
Abstract
The ongoing pandemic disease COVID‑19 has caused worldwide social and financial disruption. As many countries are engaged in designing vaccines, the harmful second and third waves of COVID‑19 have already appeared in many countries. To investigate changes in transmission rates and the effect of social distancing in the USA, we formulate a system of ordinary differential equations using data of confirmed cases and deaths in these states: California, Texas, Florida, Georgia, Illinois, Louisiana, Michigan, and Missouri. Our models and their parameter estimations show social distancing can reduce the transmission of COVID‑19 by 60% to 90%. Thus, obeying the movement restriction rules is crucial in reducing the magnitude of the outbreak waves. This study also estimates the percentage of people who were not social distancing ranges between 10% and 18% in these states. Our analysis shows the management restrictions taken by these states do not slow the disease progression enough to contain the outbreak.
Similar content being viewed by others


Introduction
The virus for COVID-19, SARS-CoV-2, is within the species SARS-like coronaviruses. At 125nm, it is marginally bigger than the flu and SARS viruses. The closest related virus started from the Rhinolophus bat which is more than 96% homologous with the current SARS-CoV-2 virus and is only 79% homologous with the original SARS CoV (Fisher and Heymann 2020).
Transmission occurs human-to-human and from close face-to-face social contact, particularly in small enclosed spaces. The transmission rate can be large in a brief period with thousands of new cases every day. While the symptoms of COVID-19 can range broadly from asymptomatic illness to pneumonia and life-threatening complications, the most common symptoms are fever, dry cough, fatigue, nasal congestion, sore throat, and diarrhea. Elderly patients with preexisting respiratory or cardiovascular conditions are the greatest risk group for extreme complications (Fisher and Heymann 2020; Grein et al. 2020; CDC COVID-19 2020).
Since late January 2020, major public health interventions have been implemented in China and other countries to slow the spread of the disease. For example, strong social separation measures and mobility limitations were facilitated and executed by the central and local governments in many countries. These huge social restrictions and alternative interventions have tremendous costs, in terms of socioeconomic and loss of opportunities (Leung et al. 2020; Nicola et al. 2020).
The World Health Organization (WHO) and the US Centers for Disease Control and Prevention (CDC) have prescribed social distancing as one of the main tools to decrease the propagation of COVID-19 and to reduce deaths and strain on healthcare systems in the absence of vaccine (Masters et al. 2020; Wang et al. 2020). The CDC advises three particular social distancing behaviors: (i) remaining more than 6 feet far from each other, (ii) don’t gather in groups, and (iii) staying out of crowded places. These behaviors were mandated by government authorities in most states such as closing schools and restaurants, and researchers found that these government actions reduced the propagation of COVID-19 in the USA (Bourassa et al. 2020; Courtemanche et al. 2020). However, due to high political and economic pressures, the White House and CDC worked on guidelines for relaxing such restrictions on April 16, 2020. While each state started relaxing restrictions at different times, most states started relaxing restrictions in the middle of May 2020 (Chiu et al. 2020; Wang et al. 2020).
There are several studies recently published related to COVID-19 and its effect on social distancing. One of them investigated the effect of the lockdowns for some countries in Europe and the USA by utilizing an SEIR system of ordinary differential equations (ODEs) (Glass 2020). This study compares the basic reproduction number before and after lockdowns. Another work using an SEIR ODE model discussed the timing and corresponding effects of social distancing as control measures on the burden of COVID-19 in the USA (Ngonghala et al. 2020). Similarly, a study quantified the effectiveness of social distancing and discussed the relaxation of social distancing without causing a second wave in Ontario, Canada (Wu et al. 2020). Besides these studies, Waku et al. (2022) proposed an inflection point method to estimate a unique maximum reproduction number and applied this new method to data from the Cameroon COVID-19 outbreak both at national and regional levels. However, we have not found any study analyzing the effect of restrictions in different stages by using SIR-type mathematical models for some specific states in the USA.
In this study, we use mathematical models to examine the effect of relaxing restrictions on the cumulative number of confirmed cases and deaths. We start with introducing the mathematical models in the following section and then discuss fitting the parameters to the data that are retrieved by The New York Times (2020). Finally, the numerical simulations and the behavior of propagation of the disease with relaxing restrictions are discussed in the final section.
Models
We utilize a compartmental ODE model proposed by Aslan et al. (2022) and modify it to include relaxing the restrictions. The ODE system from Aslan et al. (2022) is denoted by Model 1, and the modified ODE system is Model 2. These two models are used to investigate and project the COVID-19 spread in some states in the USA. Model 1 is the preliminary model with ODEs with the rates of change among the compartments of the population given in Fig. 1. This model will represent the population compartments before the relaxing restrictions start. Model 2 is a modified version of Model 1 given in Fig. 2 will present the compartments after relaxing restrictions. The details of these models are given in the following subsections.
Model 1 (the preliminary model)
Model 1 represents the disease spread from the date the first case appears to the date of the first relaxing restrictions and employs a type of feedback mechanism. The rate of confirmed cases (i.e., the number of individuals who are sick, test positive, and are subsequently isolated per day) affects the rate of susceptible individuals, S moving into the social distancing compartment, \(S_d\). When the number of confirmed cases increases, the number of people in social distancing will increase. However, when the daily number of confirmed new cases reaches a low level, social distancing mandates are relaxed, allowing \(S_d\) population individuals to move back into the susceptible compartment with a higher transmission rate. The model simulations illustrate that this decrease in social distancing could result in a new wave of outbreaks.

Flow diagram illustrating the disease transitions among the compartments
In this model, the Susceptible compartment S represents individuals in the population who have not yet been exposed to COVID-19, and are not actively practicing social distancing, and \(S_d\) individuals are susceptible and social distancing in the population. These individuals are strictly practicing the social distancing rules such as using masks and keeping a 6-foot distance. Individuals in the Exposed compartment E have been exposed to COVID-19 but are not yet able to transmit the disease, while those in the Infected I compartment are asymptomatic or only exhibited mild symptoms but have not been tested, confirmed positive, nor consequently isolated. Individuals in the isolated compartment \(I_q\) have tested positive and have been isolated, and finally, the individuals in the recovered R compartment had been infected and have recovered. Figure 1 shows the flow of people among these compartments.
The term
is used to represent the transition rate to social distancing class. Note that, as the number of new cases increases the value of \(\nu (t)\) decreases, and the number of individuals transitioning to social distancing class increases. The force of infection is
where \(N(t)= S + S_d +E +I +I_q +R\). According to the disease progression, the following system of ODEs represents the flow among these compartments.
with \(S(0) > 0, S_d(0) \ge 0, E(0)\ge 0, I(0)\ge 0, I_q(0)\ge 0, R(0)\ge 0\) and \(N(t) = S(t)+S_d(t)+E(t)+I(t)+I_q(t)+R(t).\) The description of parameters is given in Table 1.
To accurately capture the local outbreak dynamics in each state, the key parameters of the model were estimated for each state separately by using data available in The New York Times (2020) and Worldometer (2020) from the date the first case appears to the date, relaxation of the restrictions were first applied.
Model 2
Model 2 starts with the role of relaxing the restrictions. Based on the decision of government authorities and health agencies, a proportion of the people in the \(S_d\) compartment move to the S compartment with an impulse action on the date of the first relaxation of the restrictions, and the system (1) switches to a new dynamical system given in (2).

Flow diagram illustrating the disease transitions among the compartments with impulse action
The initial conditions of this new system are the values of the system (1) at the final time, which corresponds to the first day of relaxing restrictions. Figure 2 shows the flow of people among the compartments for the second model.
This second model differs from the previous model in that a proportion of the social distancing compartment moves instantly to the susceptible compartment by an impulse action. There are no continuous transitions between the susceptible compartment and the social distancing compartment. We update the proportion of people in the susceptible compartment and the social distancing compartment by applying an impulse in the second period of parameter estimation for each state and keep using that estimated proportion p in the rest of the estimations for each state. We decided to use the same proportion for the rest of the states since there were no significant changes in the estimated proportion of people in the social distancing compartment in the rest of the parameter estimations for the other states.
The dynamical system representing this flow is given by a system of ODEs as follows
with \(S(T^+) =pS_d(T^-)+S(T^-), S_d(T^+) =(1-p) S_d(T^-), E(T^+) = E(T^-), I(T^+) = I(T^-),\) \(I_q(T^+) = I_q(T^-), R(T^+) = R(T^-)\) where \(T^+\) is the first day of relaxation of the restrictions, \(T^-\) is the last day of relaxation of the restrictions in previous stage, and \(pS_q(T^-)\) is the proportion of the people in the social distancing compartment that move to the susceptible compartment with impulse action. This model is fitted to the data multiple times from the first date of relaxation of restrictions to March 2nd, 2021, and then the model is used to forecast for 15 days. In the fitting processes, the parameters, \(\beta , r, \mu _q, i_q, \gamma _q\) are estimated multiple times.
Parameter estimation over varying time intervals
We estimate the baseline parameters in the systems (1) and (2) by fitting our models with the number of daily cases and deaths data provided by The New York Times (2020) and Worldometer (2020). We use the Ordinary Least Squares (OLS) method and minimize the sum of the squares of differences between the daily reported data and those predicted by our model. Given a parameter set, the corresponding goodness of fit is measured by computing the associated relative error using the formula
where \(C_j\) and \(\hat{C_j}\) are respectively the reported (from data) and simulated (infected) cases, and \(D_j\) and \(\hat{D_j}\) are respectively the reported and simulated deaths due to COVID-19, with \(j=1,2,..., n\) as the index of the daily reported and simulated cases and deaths. In the estimation of the cumulative number of COVID-19 cases, we consider the cumulative number of confirmed cases in the \(I_q\) compartment. In the estimation of the number of COVID-19 deaths, we sum the number of deaths coming from the infected compartment I and the confirmed (infected) compartment \(I_q\). We used an ode45 solver with fmincon and MultiStart by using the Optimization Toolbox of MATLAB with 10 starting points and used the initial conditions of each state.
We estimated the following parameters for each state: disease transmission rate, \(\beta\), reduction rate due to social distancing, r, transition rate to isolated infected compartment, \(i_q\), transition rate to social distancing compartment, \(s_d\), rate of release from social distancing compartment, \(d_s\), recovery rate due to hospitalization, \(\gamma _q\), the death rate due to disease in the isolated infectious compartment, \(\mu _q\), and death rate due to disease in the infectious compartment, \(\mu _i\). We estimated these parameters for each state separately by using state-specific data. We used the same natural death rate \(d = 2.3\)x\(10^{-5}\) and recruitment rate \(\Pi\) blue depending on the population of each state (World Health Organization 2015). For each state, we used 4.2 days for the average incubation period, \(\frac{1}{\alpha }\), so \(\alpha = 0.2381\) (Nishiura et al. 2020; Guan et al. 2020; Sanche et al. 2020). Finally, we estimated the recovery rate due to natural immune response, \(\gamma _i = 0.111\), and death rate in the infectious compartment, \(\mu _i =0.0001\) by using the total number of cases and deaths in the whole USA and used these estimated values for all states. This estimate for \(\gamma _i\) is almost the same in the work by Renardy et al. (2020). Thus, we did not estimate \(\gamma _i\) and \(\mu _i\) for each state separately since we assumed these values do not change from state to state in the USA.
Numerical simulations
In this section, we discuss the forecasting and fit of models for California, Texas, Florida, Georgia, Illinois, Louisiana, and Michigan. We fitted the models to the data for each state separately, then investigated the relaxing restrictions and their effect on the propagation of COVID-19 for these states. After that, we forecasted the cumulative number of deaths and the cumulative number of cases with different scenarios by changing the social interaction among the people. We considered these states since these states had more cases and deaths during the outbreak and also started to relax restrictions earlier than other states. Furthermore, in this study, we wanted to pick some of the states from different regions. For example, we picked Texas and Florida from the southern part and Illinois and Michigan from the northern part of the USA. We picked Georgia since it was the first state to relax the restrictions and open schools and universities.
To be able to investigate relaxing restrictions in these states, we fitted Model 1 to data from the date the first case appeared to the date of relaxing restriction start, then model 2 given in (2) is fitted to the data multiple times, depending on the date of relaxing restrictions, and the behavior of data. The date of relaxation of the restrictions for each state is adjusted according to the government resources and the data (CNN 2020). After estimating the parameters with these model fits, we compared results for each state to indicate which restriction rules were better to slow down the spread of COVID-19.
When we compare the effect of restriction rules on the propagation of COVID-19, we investigated the cumulative number of cases in each state. In Figs. 3, 4, 5, 6, 7, 8, 9, and 10, the cumulative number of (confirmed) cases between inflection points identifies how big each wave was during the year between March 2020 to March 2021. Note that we have at least three waves for each state between March 2020 and March 2021. For example, in Fig. 3, we have two inflection points, the first one occurs around July 2020, and the second one occurs at the end of November 2020. Thus, the first wave occurs between March 2020 and July 2020, the second wave occurs between July 2020 and November 2020, and the third one occurs between November 2020 and March 2021.
Since we also would like to predict the trajectories of the COVID-19 outbreak in these states, we consider three scenarios until March 17, 2021, in this study. Scenario 1 is shown with green line
 where we forecast with the parameters that are estimated in the currently active restrictions. Scenario 2 is shown with orange line
where we forecast with the parameters that are estimated in the currently active restrictions. Scenario 2 is shown with orange line
 where we forecast with the parameters that are estimated in the currently active restrictions but decrease the social distancing by 50%. Scenario 3 is shown with light green line
where we forecast with the parameters that are estimated in the currently active restrictions but decrease the social distancing by 50%. Scenario 3 is shown with light green line
 where we forecast with the parameters that are estimated in the currently active restrictions but increase the social distancing by 50%. These three scenarios may occur in any state.
where we forecast with the parameters that are estimated in the currently active restrictions but increase the social distancing by 50%. These three scenarios may occur in any state.

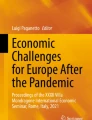
Plots show cumulative cases and deaths in California with data. The average of relative errors in the estimation is about 0.09. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, 50% above and below its estimated value in the last estimation
California
According to the time series of confirmed cases and deaths from March 2020 to March 2021, the second and particularly third waves are much bigger than the first wave (see Fig. 3). Based on the estimated parameters of our model, we also see larger transmission rates as the second and third waves start (see Table 2). We do not see any significant changes in social distancing levels due to no change in reduction rate, r (see Table 2). This indicates that this social distancing level is not enough to completely contain the outbreak in California. We also see the smallest transmission rate, \(\beta\) between January 10th and March 2nd, 2021.
We also made a 15-day forecast for the cumulative number of cases and deaths from March 2nd to March 17th, 2021. Depending on our three scenarios mentioned in the “Numerical simulations” section, Table 3 shows the possible number of cases and deaths for California on the day of March 17th, 2021. Note that we applied these three scenarios only between March 2nd to March 17th, 2021, and the time intervals for each fit were obtained and adjusted according to the dates provided by CNN (2020) .

Plots show cumulative cases and deaths in Texas with data. The average of relative errors in the estimation is about 0.1. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Texas
As can be seen in Fig. 4, the second and third waves are larger than the first wave. Based on our estimated parameters, we see larger transmission rates in the second and third waves which are causing important increases in confirmed cases and deaths in Texas. These increases in transmission rates might be due to decreases in social distancing during the second and third waves (see Table 4). Similar to California, we see the smallest transmission rate between January 25th and March 2nd, 2021. We also forecast the cumulative number of cases and deaths from March 2nd to March 17th, 2021. Depending on our 3 scenarios, Table 5 shows the possible number of cases and deaths for Texas.

Plots show cumulative cases and deaths in Florida with data. The average of relative errors in the estimation is about 0.08. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Florida
Similar to Texas, the second and third waves are again larger than the first wave in Florida (see Fig. 5). Depending on our estimated parameters, we see the larger transmission rates in the second and third waves in Florida (see Table 6). These increases in transmission rates might be due to decreases in social distancing during the second and third waves (see Table 6) in Florida. We also forecast the cumulative number of cases and deaths from March 2nd to March 17th, 2021. Depending on our 3 scenarios, Table 7 shows the possible number of cases and deaths for Florida.

Plots show cumulative cases and deaths in Georgia with data. The average of relative errors in the estimation is about 0.07. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Georgia
According to the time series of confirmed cases and deaths from January 2020 to March 2021, the second and particularly third waves are bigger than the first wave (see Fig. 6). Based on the estimated parameters of our model, we see larger transmission rates during the first wave, and the second and third waves (see Table 8). Even if we see the largest transmission rate in the first wave, the social distancing level is 0.1, which causes a 90% reduction in the transmission rate.
We do not see any significant changes in social distancing levels in the second and third waves since we have no significant changes in reduction rate, r (see Table 8). This indicates that this social distancing level is not enough to completely contain the outbreak in Georgia in the second and third waves. We also see the smallest transmission rate, \(\beta\) between January 25th and March 2nd, 2021, and the largest transmission rate, \(\beta\) between January 25th and May 19th, 2020. We also forecast the cumulative number of cases and deaths from March 2nd to March 17th, 2021. Depending on our 3 scenarios, Table 9 possible number of cases and deaths for Georgia.

Plots show cumulative cases and deaths in Illinois with data. The average of relative errors in the estimation is about 0.05. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Illinois
As it can be seen in Fig. 7, we have 3 waves, and before the second wave ended the third wave occurred. Based on our estimated parameters, we see larger transmission rates in the first, second, and third waves which are causing important increases in confirmed cases and deaths in Illinois. These large transmission rates in the second and third waves might be due to decreases in social distancing during the second and third waves (see Table 10). Even if we see the largest transmission rate in the first wave, the social distancing level is 0.1, which causes a 90% reduction in the transmission rate.
We see the smallest transmission rate between January 25th and March 2nd, 2021. We also forecast the cumulative number of cases and deaths from March 2nd to March 17th, 2021. Depending on our 3 scenarios, Table 11 shows the possible number of cases and deaths for Illinois.

Plots show cumulative cases and deaths in Louisiana with data. The average of relative errors in the estimation is about 0.07. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Louisiana
Based on the time series of confirmed cases and deaths from January 2020 to March 2021, the second and third waves are bigger than the first wave (see Fig. 8). Depending on the estimated parameters of our model, we see larger transmission rates during the first and third waves (see Table 12). Even if we see a smaller transmission rate in the second wave, the social distancing rate is 0.32, which is much worse than in the first and third waves. The social distancing rates were 0.11 and 0.15 in the first and third waves, respectively (see Table 12). Social distancing rate, r causes the smallest reduction in the transmission rate between November 13th, 2020, and March 2nd, 2021. We also forecast the cumulative number of cases and deaths from March 2nd, 2021, to March 17th, 2021. Depending on our 3 scenarios, Table 13 shows the possible number of cases and deaths for Louisiana.

Plots show cumulative cases and deaths in Michigan with data. The average of relative errors in the estimations is about 0.05. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Michigan
As it can be seen in Fig. 9, we have 3 waves, and before the second wave ended the third wave occurred. We see larger transmission rates in the first and second waves based on our estimated parameters. Even if we see a smaller transmission rate in the third wave, the social distancing rate is 0.39, which results in weak social distancing when we compare it with the first and second waves. The social distancing rates are 0.1 and 0.15 in the first and second waves, respectively. These rates cause 90% and 83% reduction in transition rates (see Table 14). Note that the reduction rate, r gets the largest value between October 5th and November 12th when the strongest third wave hits. We also forecast the cumulative number of cases and deaths from March 2nd, 2021, to March 17th, 2021. Depending on our 3 scenarios, Table 15 shows the possible number of cases and deaths for Michigan.

Plots show cumulative cases and deaths in Missouri with data. The average of relative errors in the estimation is about 0.07. The small boxes in the figures refer to 15 days of forecasting by varying the parameter r which is the reduction rate due to social distancing, \(50\%\) above and below its estimated value in the last estimation
Missouri
We have 3 waves and the third wave occurred before the second wave was over (see Fig. 10). Based on our estimated parameters, we see larger transmission rates in the first and third waves (see Table 16). Even if the transmission rate of the third wave is smaller than the transmission rate of the first wave, the reduction in the transmission rate of the third wave is about 74% (0.26) which is smaller than the reduction of the transmission rate of the first wave, which is about 88% (0.12). We see the smallest transmission rate between January 10th, 2021, and March 2nd, 2021. We also forecast the cumulative number of cases and deaths from March 2nd, 2021, to March 17th, 2021. Depending on our 3 scenarios, Table 17 shows the possible number of cases and deaths for Missouri.
Our analysis also indicated that the percentage of people in the susceptible compartment (people who do not socially distance themselves) changes between 10\(\%\) to 18\(\%\) from state to state. Thus, about 82% to 90% of people are socially distancing themselves (i.e., people wearing a mask and avoiding social activities) in states our study. The percentage of people taking social distancing is 90\(\%\) for California, 89\(\%\) for Texas, 84\(\%\) for Florida, 82\(\%\) for Georgia, 88\(\%\) for Illinois, 89\(\%\) for Louisiana, 89\(\%\) for Michigan, and 90\(\%\) for Missouri. We obtained these values in the second fits of each state and fixed these values the same in the third, fourth, and fifth fits for each state. Note that we just considered staying-at-home orders between January 2020 and May 2020 by using model 1 in (1). After May 2020, we considered the \(S_d\) class as the social distancing class instead of considering it as the self-quarantine (staying at home) class by using model 2 in (2). As discussed in the “Model 1 (the preliminary model)”, individuals in the \(S_d\) compartment are just practicing social distancing rules mandated by government authority.
The social distancing compartment (\(S_d\)), reduces the transmission rate of COVID-19 between 60\(\%\) and 90\(\%\) for California, between 76\(\%\) and 88\(\%\) for Texas, between 79\(\%\) and 87\(\%\) for Florida, between 63\(\%\) and 90\(\%\) for Georgia, between 60\(\%\) and 90\(\%\) for Illinois, between 65\(\%\) and 89\(\%\) for Louisiana, and between 61\(\%\) and 90\(\%\) for Michigan, and between 63\(\%\) and 88\(\%\) for Missouri between January 2020 and March 2021 (see the reduction rate due to taking social distancing, r in tables for each corresponding state).
Conclusion and discussion
Practicing social distancing (i.e., using a mask, avoiding contact with others, and obeying all the rules recommended by state governments) reduces transmission rates between 60\(\%\) and 90\(\%\) for the states. However, we see an increase in the reduction rate due to the social distancing from January 2021 to March 2021, which indicates the social distancing level was decreasing over time.
Our study also indicated that the percentage of people who are not taking social distancing changes between 10% to 18% from state to state. The states like Missouri and Illinois have a larger percentage of people practicing social distancing, so any increases in the reduced transmission rate, \(r\beta\) result in a larger wave compared to the states that have a lower percentage of people practicing social distancing like Georgia and Florida.
Even though some states have similarly reduced transmission rates, \(r\beta\), we see stronger waves in the states, which have a larger reduction rate, r. For example, see the tables and figures for California and Illinois. This indicates the reduction rate, r plays a crucial role to reduce the magnitude of the waves.
Based on our analysis, without further precautions (i.e., more strict restrictions or efficient vaccination), it does not look possible to contain the outbreak with these strategies taken in the states.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in The New York Times (https://www.nytimes.com/interactive/2020/us/new-york-coronavirus-cases.html) and the codes used in this study are available in (https://github.com/ibrahimhalilaslan/Analyzing-the-effect-of-restrictions-on-the-COVID-19-outbreak-for-some-US-states).
References
Aslan IH, Demir M, Wise MM, Lenhart S (2022) Modeling COVID-19: Forecasting and analyzing the dynamics of the outbreak in Hubei and Turkey. Math Meth Appl Sci 45(10):6481–6494
Bourassa KJ, Sbarra DA, Caspi A, Moffitt TE (2020) Social distancing as a health behavior: County-level movement in the United States during the COVID-19 pandemic is associated with conventional health behaviors. Ann Behav Med 54(8):548–556
CDC COVID-19 RT (2020) Severe outcomes among patients with coronavirus disease 2019 (COVID-19)-U.S, February 12-March 16, 2020. MMWR Morb Mortal Wkly Rep 69(12):343–346
Chiu WA, Fischer R, Ndeffo-Mbah ML (2020) State-level needs for social distancing and contact tracing to contain COVID-19 in the United States. Nat Hum Behav 4(10):1080–1090
CNN (2020) This is where each state is during its phased reopening. https://edition.cnn.com/interactive/2020/us/states-reopen-coronavirus-trnd/. Accessed on Sept 2021
Courtemanche C, Garuccio J, Le A, Pinkston J, Yelowitz A (2020) Strong social distancing measures in the United States reduced the COVID-19 growth rate: Study evaluates the impact of social distancing measures on the growth rate of confirmed COVID-19 cases across the united states. Health Affairs 39(7):1237–1246
Fisher D, Heymann D (2020) Q &A: The novel coronavirus outbreak causing COVID-19. BMC Med 18(1):1–3
Glass DH (2020) European and US lockdowns and second waves during the COVID-19 pandemic. Math Biosci, p 108472
Grein J, Ohmagari N, Shin D, Diaz G, Asperges E, Castagna A, Feldt T, Green G, Green ML, Lescure F-X et al (2020) Compassionate use of remdesivir for patients with severe COVID-19. N Engl J Med
Guan W-J, Ni Z-Y, Hu Y, Liang W-H, Ou C-Q, He J-X, Liu L, Shan H, Lei C-L, Hui DS et al (2020) Clinical characteristics of 2019 novel coronavirus infection in China. MedRxiv
Leung K, Wu JT, Liu D, Leung GM (2020) First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: a modeling impact assessment. The Lancet 395(10233):1382–1393
Masters NB, Shih S-F, Bukoff A, Akel KB, Kobayashi LC, Miller AL, Harapan H, Lu Y, Wagner AL (2020) Social distancing in response to the novel coronavirus (COVID-19) in the United States. PLoS ONE 15(9):e0239025
Ngonghala CN, Iboi E, Eikenberry S, Scotch M, MacIntyre CR, Bonds MH, Gumel AB (2020) Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel coronavirus. Math Biosci, p 108364
Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, Agha M, Agha R (2020) ‘The socio-economic implications of the coronavirus and COVID-19 pandemic: a review. Int J Surg
Nishiura H, Linton NM, Akhmetzhanov AR (2020) Serial interval of novel coronavirus (COVID-19) infections. Int J Infect Dis
Renardy M, Eisenberg M, Kirschner D (2020) Predicting the second wave of covid-19 in Washtenaw County, MI. J Theor Biol 507:110461
Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R (2020) High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis 26(7):1470–1477
The New York Times (2020) New York coronavirus map and case count. https://www.nytimes.com/interactive/2020/us/new-york-coronavirus-cases.html. Accessed on Sept 2021
Waku J, Oshinubi K, Demongeot J (2022) Maximal reproduction number estimation and identification of transmission rate from the first inflection point of new infectious cases waves: Covid-19 outbreak example. Math Comput Simul 198:47–64
Wang X, Du Z, Huang G, Pasco RF, Fox SJ, Galvani AP, Pignone M, Johnston SC, Meyers LA (2020) Cocooning is essential to relaxing social distancing. MedRxiv
Wang X, Pasco RF, Du Z, Petty M, Fox SJ, Galvani AP, Pignone M, Johnston SC, Meyers LA (2020) Impact of social distancing measures on coronavirus disease healthcare demand, Central Texas, usa. Emerg Infect Dis 26(10):2361
World Health Organization (2015) Crude birth and death rate data by country. http://apps.who.int/gho/data/node.main.CBDR107?lang=en. Accessed on Sept 2021
Worldometer (2020) United States coronavirus cases, deaths, recovered. https://www.worldometers.info/coronavirus/country/us/. Accessed on Sept 2021
Wu J, Tang B, Bragazzi NL, Nah K, McCarthy Z (2020) Quantifying the role of social distancing, personal protection and case detection in mitigating COVID-19 outbreak in Ontario, Canada. J Math Ind 10(1):1–12
Author information
Authors and Affiliations
Contributions
M. D. and I. H. A. analyzed the data, performed the computations, and obtained model simulations with the guidance of S. L. All the authors contributed to the writing of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Demir, M., Aslan, I.H. & Lenhart, S. Analyzing the effect of restrictions on the COVID-19 outbreak for some US states. Theor Ecol 16, 117–129 (2023). https://doi.org/10.1007/s12080-023-00557-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12080-023-00557-1