
Abstract
We report a case of parasitic twin or incomplete or heteropagus twining of extra portions of a pelvis, lower and upper limbs, duplication of genitalia and herniation of intestinal tract with spleen—variant of conjoined twinning (CT) consistent with fusion of two embryos followed by resorption of the caudal half of one of them, resulting in a normal male baby with the upper half of a male parasitic twin fused to his chest.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Case Report
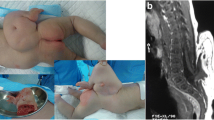
One-day-old male infant with herniation of small bowel and spleen through the lower left side of the abdominal wall defect close to the umbilicus, two upper limbs, two lower limbs, two pelvis and two genitalia was admitted in our department (Fig. 1). The child passed meconium immediately after normal delivery. The infant was diagnosed as a parasitic conjoined twin who was found to be attached to the left of the upper chest through 1 × 1 in. of bridging tissue containing skin, subcutaneous tissue and vascular pedicle. Since the general condition was poor, the child resuscitated with IV fluids, oxygen, blood and antibiotics. The herniated bowel was covered with sterile dressing. All variants of conjoined twins have been reported in the literatures, but parasitic conjoined twins with gastroschisis have rarely been reported in the literatures. The earliest example of conjoined twin marble statue called double goddess is placed in the Anatolian Civilisation Museum, Ankara, Turkey [1].

One day old - parasitic conjoined twin
Diagnosis
Because of poor general condition of the baby, limited investigations were performed. The conjoined twin was evaluated by whole body X-ray, basic blood investigation, electrocardiogram, whole body X-ray, ultrasonogram, intravenous pyelography (IVU), micturating cystourethrogram (MCU) and computerized tomography. Magnetic resonance imaging did not add much to ultrasonography when evaluating the conjoined twins [2]. The conjoined twin had single heart, double pelvis, double upper and lower limbs, single hepatobiliary system, two kidneys, two sets of ureters, double bladder, double genitalia with empty scrotum of parasite, herniated portion of the intestine and spleen.
Discussion
Conjoined twins can be classified as symmetrical or asymmetrical. Asymmetrical (incomplete) conjoined twins result from the disappearance of one of the twins with remnant structures attached to the complete twin, with the remaining junction. The incidence of parasitic or heterotopic monozygotic conjoined twinning is about one or two per million live births. Conjoined twins are identified by prenatal ultrasonography, but this mother did not undergo ultrasonography prenatally. Intrauterine distress in conjoined twins can be avoided by elective caesarean section. The conjoined twins can be diagnosed by the 12th week of gestation with prenatal ultrasonography. Anatomical details of conjoined organs can be determined by prenatal ultrasonography at 20th week. The timing of surgical separation may be variable, but it is best to plan on separation on an elective basis when the infants are 9–12 months of age. Emergent condition such as congestive cardiac failure, respiratory distress, intestinal obstruction, gastroschisis and obstructive uropathy may necessitate early separation [3]. The surgical separation presents a great challenge and requires multispecialty team.
Initially, we planned to repair gastroschisis and then separation of parasite. On a table, we found that the parasite was interfering with the surgical procedure, and hence, we decided to proceed initially for the separation of the parasite and then bowel repair.
Complete reduction of the herniated bowel and abdominal wall closure were not possible in this baby. We decided to treat gastroschisis without creating undue intra-abdominal pressure and tension in the abdominal wall closure. So, the staged reduction described by Schuster with silastic sheeting (sterile urobag) [4] was performed. Defect in the chest wall after excision of the parasite was covered by the skin flap raised from the parasite (Fig. 2). Post-operatively, the separated infant was connected to the ventilator and monitored in the intensive care unit with regulated fluid and antibiotics.

After excision of the parasite
Conclusion
The infant in our case died after 12 h after surgery, and the mortality may be due to sudden ET tube block, poor diaphragmatic function, cerebral anoxia or unresolved aspiration. We were not able to determine the exact cause of death. Prognosis depends on the state of conjoined organs, associated anomalies and the potential for successful separation. Detailed preoperative assessment is essential to determine the best surgical approach, reconstruction methods and ultimate outcome
References
Geroulanos S, Jaggi F, Wydler J, Lachat M, Cakmakci M (1993) Thoracopagus symmetricus. Gesnerus 50:179–200
Turner RJ et al (1986) Magnetic resonance imaging and ultrasonography in the antenatal evaluation of conjoined twins. Am J Obstet Gynecol 155:645
Schuster SR (1967) A new method for the staged repair of large omphaloceles. Surg Gynecol Obstet 125:837–850
O’Neill and others: Ann: Surg, 308, September. 1988
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Baskaran, D., Aleem, M.A. & Ravi, R. Parasitic Twin with Gastroschisis Is One of the Rarest Variant of Conjoined Twins: a Case Report. Indian J Surg 77 (Suppl 1), 90–91 (2015). https://doi.org/10.1007/s12262-014-1165-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-014-1165-8