
Abstract
Objective
To evaluate the relevance of high-resolution computed tomography (HRCT) findings and fluorine-18-fluorodeoxyglucose (18F-FDG) uptake for risk stratification of visceral pleural invasion by lung adenocarcinoma.
Methods
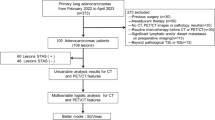
The HRCT findings and 18F-FDG uptake for lung adenocarcinomas with pleural contact on CT were retrospectively analyzed in 208 consecutive patients (94 females and 114 males; median age, 69.0 years) between January 2009 and December 2013, with institutional review board approval. The HRCT findings and maximum standardized uptake value (SUVmax) were recorded for each patient. Multivariate logistic regression was used for statistical analysis, and subgroup analysis stratified for whole tumor size ≤3 cm was also performed.
Results
Multivariate analysis showed that SUVmax [odds ratio (OR) 1.09, 95 % confidence interval (CI) 1.02–1.16, P = 0.014] and obtuse angle (OR 4.14, 95 % CI 1.97–8.74, P < 0.001) were significant independent predictors for visceral pleural invasion. Receiver operating characteristic (ROC) analysis showed that, compared with the multivariate models [area under the curve (Az) 0.819–0.829], SUVmax alone (Az 0.815) was useful in predicting visceral pleural invasion. In the subgroup analysis, multivariate analysis showed that SUVmax (OR 1.29, 95 % CI 1.12–1.50, P = 0.001) and contact length with the pleura (OR 1.13, 95 % CI 1.05–1.22, P = 0.001) were significant independent predictors for visceral pleural invasion. ROC analysis showed that SUVmax alone (Az 0.844) showed similar diagnostic performance to the multivariate models (Az 0.845–0.857).
Conclusions
SUVmax alone and multivariate models including SUVmax are useful for the prediction of visceral pleural invasion by lung adenocarcinoma.

Similar content being viewed by others


References
Kawaguchi K, Mori S, Usami N, Fukui T, Mitsudomi T, Yokoi K. Preoperative evaluation of the depth of chest wall invasion and the extent of combined resections in lung cancer patients. Lung Cancer. 2009;64(1):41–4.
Suzuki N, Saitoh T, Kitamura S. Tumor invasion of the chest wall in lung cancer: diagnosis with US. Radiology. 1993;187(1):39–42.
Murata K, Takahashi M, Mori M, Shimoyama K, Mishina A, Fujino S, et al. Chest wall and mediastinal invasion by lung cancer: evaluation with multisection expiratory dynamic CT. Radiology. 1994;191(1):251–5.
Shirakawa T, Fukuda K, Miyamoto Y, Tanabe H, Tada S. Parietal pleural invasion of lung masses: evaluation with CT performed during deep inspiration and expiration. Radiology. 1994;192(3):809–11.
Akata S, Kajiwara N, Park J, Yoshimura M, Kakizaki D, Abe K, et al. Evaluation of chest wall invasion by lung cancer using respiratory dynamic MRI. J Med Imag Rad Oncol. 2008;52(1):36–9.
Hamasaki M, Kato F, Koga K, Hayashi H, Aoki M, Miyake Y, et al. Invasion of the inner and outer layers of the visceral pleura in pT1 size lung adenocarcinoma measuring ≤3 cm: correlation with malignant aggressiveness and prognosis. Virchows Archiv Int J Pathol. 2012;461(5):513–9.
Kato T, Ishikawa K, Aragaki M, Sato M, Okamoto K, Ishibashi T, et al. Angiolymphatic invasion exerts a strong impact on surgical outcomes for stage I lung adenocarcinoma, but not non-adenocarcinoma. Lung Cancer. 2012;77(2):394–400.
Neri S, Yoshida J, Ishii G, Matsumura Y, Aokage K, Hishida T, et al. Prognostic impact of microscopic vessel invasion and visceral pleural invasion in non-small cell lung cancer: a retrospective analysis of 2657 patients. Ann Surg. 2014.
Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–14.
Higashi K, Ueda Y, Arisaka Y, Sakuma T, Nambu Y, Oguchi M, et al. 18F-FDG uptake as a biologic prognostic factor for recurrence in patients with surgically resected non-small cell lung cancer. J Nuclear Med Off Publ Soc Nuclear Med. 2002;43(1):39–45.
Travis WBE, Muller-Hermelink H, Harris C. International histological classification of tumors. 3rd ed. Lyon: IARC Press; 2004.
Glazer HS, Duncan-Meyer J, Aronberg DJ, Moran JF, Levitt RG, Sagel SS. Pleural and chest wall invasion in bronchogenic carcinoma: cT evaluation. Radiology. 1985;157(1):191–4.
Ratto GB, Piacenza G, Frola C, Musante F, Serrano I, Giua R, et al. Chest wall involvement by lung cancer: computed tomographic detection and results of operation. Ann Thoracic Surg. 1991;51(2):182–8.
Imai K, Minamiya Y, Ishiyama K, Hashimoto M, Saito H, Motoyama S, et al. Use of CT to evaluate pleural invasion in non-small cell lung cancer: measurement of the ratio of the interface between tumor and neighboring structures to maximum tumor diameter. Radiology. 2013;267(2):619–26.
Casali C, Cucca M, Rossi G, Barbieri F, Iacuzio L, Bagni B, et al. The variation of prognostic significance of Maximum Standardized Uptake Value of [18F]-fluoro-2-deoxy-glucose positron emission tomography in different histological subtypes and pathological stages of surgically resected Non-Small Cell Lung Carcinoma. Lung Cancer. 2010;69(2):187–93.
Tsutani Y, Miyata Y, Nakayama H, Okumura S, Adachi S, Yoshimura M, et al. Prediction of pathologic node-negative clinical stage IA lung adenocarcinoma for optimal candidates undergoing sublobar resection. J Thoracic Cardiovas Surg. 2012;144(6):1365–71.
Domen H, Hida Y, Okamoto S, Hatanaka KC, Hatanaka Y, Kaga K, et al. Histopathologic characterization of lung adenocarcinoma in relation to fluorine-18-fluorodeoxyglucose uptake on positron emission tomography. Jpn J Clin Oncol. 2013;43(9):874–82.
Maeda R, Isowa N, Onuma H, Miura H, Harada T, Touge H, et al. The maximum standardized 18F-fluorodeoxyglucose uptake on positron emission tomography predicts lymph node metastasis and invasiveness in clinical stage IA non-small cell lung cancer. Interact Cardio Vasc Thorac Surg. 2009;9(1):79–82.
Takenaka T, Yano T, Morodomi Y, Ito K, Miura N, Kawano D, et al. Prediction of true-negative lymph node metastasis in clinical IA non-small cell lung cancer by measuring standardized uptake values on positron emission tomography. Surg Today. 2012;42(10):934–9.
Hattori A, Suzuki K, Matsunaga T, Fukui M, Tsushima Y, Takamochi K, et al. Tumour standardized uptake value on positron emission tomography is a novel predictor of adenocarcinoma in situ for c-Stage IA lung cancer patients with a part-solid nodule on thin-section computed tomography scan. Interact CardioVasc Thorac Surg. 2014;18(3):329–34.
Williford ME, Hidalgo H, Putman CE, Korobkin M, Ram PC. Computed tomography of pleural disease. AJR Am J Roentgenol. 1983;140(5):909–14.
Tsutani Y, Miyata Y, Mimae T, Kushitani K, Takeshima Y, Yoshimura M, et al. The prognostic role of pathologic invasive component size, excluding lepidic growth, in stage I lung adenocarcinoma. J Thoracic Cardiovasc Surg. 2013;146(3):580–5.
Tamura M, Oda M, Matsumoto I, Shimizu Y, Waseda R, Watanabe G. Radiologic and nuclear medicine predictors of tumor invasiveness in patients with clinical stage IA lung adenocarcinoma. World J Surg. 2011;35(9):2010–5.
Yanagawa M, Tanaka Y, Leung AN, Morii E, Kusumoto M, Watanabe S, et al. Prognostic importance of volumetric measurements in stage I lung adenocarcinoma. Radiology. 2014;272(2):557–67.
Conflict of interest
No potential conflicts of interest were disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tanaka, T., Shinya, T., Sato, S. et al. Predicting pleural invasion using HRCT and 18F-FDG PET/CT in lung adenocarcinoma with pleural contact. Ann Nucl Med 29, 757–765 (2015). https://doi.org/10.1007/s12149-015-0999-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-015-0999-x