
Abstract
Background
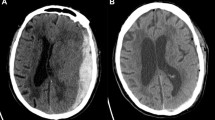
Little is known about the natural history of non-surgically managed subdural hematoma (SDH). The purpose of this study is to determine rates of adverse events after non-surgical management of SDH and whether these outcomes differ depending on traumatic versus nontraumatic etiology. A retrospective cohort study was conducted using administrative claims data on all emergency department visits and acute care hospitalizations at nonfederal facilities in California from 2005 to 2011, Florida from 2005 to 2012, and New York from 2006 to 2011. We included patients who were discharged home after hospitalization with a first-recorded diagnosis of SDH and no record of surgical hematoma evacuation.
Methods
Patients were followed for readmission with SDH, readmission for surgical SDH evacuation, and fatal readmission with SDH. Survival statistics and the log-rank test were used to compare rates of these adverse events after traumatic versus nontraumatic SDH. Multivariable Cox regression analysis was used to compare hazards for traumatic versus nontraumatic etiology while adjusting for age, sex, race, insurance status, presence of dementia, alcohol use, acquired abnormalities in coagulation, acquired abnormalities in platelet function, hypertension, atrial fibrillation, venous thromboembolism, ischemic stroke, coronary heart disease, and valvular disease.
Results
We identified 27,502 conservatively treated patients with SDH, of which 70.9 % were traumatic and 29.1 % nontraumatic. Compared to patients with traumatic SDH, patients with nontraumatic SDH had significantly higher rates of subsequent hospitalization with SDH (cumulative 90-day rates: 15.3 % [95 % CI 14.5–16.1 %] vs. 10.3 % [95 % CI 9.9–10.8 %]), surgical SDH evacuation (7.8 % [95 % CI 7.3–8.5 %] vs. 5.5 % [95 % CI 5.2–5.8 %]), and SDH-related in-hospital death (1.0 % [95 % CI 0.8–1.2 %] vs. 0.4 % [95 % CI 0.3–0.5 %]). In multivariable Cox regression analysis, nontraumatic etiology was associated with a higher hazard of readmission with SDH (HR 1.4; 95 % CI 1.3–1.5), surgery (HR 1.3; 95 % CI 1.2–1.4), and in-hospital mortality (HR 1.9; 95 % CI 1.4–2.5). Our findings were unchanged in sensitivity analyses that also adjusted for Elixhauser comorbidities.
Conclusions
Approximately one in eight patients with a conservatively managed SDH was readmitted with SDH within 90 days. A substantial proportion of these readmissions involved surgical hematoma evacuation. These outcomes occurred significantly more often after nontraumatic as compared to traumatic SDH.



Similar content being viewed by others

References
Frontera JA, Egorova N, Moskowitz AJ. National trend in prevalence, cost, and discharge disposition after subdural hematoma from 1998-2007. Crit Care Med. 2011;39(7):1619–25.
U.S. Census Bureau. Census QuickFacts. http://quickfacts.census.gov. Accessed March 10 2015.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167(13):1414–9.
Hylek EM, Singer DE. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med. 1994;120(11):897–902.
Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. http://hcupnet.ahrq.gov. Accessed March 10 2015.
Bullock MR, Chesnut R, Ghajar J, et al. Surgical management of acute subdural hematomas. Neurosurgery. 2006;58(3 Suppl):S16–24; discussion Si–iv.
Wong CW. Criteria for conservative treatment of supratentorial acute subdural haematomas. Acta Neurochir (Wien). 1995;135(1–2):38–43.
Dent DL, Croce MA, Menke PG, et al. Prognostic factors after acute subdural hematoma. J Trauma. 1995;39(1):36–42;discussion 42–33..
Croce MA, Dent DL, Menke PG, et al. Acute subdural hematoma: nonsurgical management of selected patients. J Trauma. 1994;36(6):820–6; discussion 826–827.
Mathew P, Oluoch-Olunya DL, Condon BR, Bullock R. Acute subdural haematoma in the conscious patient: outcome with initial non-operative management. Acta Neurochir (Wien). 1993;121(3–4):100–8.
Servadei F, Nasi MT, Cremonini AM, Giuliani G, Cenni P, Nanni A. Importance of a reliable admission Glasgow Coma Scale score for determining the need for evacuation of posttraumatic subdural hematomas: a prospective study of 65 patients. J Trauma. 1998;44(5):868–73.
Feliciano CE, De Jesus O. Conservative management outcomes of traumatic acute subdural hematomas. P R Health Sci J. 2008;27(3):220–3.
Seifi A, Asadi-Pooya AA, Carr K, et al. The epidemiology, risk factors, and impact on hospital mortality of status epilepticus after subdural hematomas in the United States. SpringerPlus. 2014;3:332.
Agency for Healthcare Research and Quality. HCUP methods series: methodological issues when studying readmissions and revisits using hospital administrative data. http://www.hcup-us.ahrq.gov/reports/methods/2011_01.pdf. Accessed March 10 2015.
De Coster C, Li B, Quan H. Comparison and validity of procedures coded With ICD-9-CM and ICD-10-CA/CCI. Med Care. 2008;46(6):627–34.
Son S, Yoo CJ, Lee SG, Kim EY, Park CW, Kim WK. Natural course of initially non-operated cases of acute subdural hematoma : the risk factors of hematoma progression. J Korean Neurosurg Soc. 2013;54(3):211–9.
Kim BJ, Park KJ, Park DH, et al. Risk factors of delayed surgical evacuation for initially nonoperative acute subdural hematomas following mild head injury. Acta Neurochir (Wien). 2014;156(8):1605–13.
Laviv Y, Rappaport ZH. Risk factors for development of significant chronic subdural hematoma following conservative treatment of acute subdural hemorrhage. Br J Neurosurg. 2014;28(6):733–8.
Agency for Healthcare Research and Quality. Clinical classification software for ICD-9-CM. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed March 10 2015.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27.
Coombs JB, Coombs BL, Chin EJ. Acute spontaneous subdural hematoma in a middle-aged adult: case report and review of the literature. J Emerg Med. 2014;47(3):e63–8.
Acknowledgments
The authors would like to thank Joshua Z. Willey, MD, MS for his thoughtful review of our manuscript. This study was supported by Grant K23NS082367 (Kamel) from the National Institute of Neurological Disorders and Stroke and a grant from the Michael Goldberg Stroke Research Fund (Kamel).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Morris, N.A., Merkler, A.E., Parker, W.E. et al. Adverse Outcomes After Initial Non-surgical Management of Subdural Hematoma: A Population-Based Study. Neurocrit Care 24, 226–232 (2016). https://doi.org/10.1007/s12028-015-0178-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-015-0178-x