completed treatment and Olivia’s parent opted for the optional session focused on parent stress (see Table 1). Alex’s parent completed treatment in seven weeks, Sophia’s in twelve weeks, and Olivia’s in ten weeks. Alex and Olivia’s treatment length aligns with the number of sessions they had (Table 1). Sophia’s mother did not have treatment sessions during the two winter holiday breaks that occurred during participation, slightly lengthening their time in treatment. Sophia’s and Alex’s parents completed the TAI. Alex’s mother reported high overall satisfaction with a score of 44. Sophia’s mother reported neutral satisfaction with a total score of 30. Due to personal stressors, Olivia’s mother did not complete the TAI after treatment.
Daily Ratings
Following guidelines for visual analysis, the level, immediacy, variability, trend, and overlap of the treatment effect was evaluated (Fig. 1) for the primary study outcome of child academic engagement across phase changes between baseline, treatment, and post-treatment phases. As the intervention directly targets parents as agents of change, we did not expect immediate changes in child behavior after the first session of treatment. Relatedly, we did not expect an immediate deterioration of effects between the treatment and post-treatment phases. We briefly review effects of the intervention on secondary outcomes of disruptive and respectful behavior. See supplemental materials for disruptive and respectful behavior graphs.
Alex had the most pronounced and consistent positive response to treatment. During the baseline phase, his academic engagement fell below 80% three times and his overall behavior appeared to be worsening. During treatment, his academic engagement increased to 96% on average and there was 77% non-overlap between baseline and treatment phase academic engagement. Given the worsening trend during baseline, this change is very likely due to the intervention. Variability decreased from the baseline phase (SD = 13.77) to the treatment phase (SD = 10.13) and post-treatment phase (SD = 0). During post-treatment, his parent reported that he was academically engaged and respectful 100% of the time indicating a clear change in level and variability of academic engagement. As indicated by the effect sizes in Table 2, Alex had a significant, positive response to treatment that continued through the post-treatment phase (Tau = 0.82–1.0). The positive effect of treatment on all daily outcomes was immediate, and there was 100% non-overlap between baseline and post-treatment academic engagement. Masked coders similarly rated Alex as 100% academically engaged, 99.5% respectful, and 0% disruptive during the post-treatment observation compared to pre-treatment ratings of 55.5% academically engaged, 69% respectful, and 35.5% disruptive.
Sophia did not appear to respond to the intervention in terms of academic engagement. At baseline, Sophia had low academic engagement—an average of 30% with below 40% engagement almost every day. During the treatment phase, she was academically engaged an average of 39% of the time with marginal non-overlap between baseline and treatment phases (42% non-overlap). From the baseline phase to treatment phase, there was no clear immediate beneficial effect or change in level or trend. Sophia’s academic engagement during treatment was more variable (SD = 18.54) than her engagement variability during baseline (SD = 10.31) and post-treatment (SD = 9.27). After treatment, Sophia’s data show no days above 40% academic engagement indicating no change in level of academic engagement, no evidence of an immediate effect, and no non-overlapping data. Her trend of academic engagement at baseline was stable and, at post-treatment, appears largely stable with possible linear improvement from day 17 to day 24. There was not a significant, positive effect of treatment on academic engagement for Sophia (Tau = -0.19 to 0.32, Table 2). Sophia’s disruptive behavior continued to be variable throughout each phase, though she did not have any highly disruptive home learning days during post-treatment treatment compared to about one third of days above 60% disruptive throughout the baseline and treatment phases, indicating some benefit after treatment. Sophia’s average percentage of respectful behavior was 79% during baseline, 81% during treatment, and 69% during the post-treatment phase indicating no benefit.
Olivia presented with variable home learning behavior during the baseline phase and overall positive effects of treatment. Her average academic engagement was 58% at baseline compared to 83% during treatment and 85% during post-treatment indicating an immediate change in level. Her trend at baseline was stable, and as such the change in level of academic engagement is likely due to the intervention. Further, 78.5% and 83.33% of the treatment and post-treatment data, respectively, were non-overlapping with baseline. Olivia’s academic engagement varied between 37 and 77% at baseline (SD = 12.54), between 53 and 97% during treatment (SD = 11.23), and between 46 and 97% at post-treatment (SD = 19.61). This indicates initial stability followed by an increase in variability during the post-treatment phase counter to hypotheses. However, this was due to an outlier during post-treatment in which the family had a medical emergency. Without that outlier, Olivia’s variability in academic engagement improved markedly from baseline (SD = 12.54) to post-treatment (SD = 5.37). Treatment had a significant, positive effect on Olivia’s academic engagement (Tau = 0.72 – 0.88, Table 2). Olivia’s disruptive behavior was below 20% on 7 of 12 baseline days though there were notable spikes in disruptive behavior during baseline. Her respectful behavior followed a similar pattern with only one day below 60% respectful during baseline. During treatment, her parent reported consistently positive behavior with only two days reported as more than 20% disruptive and four days reported as less than 80% respectful. Post-treatment, Olivia had only one day with substantial negative behavior during home learning (outlier discussed above). All other post-treatment days, she had above 80% respectful behavior and less than 20% disruptive behavior. Overall, Olivia responded positively to treatment.
Positive effects of treatment were found for Alex and Olivia. The immediacy of change in academic engagement is evidence that results are related to the implementation of treatment. Alex was first assigned to treatment, and his improved academic engagement is in direct contrast to Olivia and Sophia’s comparatively low academic engagement in the baseline phase. The combined Tau-U non-overlap statistic indicates a significant, positive effect of BPT on the primary outcome of interest—academic engagement—across subjects (Tau-U = 0.69, see Table 2). Overall, average academic engagement improved from baseline to treatment and from baseline to post-treatment. There was a significant decrease in average disruptive behavior from baseline to post-treatment. There was not a significant effect of treatment on respectful behavior. Average respectful behavior during the baseline period was 82%, 79%, and 78% for Alex, Sophia, and Olivia, respectively, indicating a possible ceiling effect.
Parent–Child Observed Interactions
See Table 3 for all observed outcome variables by participant. Olivia’s mother increased her use of praise. Praise did not change for Alex’s or Sophia’s parents. Notably, parent negative statements decreased substantially from an average of 3 negative statements in the 15-min baseline observation to only one instance coded across the three participants at post-treatment. Parents issued fewer commands at post-treatment compared to baseline, and children were more likely to comply with a compliance rate of about 63% at baseline and about 99% at post-treatment—though Olivia’s compliance was high at baseline and post treatment (97% and 100%, respectively). Masked observers indicated clear improvements in child academic engagement, respectful behavior, and disruptive behavior on the DBR as well as increased parental warmth and responsiveness across participants.
Parent and Teacher Report
The parent-report IRS measures impairment in the following domains: home learning, social functioning, relationship with sibling(s), relationship with parent, academic progress, self-esteem, family functioning, and overall. The teacher IRS measures impairment in the following domains: home learning, social functioning, relationship with teacher, academic progress, classroom functioning, self-esteem, and overall. At baseline, Alex was reported to be impaired (defined by score of 3 or greater) in all domains except relationship with sibling on parent report. He continued to be impaired according to his parent across domains at post-treatment. Conversely, his teacher reported impairment in academic progress, classroom functioning, self-esteem, and overall functioning at baseline that resolved to subclinical at post-treatment.
At baseline, Sophia’s parent reported that she was impaired in home learning, sibling relationship, parent relationship, and overall functioning. At post-treatment, she remained in the impaired range for these domains. Sophia’s teacher reported no impairment on the IRS at baseline or post-treatment.
At baseline, Olivia’s parent reported impairment across domains apart from social functioning and relationship with sibling(s). After treatment, her parent reported that family functioning and relationship with parent had improved and were no longer clinically impaired. Further, home learning impairment reduced from 5 to 3, which is the cut-off for clinical impairment. Olivia’s teacher reported impairment across all domains at baseline and continued impairment across domains at post-treatment.
Discussion
There have been a multitude of challenges related to the COVID-19 pandemic and mitigation efforts for parents and families. Parents of children with mental health difficulties, such as ADHD, or who require extra support in school settings were under particular strain as they support their child’s home learning. To meet this need and evaluate initial efficacy of a modified treatment approach, we conducted a multiple baseline trial of home learning-focused BPT which extends previous work on homework-focused BPT (Merrill et al., 2017; Power et al., 2012). Treatment was delivered via telehealth and modified to address home learning and parent stress as needed. Daily ratings of child academic engagement and behavior during home learning were collected, and academic engagement was targeted as the primary outcome. Of the three families in the trial, two had a clear, positive response to BPT providing some evidence that BPT was successfully modified to address emergent needs of families Potential reasons for differing effects are discussed below. We were not able to demonstrate a functional relation between home learning-focused BPT and improved academic engagement as results were only replicated for two of the three cases. Based on structured observations, parent behavior and child compliance improved from baseline to post-treatment.
Improvements in daily home learning behavior and engagement were particularly evident for two of the three participants. Alex’s improvement was the most consistent with an average of 96% for academic engagement during the treatment phase—which translates to 77% non-overlap between baseline and treatment phase academic engagement. In fact, daily post-treatment ratings indicated he was 100% engaged, 100% respectful, and 0% disruptive during the hours sampled. Though this appears unusually good, in fact perfect, these ratings do align with the structured observation at post-treatment in which the child was rated by masked observers as being 100% academically engaged, 99.5% respectful, and 0% disruptive. Alex’s mother appeared to apply what was learned in treatment immediately and effectively, and Alex’s academic engagement was significantly improved (Table 2).
Olivia’s response to treatment was significant and positive (Table 2), though her daily engagement and behavior were much more variable than Alex’s. Her academic engagement improved from an average of 58% at baseline to 83% and 85% during the treatment and post-treatment phases. She had one difficult day during the post-treatment phase, but otherwise had above 80% academic engagement and respectful behavior and below 20% disruptive behavior each day during home learning at post-treatment.
Sophia did not appear to respond to the intervention based on daily ratings of academic engagement during home learning resulting in a non-significant effect (Table 2). Sophia met criteria for ADHD, combined presentation, and ODD. Her IQ was in the superior range, and she also had high achievement scores in word reading and spelling. These factors may make her a unique case given that she was struggling with home learning and academics despite her superior intelligence. Comparatively, Alex and Olivia had average IQ scores and did not meet criteria for ODD. The skills taught in home learning-focused BPT overlap with those taught in BPT for oppositional behavior. However, it remains possible that brief treatment was insufficient to address Sophia’s difficulties or that insufficient attention was paid to addressing her argumentative and oppositional behaviors in the current treatment. Further, it is possible that focusing on home learning and parental academic management diluted BPT’s focus on oppositional behavior and was not appropriately targeted toward Sophia’s presenting problems at home. In fact, her mother reported that treatment “seemed to help with getting her to do her schoolwork, but her behavior in the house (defiance, picking fights) has stayed the same or worsened.” On the other hand, Sophia’s compliance increased from 52% at baseline to 97% at post-treatment. Lastly, Sophia was in a hybrid learning setting, whereas Alex and Olivia were in fully remote learning. This could have affected parent motivation, and the rapidly changing routine and demands between settings could have made home learning more difficult for Sophia and her mother as inconsistent routines are particularly difficult for children with externalizing problems (Harris et al., 2014). More research is needed on the differential impact of hybrid learning, remote learning, and in-person schooling on the behavior of youth with ADHD.
During structured observations conducted at baseline and post-treatment, parent/child dyads completed a short writing assignment. Though the current multiple baseline study is not powered to statistically compare means on variables that are measured infrequently (i.e., only at assessment points), we display participant-level data in Table 3. It is clear from observed parent behavior that parents learned to criticize their children less and were observed to be warmer and more responsive at post-treatment. At baseline, children were compliant with parental commands around 50% of the time except for Olivia who was compliant 97% of the time. After treatment, children were compliant with approximately 100% of parent requests. It is clear from these data that children were learning how to respond to and comply with adult requests. This can be a meaningful difference when academic work is limited to an hour a day, and during home learning, compliance improving to that magnitude could greatly impact the family’s overall functioning. Similar results were found for engagement and behavior during the academic task on the observer-completed DBR. Results also support the use of multi-method assessment to examine change in parent and child behavior (Fabiano et al., 2017) as the observations complemented daily ratings and provided an objective metric of child behavior. Cumulatively, parents learned how to support their children’s academic engagement during home learning.
Despite promising results on daily and observational measures, impairment continued for each child according to either parent or teacher report. Alex’s teacher reported clinical improvement after treatment whereas his mother reported that he remained impaired in most areas (e.g., home learning, academic progress, family functioning). Conversely, Olivia’s mother reported clinical improvement in some areas—with overall family functioning and relationship with parent improving to the subclinical range—while her teacher reported continued impairment across domains. Sophia’s mother did not report clinical improvement, which is unsurprising.
As results were replicated across two participants, we are not able to demonstrate a clear functional relation between the treatment and positive outcomes which requires three replications. However, results do provide some support for the salutary effects of telehealth-delivered behavioral treatment, consistent with the overarching trend indicating equivalent outcomes for family interventions delivered via videoconferencing compared to delivered in-person (Breaux et al., 2021; Comer & Myers, 2016; Comer et al., 2017; Fogler et al., 2020; Myers et al., 2015; Prinz et al., 2021). There is initial evidence that telehealth leads to superior outcomes in some domains and inferior outcomes in others (e.g., Breaux et al., 2021), but we are not able to investigate these nuances in the current trial. Parents were able to attend sessions according to their own schedule, and engagement was viewed positively as no parents who initiated the treatment dropped out. School counselors and other school mental health professionals who aim to improve family-school partnerships and parent engagement in the child’s academic success may therefore consider a similar intervention. The current intervention provided positive behavioral support strategies aimed at improving a parent-identified behavioral concern at home related to the child’s academic success. This may have positively impacted initial parent buy-in and subsequent engagement.
Limitations and Future Directions
By utilizing a multiple baseline design, this study is limited such that findings on measures other than the daily measure (DBR academic engagement, respectful behavior, and disruptive behavior) should be interpreted with caution. These measures should be viewed as descriptive and utilized to generate hypotheses for future studies. Specifically, it is not clear whether teachers had sufficient experience working with these children to provide accurate reports on the IRS. DBR ratings may have been affected by the home learning environment in that parents may not have been monitoring their children consistently. However, DBR ratings were scheduled during times that parents indicated they would be able to observe their children’s home learning. DBR reliability was assessed during scheduled, recorded home observations which may have been different from daily DBR ratings. Future studies may implement passive or unobtrusive recording technologies to assess inter-rater reliability. Additionally, two Ph.D., postdoctoral clinical psychology trainees administered treatment. This is infeasible in most settings due to cost of Ph.D.-level providers, and thus future research should evaluate treatment effectiveness with masters-level providers. This also led to a confounding of intervention success with assigned treatment provider as Sophia’s mother had a different therapist than Olivia’s and Alex’s mothers had. We are therefore unable to determine if differences in treatment response were a result of therapist-specific effects. However, fidelity to treatment content did not vary between therapists, and, on observed measures, all families appeared to respond to treatment, reducing the likelihood that assigned therapist explains differences in treatment response.
Future research should include more in-depth focus on parental psychopathology (e.g., ADHD or depression), family stress, and oppositional behavior given variability in response across families. Two families dropped out prior to treatment starting, and the results may therefore represent families who are unsystematically more likely to engage in treatment. Further, participating families were White and non-Hispanic/Latinx, reducing generalizability of findings. Future research should investigate effects with racially diverse and underrepresented families. Overall impairment was also not improved at post-treatment, indicating that additional supports and interventions may be needed to address areas of functional impairment beyond the home learning situation in future studies. Given the timing of the current study and elevated needs of children and families, the lack of change in overall impairment may indicate that the current treatment was insufficient to promote clinically significant, generalized improvement in child behavior. Teacher demographics were not collected.
Most importantly, this is a multiple-baseline trial and is therefore vulnerable to effects of maturation confounding findings. Without a control group, confounding variables cannot be ruled out. However, given decades of randomized trials of BPT, recent investigations of homework-focused BPT and telehealth-delivered BPT, and meta-analytic evidence of BPT efficacy for children with ADHD (Fabiano et al., 2021; Merrill et al., 2017; Power et al., 2012), we believe the current study demonstrating effectiveness for two of three children is valid.
Conclusions
Despite the multifaceted challenges and stressors faced by families during the COVID-19 pandemic, home learning-focused BPT delivered via telehealth was associated with improvements in academic engagement for two of three families. In combination with available evidence, this suggests that evidence-based BPT programs can be modified to target emergent needs of children and families. It is important to note that clinical impairment remained across families, and this work therefore does not suggest that home learning is a preferable form of learning for youth with ADHD. This study is not poised to address that question, and emerging COVID-19 impact research suggests the opposite (e.g., Melegari et al., 2021; Pecor et al., 2021; Wendel et al., 2020). Rather, given the circumstances of increased stress and virus mitigation efforts, home learning-focused BPT may be an effective support for families to improve the academic behavior of their children with ADHD—especially if parents report home learning or homework as the primary difficulty at home. More work is needed to examine differential effects for children with varying presenting problems such as oppositional behavior. Clinicians may consider utilizing home learning-focused BPT to support families of children with ADHD as they continue to encounter home learning via homework or unplanned circumstances including quarantines and school closures.
Notes
Sophia’s teacher did not report impairment prior to the start of the study. However, diagnosis was established based on teacher ratings of impairment from the previous year. These were believed to be more accurate given that Sophia’s current teacher had limited experience working with Sophia due to remote and hybrid schooling
References
Barkley, R. A., Fischer, M., Smallish, L., & Fletcher, K. (2006). Young adult outcome of hyperactive children: Adaptive functioning in major life activities. Journal of the American Academy of Child and Adolescent Psychiatry, 45(2), 192–202. https://doi.org/10.1097/01.chi.0000189134.97436.e2
Becker, S. P., Breaux, R., Cusick, C. N., Dvorsky, M. R., Marsh, N. P., Sciberras, E., & Langberg, J. M. (2020). Remote learning during COVID-19: Examining school practices, service continuation, and difficulties for adolescents with and without attention-deficit/hyperactivity disorder. Journal of Adolescent Health, 67(6), 769–777. https://doi.org/10.1016/j.jadohealth.2020.09.002
Booster, G. D., Dupaul, G. J., Eiraldi, R., & Power, T. J. (2012). Functional impairments in children with ADHD: Unique effects of age and comorbid status. Journal of Attention Disorders, 16(3), 179–189. https://doi.org/10.1177/1087054710383239
Breaux, R., Shroff, D. M., Cash, A. R., Swanson, C. S., Carlton, C., Bertollo, J. R., & Dahiya, A. V. (2021). Telehealth delivery of the RELAX intervention for families of adolescents diagnosed with ADHD: Preliminary treatment outcomes and evidence of acceptability and feasibility. Evidence-Based Practice in Child and Adolescent Mental Health. https://doi.org/10.1080/23794925.2021.1970053
Brestan, E., Jacobs, J., Rayfield, A., & Eyberg, S. M. (1999). A consumer satisfaction measure for parent-child treatments and its relationship to measures of child behavior change. Behavior Therapy, 30, 17–30.
Briesch, A. M., Chafouleas, S. M., & Riley-Tillman, T. C. (2010). Generalizability and dependability of behavior assessment methods to estimate academic engagement: A comparison of systematic direct observation and direct behavior rating. School Psychology Review, 39, 408–421.
Chafouleas, S. M., Riley-Tillman, T. C., & Christ, T. J. (2009). Direct behavior rating (DBR): An emerging method for assessing social behavior within a tiered intervention system. Assessment for Effective Intervention, 34(4), 195–200.
Christ, T. J., Riley-Tillman, T. C., & Chafouleas, S. M. (2009). Foundation for the development and use of direct behavior rating (DBR) to assess and evaluate student behavior. Assessment for Effective Intervention, 34(4), 201–213.
Christ, T. J., Riley-Tillman, T. C., Chafouleas, S. M., & Boice, C. H. (2010). Direct behavior rating (DBR): Generalizability and dependability across raters and observations. Educational and Psychological Measurement, 70(5), 825–843. https://doi.org/10.1177/0013164410366695
Chronis-Tuscano, A., & Johnson, C. (2014). Families and ADHD. In R. A. Barkley (Ed.), Attention-deficit hyperactivity disorder (4th ed., pp. 191–209). Guilford Press.
Chronis-Tuscano, A., Raggi, V. L., Clarke, T. L., Rooney, M. E., Diaz, Y., & Pian, J. (2008). Associations between maternal attention-deficit/hyperactivity disorder symptoms and parenting. Journal of Abnormal Child Psychology, 36(8), 1237–1250. https://doi.org/10.1007/s10802-008-9246-4
Chronis-Tuscano, A., Rooney, M., Seymour, K. E., Lavin, H. J., Pian, J., Robb, A., & Stein, M. A. (2010). Effects of maternal stimulant medication on observed parenting in mother-child dyads with attention-deficit/hyperactivity disorder. Journal of Clinical Child and Adolescent Psychology, 39(4), 581–587. https://doi.org/10.1080/15374416.2010.486326
Chronis-Tuscano, A., O’Brien, K., & Danko, C. (2021). Supporting caregivers of children with ADHD: An integrated parenting program: Therapist guide. Oxford University Press.
Comer, J. S., & Myers, K. (2016). Future directions in the use of telemental health to improve the accessibility and quality of children’s mental health services. Journal of Child and Adolescent Psychopharmacology, 26(3), 296–300. https://doi.org/10.1089/cap.2015.0079
Comer, J. S., Furr, J. M., Miguel, E. M., Cooper-Vince, C. E., Carpenter, A. L., Elkins, R. M., & Chase, R. (2017). Remotely delivering real-time parent training to the home: An initial randomized trial of Internet-delivered parent-child interaction therapy (I-PCIT). Journal of Consulting and Clinical Psychology, 85(9), 909–917. https://doi.org/10.1037/ccp0000230
Cray, K., & Ome, M. (2021, March 8). Snow days may never be the same. The Atlantic. https://www.theatlantic.com/family/archive/2021/03/snow-days-are-endangered-remote-learning/618216/.
Danforth, J. S., Anderson, L., Barkley, R. A., & Stokes, T. F. (1991). Observations of parent-child interactions with hyperactive children: Research and clinical implications. Clinical Psychology Review, 11(6), 703–727.
Danielson, M. L., Bitsko, R. H., Ghandour, R. M., Holbrook, J. R., Kogan, M. D., & Blumberg, S. J. (2018). Prevalence of parent-reported ADHD diagnosis and associated treatment among U.S. children and adolescents, 2016. Journal of Clinical Child and Adolescent Psychology, 47(2), 199–212. https://doi.org/10.1080/15374416.2017.1417860
Deater-Deckard, K. (2017). Parents’ and children’s ADHD in a family system. Journal of Abnormal Child Psychology, 45(3), 519–525. https://doi.org/10.1007/s10802-017-0276-7
DuPaul, G. J., Kern, L., Belk, G., Custer, B., Daffner, M., Hatfield, A., & Peek, D. (2018). Face-to-face versus online behavioral parent training for young children at risk for ADHD: Treatment engagement and outcomes. Journal of Clinical Child & Adolescent Psychology, 47(sup1), S369–S383.
Evans, S. W., Owens, J. S., Wymbs, B. T., & Ray, A. R. (2018). Evidence-based psychosocial treatments for children and adolescents with attention deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 47(2), 157–198.
Eyberg, S. M., & Robinson, E. A. (1983). Dyadic parent-child interaction coding system (DPICS): A manual. Psychological Documents, 13, 24.
Eyberg, S. M., Nelson, M. M., Duke, M., & Boggs, S. R. (2009). Manual for the dyadic parent-child interaction coding system (3rd ed.). Unpublished coding manual.
Fabiano, G. A., Pelham, W. E., Jr., Waschbusch, D. A., Gnagy, E. M., Lahey, B. B., Chronis, A. M., & Burrows-Maclean, L. (2006). A practical measure of impairment: Psychometric properties of the impairment rating scale in samples of children with attention deficit hyperactivity disorder and two school-based samples. Journal of Clinical Child and Adolescent Psychology, 35(3), 369–385. https://doi.org/10.1207/s15374424jccp3503_3
Fabiano, G. A., Pelham, W. E., Gnagy, E. M., Burrows-MacLean, L., Coles, E. K., Chacko, A., Wymbs, B. T., Walker, K. S., Arnold, F., Garefino, A., Keenan, J. K., Onyango, A. N., Hoffman, M. T., Massetti, G. M., & Robb, J. A. (2007). The single and combined effects of multiple intensities of behavior modification and multiple intensities of methylphenidate in a classroom setting. School Psychology Review, 36, 195–216.
Fabiano, G. A., Pyle, K., Kelty, M. B., & Parham, B. R. (2017). Progress monitoring using direct behavior rating single item scales in a multiple-baseline design study of the daily report card intervention. Assessment for Effective Intervention, 43(1), 21–33. https://doi.org/10.1177/1534508417703024
Fabiano, G. A., Schatz, N. K., Aloe, A. M., Pelham, W. E., Jr., Smyth, A. C., Zhao, X., & Coxe, S. (2021). Comprehensive meta-analysis of attention-deficit/hyperactivity disorder psychosocial treatments investigated within between group studies. Review of Educational Research, 91(5), 718–760.
Fogler, J. M., Normand, S., O’Dea, N., Mautone, J. A., Featherston, M., Power, T. J., & Nissley-Tsiopinis, J. (2020). Implementing group parent training in telepsychology: Lessons learned during the COVID-19 pandemic. Journal of Pediatric Psychology, 45(9), 983–989. https://doi.org/10.1093/jpepsy/jsaa085
Harris, A. N., Stoppelbein, L., Greening, L., Becker, S. P., Luebbe, A., & Fite, P. (2014). Child routines and parental adjustment as correlates of internalizing and externalizing symptoms in children diagnosed with ADHD. Child Psychiatry & Human Development, 45(2), 243–253.
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., & O’Neal, L. (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 95, 103208.
Johnston, C., & Mash, E. J. (2001). Families of children with attention-deficity/hyperactivity disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4(3), 183–207.
Joline, E., & B., Lainie K, H., Susan D, A., Amy J, H., Robert, R., & Maurice G, S. (2020). School reopening during COVID-19 pandemic: Considering students with disabilities. Journal of Pediatric Rehabilitation Medicine, 13, 1–7.
Koo, T. K., & Li, M. Y. (2016). A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15(2), 155–163.
Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M & Shadish, W. R. (2010). Single-case designs technical documentation. Retrieved from What Works Clearinghouse website: http://ies.ed.gov/ncee/wwc/pdf/wwc_scd.pdf.Langberg, J. M., Arnold, L. E., Flowers, A. M., Altaye, M., Epstein, J. N., & Molina, B. S. (2010). Assessing homework problems in children with ADHD: validation of a parent-report measure and evaluation of homework performance patterns. School Mental Health, 2(1), 3–12. doi:https://doi.org/10.1007/s12310-009-9021-x
Kuhfeld, M., Tarasawa, B., Johnson, A., Ruzek, E., & Lewis, K. (2020). Learning during COVID-19: Initial findings on students' reading and math achievement and growth. Retrieved from https://www.nwea.org/research/publication.
Kuriyan, A. B., Pelham, W. E., Jr., Molina, B. S., Waschbusch, D. A., Gnagy, E. M., Sibley, M. H., & Kent, K. M. (2013). Young adult educational and vocational outcomes of children diagnosed with ADHD. Journal of Abnormal Child Psychology, 41(1), 27–41. https://doi.org/10.1007/s10802-012-9658-z
Langberg, J. M., Dvorsky, M. R., & Evans, S. W. (2013). What specific facets of executive function are associated with academic functioning in youth with attention-deficit/hyperactivity disorder? Journal of Abnormal Child Psychology, 41(7), 1145–1159.
Larsen, L., Helland, M. S., & Holt, T. (2021). The impact of school closure and social isolation on children in vulnerable families during COVID-19: a focus on children’s reactions. European Child & Adolescent Psychiatry, 31, 1–11.
Lupas, K. K., Mavrakis, A., Altszuler, A., Tower, D., Gnagy, E., MacPhee, F., & Pelham, W., Jr. (2021). The short-term impact of remote instruction on achievement in children with ADHD during the COVID-19 pandemic. School Psychology, 36(5), 313.
Masonbrink, A. R., & Hurley, E. (2020). Advocating for children during the COVID-19 school closures. Pediatrics, 146 (3).
Massetti, G. M., Pelham, W. E., Chacko, A., Walker, K. S., Arnold, F. W., Coles, E. K., Wymbs B. T., Swanger, M. S., Robb, J. A., Fabiano, G. A., Onyango, A. N., Gnagy, E. M., & Burrows-MacLean, L. (2003). Situational variability of ADHD, ODD and CD: Psychometric properties of the DBD Interview and Rating Scale. In Poster presented at the association for advancement of behavior therapy conference, Boston, MA.
Melegari, M. G., Giallonardo, M., Sacco, R., Marcucci, L., Orecchio, S., & Bruni, O. (2021). Identifying the impact of the confinement of Covid-19 on emotional-mood and behavioural dimensions in children and adolescents with attention deficit hyperactivity disorder. Psychiatry Research, 296, 113692. https://doi.org/10.1016/j.psychres.2020.113692
Merrill, B. M., Morrow, A. S., Altszuler, A. R., Macphee, F. L., Gnagy, E. M., Greiner, A. R., & Pelham, W. E., Jr. (2017). Improving homework performance among children with ADHD: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 85(2), 111–122. https://doi.org/10.1037/ccp0000144
Miller, F. G., Johnson, A. H., Yu, H., Chafouleas, S. M., McCoach, D. B., Riley-Tillman, T. C., & Welsh, M. E. (2018). Methods matter: A multi-trait multi-method analysis of student behavior. Journal of school psychology, 68, 53–72.
Misirli, O., & Ergulec, F. (2021). Emergency remote teaching during the COVID-19 pandemic: Parents experiences and perspectives. Education and Information Technologies, 26(6), 6699–6718.
Myers, K., Vander Stoep, A., Zhou, C., McCarty, C. A., & Katon, W. (2015). Effectiveness of a telehealth service delivery model for treating attention-deficit/hyperactivity disorder: A community-based randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 54(4), 263–274. https://doi.org/10.1016/j.jaac.2015.01.009
Pecor, K. W., Barbyannis, G., Yang, M., Johnson, J., Materasso, S., Borda, M., & Ming, X. (2021). Quality of life changes during the COVID-19 pandemic for caregivers of children with ADHD and/or ASD. International Journal of Environmental Research and Public Health. https://doi.org/10.3390/ijerph18073667
Pelham, W. E., Jr., & Fabiano, G. A. (2008). Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 37(1), 184–214.
Pelham, W. E., Jr., Gnagy, E. M., Greenslade, K. E., & Milich, R. (1992). Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 31(2), 210–218.
Pelham, W. E., Jr., Fabiano, G. A., & Massetti, G. (2005). Evidence-based assessment of Attention Deficit Hyperactivity Disorder in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 34(3), 449–476.
Power, T. J., Karustis, J. L., & Habboushe, D. F. (2001). Homework Success for children with ADHD: A family-school intervention program. Guilford Press.
Power, T. J., Mautone, J. A., Soffer, S. L., Clarke, A. T., Marshall, S. A., Sharman, J., & Jawad, A. F. (2012). A family-school intervention for children with ADHD: Results of a randomized clinical trial. Journal of Consulting and Clinical Psychology, 80(4), 611–623. https://doi.org/10.1037/a0028188
Prinz, R. J., Metzler, C. W., Sanders, M. R., Rusby, J. C., & Cai, C. (2021). Online-delivered parenting intervention for young children with disruptive behavior problems: A noninferiority trial focused on child and parent outcomes. Journal of Child Psychology and Psychiatry, 63, 199–209.
Riley-Tillman, T. C., Christ, T. J., Chafouleas, S. M., Boice, C. H., & Briesch, A. M. (2010). The impact of observation duration on the accuracy of data obtained from direct behavior rating (DBR). Journal of Positive Behavior Interventions, 13, 119–128.
Roy, A. K., Breaux, R., Sciberras, E., Patel, P., Ferrara, E., Shroff, D. M., & Becker, S. P. (2022). A preliminary examination of key strategies, challenges, and benefits of remote learning expressed by parents during the COVID-19 pandemic. School Psychology, 37(2), 147.
Shah, R., Raju, V. V., Sharma, A., & Grover, S. (2021). Impact of COVID-19 and lockdown on children with ADHD and their families-an online survey and a continuity care model. Journal of Neurosciences in Rural Practice, 12(1), 71–79. https://doi.org/10.1055/s-0040-1718645
Smith, T. E., Sheridan, S. M., Kim, E. M., Park, S., & Beretvas, S. N. (2020). The effects of family-school partnership interventions on academic and social-emotional functioning: A meta-analysis exploring what works for whom. Educational Psychology Review, 32(2), 511–544.
Vannest, K. J., Parker, R. I., Gonen, O., & Adiguzel, T. (2016). Single Case Research: Web based calculators for SCR analysis. (Version 2.0) [Web-based application]. College Station, TX: Texas A&M University. Retrieved Tuesday 30th March 2021. Available from singlecaseresearch.org.
Wechsler, D. (2011). Wechsler Abbreviated Scale of Intelligence- Second Edition (WASI-II). San Antonio, TX: NCS Pearson.
Wendel, M., Ritchie, T., Rogers, M. A., Ogg, J. A., Santuzzi, A. M., Shelleby, E. C., & Menter, K. (2020). The association between child ADHD symptoms and changes in parental involvement in kindergarten children’s learning during COVID-19. School Psychology Review, 49(4), 466–479. https://doi.org/10.1080/2372966x.2020.1838233
Wolfe, K., Dickenson, T. S., Miller, B., & McGrath, K. V. (2019). Comparing visual and statistical analysis of multiple baseline design graphs. Behavior Modification, 43(3), 361–388. https://doi.org/10.1177/0145445518768723
Xie, Y., Dixon, J. F., Yee, O. M., Zhang, J., Chen, Y. A., DeAngelo, S., & Schweitzer, J. B. (2013). A study on the effectiveness of videoconferencing on teaching parent training skills to parents of children with ADHD. Telemedicine and e-Health, 19(3), 192–199.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, and data collection were performed by Brittany MM, WJM, and ER. Treatment was implemented by BMM and WJM. The first draft of the manuscript was written by BMM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All study procedures were approved by the Florida International University Institutional Review Board (IRB). Parents and their children completed IRB-approved consent and assent documents. Authors have no disclosures or conflicts of interest. The current study was not funded.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Merrill, B.M., Monopoli, W.J., Rejman, E. et al. Supporting Parents of Children with ADHD During COVID-19 School Closures: A Multiple-Baseline Trial of Behavioral Parent Training for Home Learning. School Mental Health 15, 370–383 (2023). https://doi.org/10.1007/s12310-023-09569-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12310-023-09569-y