
Abstract
Objective
To compare postductal heart rate and saturation (SpO2) measurements from the wireless PO device obtained by iVital+ against measurements by the standard Masimo (SET technology) monitor in the monitoring of neonates.
Methods
Pulse oximetry reading of newborns were assessed in terms of heart rate and saturations with two PO simultaneously attached to postductal site and data comparison was done.
Results
Out of the 1000 cumulative recordings, the mean difference between HR obtained from both PO was 0.415 and level of agreement was 2.3 beats per minute. For SpO2 mean difference between devices was 1.21 and level of agreement was 1.5%. There was very little difference between SpO2 measurements when the Masimo SpO2 was ≥ 70%.
Conclusion
As this pulse oximeter is small, portable and accuracy is as comparable to Masimo, this provides a good solution for efficaciously monitoring neonates. It can also be used in the monitoring of children with suspected or affected with COVID-19 in hospital and ICU settings as also in the quarantine facilities. This reduces the need for constant presence of medical and nursing personnel.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Neonatal monitoring continuously in the NICU and neonatal wards helps in the identification of fluctuations in the physiological parameters and in the early intervention. The authors have endeavoured in this study to show that quality of care can be enhanced by the use of ‘Continuous portable remote monitoring’ in real-time of neonates. The standard of monitoring in an ICU setting, unfortunately, cannot be made available for every baby in most maternity hospitals. Continuous monitoring of the neonate’s vital signs and physiological parameters can be achieved with the development and fusion of wearable sensing technologies coupled with wireless communication techniques and data processing algorithms. If applied as a clinical tool, a wearable sensor system for patients can be applied to obtain the data remotely by the clinicians. Traditional sensors and medical instruments cannot be used for wearable physiological monitoring applications, as they are difficult to wear for long periods, and they also cause discomfort to the wearer, including skin irritation, hampering due to wires, interruption of sleep, and lack of communication because of the limitations of technologies in sensors, wireless networks, and energy supply. Hence, these systems should be capable of carefully, conveniently, and robustly monitoring babies in the NICU or at home. Wearable electronics can effectively avoid all the above discomforts and monitor neonates remotely. It needs to be ensured, however, that this data are accurate in the neonatal population. Remote monitoring has earlier met with skepticisms about its viability, accuracy, and quality. Masimo pulse-oximetry is the current standard of care in the NICUs across the globe [1]. Masimo SET PO model accounts for saturation values (SpO2) contributed for true arterial signals and by one or more motion or noise signals [2]. The present study has compared the new inexpensive indigenous wireless technology PO capable of remote monitoring by transmitting data across the cloud platform with the Masimo SET PO. Remote monitoring data have helped people in teleconsultations and people have used it in electronic ICU in remote monitoring data [3]. The authors have tried to see whether data from ‘remote monitoring wireless device’ is equally effective as the standard of care. The aim of the present study was to compare postductal heart rate and saturation (SpO2) measurements from the wireless PO device obtained by iVital+ against measurements by the standard Masimo (SET technology) monitor in the monitoring of neonates.
Material and Methods
Masimo signal extraction technology (SET) Radical (v4) PO set to 2 s data averaging and maximum sensitivity with the low noise optical probe (LNOP) Neo-L adhesive sensor (Masimo Corporation, Irvine, CA, USA) was used [2].
Smart PO with healthcare internet of things (HcIOT) [2] sensor coupled with bluetooth low energy (BLE)ver 4.0 was used for transmission of data over the cloud-based computing resource. (Helyxon Healthcare solution Pvt Ltd, IIT Madras Research Park, Taramani, Chennai, India) [4].
The study was undertaken on forty healthy neonates to see the accuracy of data captured by remotely monitoring them with an indigenous, inexpensive, simple wireless PO device (B) (iVital Helyxion) compared to standard care using Masimo monitoring device (A) [2] for heart rate and oxygen saturation. Eligible infants were those born at or near term and admitted to neonatal wards postdelivery. Neonates with major congenital anomalies and sick neonates were excluded from the study. Written parental consent was obtained. Clinical history, physical findings, and probable diagnosis were noted in all neonates in a predefined proforma. Babies were simultaneously monitored using both ‘Masimo PO’ and the ‘wireless PO’. PO sensor was applied by the researcher around each midfoot to reduce interference from light, cross-talk between sensors and to avoid the preductal and postductal differences at 24 h of postnatal age. Serial recordings with the predefined interval were taken when the neonate was calm and sleeping. Recordings of HR and SpO2 measurements from both the oximeters were collected. Twenty-five of these measurements were noted on a data collection sheet at 5 min intervals from each neonate. A total of 1000 readings were taken from 40 healthy neonates, 987 readings were in the range of > 95%, 11 readings were in the range of 90%–94%, 2 readings were in the range of 85%–90% and none of the readings were below 80%. The same pulse oximeter was used to measure all the readings from all 40 neonates to avoid differences between machines.
Data extraction commenced when both the monitors displayed measurements. Recordings were paused every minute, when each investigator recorded HR, SpO2 and signal quality for their respective monitor. Good-quality signal was defined a priori for each monitor as—iVital PO: regular plethysmograph, pulse search, and interference indicators not lit continuously; Masimo PO: regular plethysmograph, large vertical bars at the base of the screen, and absence of error messages (Fig. 1).

Sequence diagram of data extraction and monitoring
Clinical and demographic data from the medical records and data from the recording from PO were entered into Microsoft Excel and analyzed using SPSS software. The Bland–Altman method was used to determine agreement between HRiVital and HRMasimo and between SpO2iVital and SpO2Masimo. The percentage similarity graph was plotted to check the accuracy of the test.
Results
Forty term neonates were recruited after obtaining consent for the study; out of which 25 (62.5%) were males and 15 (37.5%) were females. The study cohort of 40 infants with a total of 1000 observations had a mean gestational age of 38 ± 1.240 SD wk, birth weight 2946 ± 0.208 g and median (interquartile range) Apgar scores of 9 at 1 and 5 min.
There was little difference between HR obtained from the Masimo compared with HR from iVital oximeter. Figure 2 displays the Bland–Altman plot comparing HRMasimo with HRiVital.The Mean HR measured with Masimo PO was 144.7 bpm ± 9.036 SD and with iVital PO was 144.3 bpm ± 9.471 SD and the mean difference (HRMasimo–HRiVital) ± 2 SD was 0.415 and level of agreement was 2.3 beats per min (bpm) n = 1000; 95% limits of level of agreement for HR is at 4.191 to 5.021. Figure 3 explains the percentage similarity of the heart rate between two devices which shows the curve that the tests are accurate and not precise; good test but poor technique.

Bland–Altman plots showing the level of agreement between HR-Masimo and HR-iVital+. The mean difference (HRMasimo–HRiVital+) was 0.415 (±2.305)

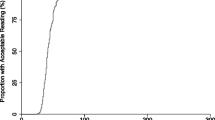
Percentage similarity graph—heart rate. The graph depicts the percentage similarity of the heart rate between two devices and the curve shows that the tests are accurate and not precise; good test but poor technique (graph C of percentage similarity interpretation graph)
For the total number of SpO2 measurements (n = 1000), the mean SpO2 measured with Masimo PO was 97.7% ± 1.597 SD, and with iVital PO was 97.8% ± 1.456 SD and mean difference between SpO2 measurements (SpO2Masimo–SpO2iVital) (± 2 SD) was 1.21 ± 1.529 SD and level of agreement was 1.5% (Fig. 4). There was very little difference between SpO2 measurements (n = 1000) when the Masimo SpO2 was ≥ 70%; 95% limits of level of agreement for SpO2 was at 2.875 to 3.118. Figure 5 depicts the percentage similarity of the saturations between the two devices, which shows that the tests are accurate and not precise; good test but poor technique.

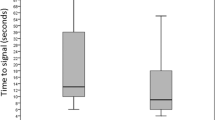
Bland–Altman plots showing the level of agreement between SpO2Masimo and SpO2iVital+. Mean difference between SpO2 measurements (SpO2Masimo–SpO2iVital+) was 0.121 (±1.529)%

Percentage similarity Graph of SpO2. The graph depicts the percentage similarity of the saturations between the two devices and the curve shows that the tests are accurate and not precise; good test but poor technique (graph C of percentage similarity interpretation graph)
Discussion
Previous studies have reported that ECG provides a reliable measure of HR during neonatal resuscitation and monitoring in the NICU. The sensitivity of iVital PO was 95.1% with 95% CI, specificity of 99.9% with CI of 95% reported by a pilot study done by Kamalakannan et al. [4]. The authors report that overall, the iVital oximeters measured HR within 2–3 bpm of HRMasimo, without any statistically significant difference between HRMasimo and HRiVital oximeter. Therefore, the reference range for HR obtained with a Masimo PO [2] is likely to be applicable to the iVital PO. Accuracy of oximeter HR measurements when HR is low is important. The current study recruited infants born at term, a cohort of ‘at low risk’ neonates in the ward. The majority of infants had few measurements recorded about 25 observations from 40 infants where HR were < 100 bpm only for more than a few beats. The accuracy of HR measurements from both oximeters for HR < 100 bpm could not be measured as the number of recordings was insignificant. The iVital PO measured HR, on average, within 3 bpm compared with the Masimo PO, which might be related to the different algorithms used to detect and measure HR. These algorithms affect how each oximeter processes incoming signals, assigns signal relative weightings, and distinguishes signals affected by artefact from true signals.
Pulse oximetry is an important part of examination and an addition to the clinical assessment of infants during resuscitation and monitoring in babies in the NICU. POs measure SpO2 by comparing signal outputs to inbuilt empirical calibration curves. These calibration curves have been experimentally generated by inducing hypoxaemia in healthy young adults. Overall, in the present study there was good agreement between SpO2 measurements from the oximeters. On average, SpO2 measurements from the Masimo POs and iVital POs varied by approximately 1.5%; this difference is unlikely to be clinically important.
In clinical practice, it is recommended that the PO sensor is applied to neonate’s right hand/wrist, as it is a preductal site. In the present study, the Masimo and iVital sensors were placed on either foot so that two postductal sites could be compared. Postductal measurements were used because the concern was that placing two sensors simultaneously, on the right hand/wrist for the study might cause cross-talk between sensors or interference to the distal sensor. Also, pre- and postductal differences would interfere without a comparative study. In this study, the focus was on comparing measurements between the two oximeters, and hence, sensors were placed on either foot (postductal).
Conclusion
The iVital pulse oximeter is a small, portable, inexpensive device whose accuracy of HR and SpO2 data is comparable to the standard of care, i.e., Masimo-SET technology [2], and can be used to monitor newborns in the low-resource settings and neonatal wards, newborns discharged from NICU or in home, as it also transmits the data to centralized data centers so as to help analyze the physiological parameters in real-time.
References
Dawson JA, Saraswat A, Simionato L, et al. Comparison of heart rate and oxygen saturation measurements from Masimo and Nellcor pulse oximeters in newly born term infants. Acta Paediatr. 2013;102:955–60.
Goldman JM, Petterson MT, Kopotic RJ, Barker SJ. Masimo signal extraction pulse oximetry. J Clin Monit Comput. 2000;16:475–83.
Greenhalgh T, Koh GCH, Car J. Covid-19: a remote assessment in primary care. BMJ. 2020;368:m1182.
Kamalakannan D, Kumutha P, Manohran P. Continuous remote monitoring of newborn babies using iVital monitoring system is better than intermittent monitoring – A pilot study. Am J Biomed Eng. 2020;1:1–7.
Acknowledgements
The authors would like to thank Dr H. A. Venkatesh, Consultant Neonatologist for his support, and all the nursing staff and colleagues for their help in the study. A heartfelt thanks to the newborns and parents for having allowed the conduct of this study as well.
Funding
None. The iVital device used in the study was provided free of cost by Helyxon Pvt. Ltd. and the Masimo device was available as a standard device in the hospital.
Author information
Authors and Affiliations
Contributions
SK conducted the study under the supervision of NKN who planned devised and supervised the study. The first draft was written by SK which was modified and corrected by NKN. Both SK and NKN approve the final script. SK will act as the guarantor for this paper.
Corresponding author
Ethics declarations
Ethical Clearance Certificate
Obtained.
Conflict of Interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Keerthy, S., Nagesh, N.K. Efficacious Continuous Monitoring of Infants Using Wireless Remote Monitoring Technology. Indian J Pediatr 89, 771–775 (2022). https://doi.org/10.1007/s12098-021-04035-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-021-04035-6