
Abstract
Background
Altered cerebral vasomotor reactivity leading to vasospasm can be seen both in patients with primary headache disorders (PHD) and in patients with subarachnoid hemorrhage (SAH). The pathogenesis of vasospasm in post-SAH patients and in headache disorder sufferers may be related. To address this hypothesis, we analyzed a large cohort of SAH patients to determine whether a diagnosis of PHD predisposes to vasospasm, delayed cerebral ischemia, or worsened clinical outcome.
Methods
Prospectively collected data from patients enrolled in the SAH Outcomes Project between 1996 and 2006 were analyzed. Patients were segregated based on whether they had a diagnosis of PHD or not and were subsequently compared for differences in clinical and radiographic outcome.
Results
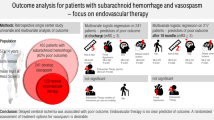
A total of 921 SAH patients were analyzed, 265 of which had a diagnosis of PHD. In total, symptomatic vasospasm was seen in 17 %, while angiographic vasospasm was seen in 28 %. Vasospasm rates were similar among patients with a PHD and in those without a PHD (p > 0.05). However, on multivariate analysis new ischemic infarcts were more common in patients with a PHD as compared to patients without a PHD (p = 0.015). Functional outcomes at 3 months were similar among PHD and non-PHD patients (p > 0.05).
Conclusion
A history of PHD is associated with an increased rate of ischemic infarcts during admission for SAH. Increased rates of vasospasm within small cerebral blood vessels may be implicated. Further studies are warranted to more closely link the mechanisms of vasospasm in PHD and SAH patients.
Similar content being viewed by others


References
de Rooij NK, Linn FH, van der Plas JA, Algra A, and Rinkel GJ. Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry. 2007;78(12):1365–72.
Weir B, Grace M, Hansen J, Rothberg C. Time course of vasospasm in man. J Neurosurg. 1978;48(2):173–8.
Rabinstein AA. The blood and the vessel: prediction of cerebral vasospasm after subarachnoid hemorrhage. Neurology. 2006;66(5):622–3.
Allen GS, Ahn HS, Preziosi TJ, et al. Cerebral arterial spasm: a controlled trial of nimodipine in patients with subarachnoid hemorrhage. N Engl J Med. 1983;308(11):619–24.
Hansen-Schwartz J. Cerebral vasospasm: a consideration of the various cellular mechanisms involved in the pathophysiology. Neurocrit Care. 2004;1(2):235–46.
Kassell NF, Sasaki T, Colohan AR, Nazar G. Cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Stroke. 1985;16(4):562–72.
Silberstein SD. Migraine pathophysiology and its clinical implications. Cephalalgia Int J Headache. 2004;24(Suppl 2):2–7.
Edvinsson L, Uddman R. Neurobiology in primary headaches. Brain Res Brain Res Rev. 2005;48(3):438–56.
Cole AJ, Aube M. Migraine with vasospasm and delayed intracerebral hemorrhage. Arch Neurol. 1990;47(1):53–6.
Frontera JA, Rundek T, Schmidt JM, et al. Cerebrovascular reactivity and vasospasm after subarachnoid hemorrhage: a pilot study. Neurology. 2006;66(5):727–9.
Solomon S, Lipton RB, Harris PY. Arterial stenosis in migraine: spasm or arteriopathy? Headache. 1990;30(2):52–61.
Masuzawa T, Shinoda S, Furuse M, Nakahara N, Abe F, Sato F. Cerebral angiographic changes on serial examination of a patient with migraine. Neuroradiology. 1983;24(5):277–81.
Garnic JD, Schellinger D. Arterial spasm as a finding intimately associated with the onset of vascular headach. A case report. Neuroradiology. 1983;24(5):273–6.
Viola S, Viola P, Litterio P, Buongarzone MP, Fiorelli L. Stroke risk and migraine: near-infrared spectroscopy study. Neurol Sci. 2012;33(Suppl 1):173–5.
Dietrich HH, Dacey RG Jr. Molecular keys to the problems of cerebral vasospasm. Neurosurgery. 2000;46(3):517–30.
The primary headaches. Cephalalgia Int J Headache. 2004;24:23–136.
Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968;28(1):14–20.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81–4.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–29.
Hijdra A, Brouwers PJ, Vermeulen M, van Gijn J. Grading the amount of blood on computed tomograms after subarachnoid hemorrhage. Stroke. 1990;21(8):1156–61.
Komotar RJ, Schmidt JM, Starke RM, et al. Resuscitation and critical care of poor-grade subarachnoid hemorrhage. Neurosurgery. 2009;64(3):397–410; discussion 410–1.
Raps EC, Rogers JD, Galetta SL, et al. The clinical spectrum of unruptured intracranial aneurysms. Arch Neurol. 1993;50(3):265–8.
de Falco FA. Sentinel headache. Neurol Sci. 2004;25(Suppl 3):S215–7.
Polmear A. Sentinel headaches in aneurysmal subarachnoid haemorrhage: what is the true incidence? A systematic review. Cephalalgia Int J Headache. 2003;23(10):935–41.
Dennis M, Warlow C. Migraine aura without headache: transient ischaemic attack or not? J Neurol Neurosurg Psychiatry. 1992;55(6):437–40.
Ertresvg JM, Stovner LJ, Kvavik LE, et al. Migraine aura or transient ischemic attacks? A five-year follow-up case-control study of women with transient central nervous system disorders in pregnancy. BMC Med. 2007;5:19.
Agostoni E, Rigamonti A. Migraine and cerebrovascular disease. Neurol Sci. 2007;28(Suppl 2):S156–60.
Del Sette M. Migraine and cerebrovascular risk. Neurol Sci. 2010;31(Suppl 1):S127–8.
Bousser MG, Welch KM. Relation between migraine and stroke. Lancet neurology. 2005;4(9):533–42.
Stewart WF, Wood C, Reed ML, Roy J, Lipton RB. Cumulative lifetime migraine incidence in women and men. Cephalalgia Int J Headache. 2008;28(11):1170–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ellis, J.A., Goldstein, H., Meyers, P.M. et al. Post-subarachnoid Hemorrhage Vasospasm in Patients with Primary Headache Disorders. Neurocrit Care 18, 362–367 (2013). https://doi.org/10.1007/s12028-012-9801-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9801-2