
Abstract
Asthma is probably the most common serious medical disorder that may complicate pregnancy. A third of pregnant women with asthma will experience worsening of their symptoms, a third will see improvement of their symptoms and a third will see no change. The primary goal is to maintain optimal control of asthma for maternal health and well-being as well as fetal maturation. Vital patient education should cover the use of controller medication, avoidance of asthma triggers and early treatment of asthma exacerbations. Proper asthma management should ideally be started in the preconception period. Since smoking is probably the most modifiable risk factor of asthma, pregnant woman should avoid active and passive smoking. Acute asthma exacerbation during the first trimester is associated with an increased risk of congenital malformations. Poorly controlled asthma is associated with low birth weight, preeclampsia, and preterm birth. Medications used for asthma control in the non-pregnant population are generally the same in pregnancy with a few exceptions. Inhaled corticosteroids (ICS) are the preferred controller therapy. Budesonide is the preferred ICS. Long-acting B-agonists (LABA) are the preferred add-on therapy to medium to high dose ICS. Major triggers for asthma exacerbations during pregnancy are viral infections and ICS nonadherence.
Similar content being viewed by others



Introduction
Asthma can significantly affect pregnancy outcomes if not well-controlled. The National Asthma Education and Prevention Program (NAEPP) [1] emphasizes that maintaining optimal control of asthma during pregnancy is important for the health and well-being of both the mother and her baby. Since asthma has a variable course during pregnancy, it is important to monitor closely to make adjustments in therapy. Pregnant women may be ambivalent about taking medications during pregnancy due to concerns about adverse effects on the fetus; however, the epidemiologic evidence is extremely strong in favor of using medications for asthma control. In fact, asthma control is especially crucial during first trimester when organogenesis takes place. Congenital malformations were significantly more common in asthmatic women who had an asthma exacerbation during the first trimester [2]. Overall, maternal asthma increases the risk of preeclampsia, congenital malformations, low birth weight, perinatal mortality, and preterm birth.
Preconception Counseling and Evaluation
By using national health surveys, data on the trend and prevalence of asthma in the preconception period has been reported. Among adult women of childbearing age, a two-fold increase in asthma prevalence from 2.9% to 5.8% occurred between 1976–1980 and 1988–1994. Among women aged 18 to 24, the increase was three-fold, from 1.8% to 6.0% [3]. In another study, approximately 4.1% of all pregnant women experienced an asthma attack in the preceding year (the preconception period) [4]. Preconception counseling is extremely important for women with asthma to clarify concerns about possible adverse effects on the fetus of the medications used to treat asthma and to ensure excellent asthma control, especially in the first trimester [5].
In 2006, the U.S. Center for Disease Control (CDC) published recommendations to improve health care for women before pregnancy and between pregnancies. The Pregnancy Risk Assessment Monitoring System (PRAMS) provided data on 18 behaviors and conditions that are relevant to preconception health and ten that are relevant to postpartum health. According to the PRAMS 2004 data, the prevalence during the preconception period was 23.2% for tobacco use, 6.9% for asthma, 13.1% for being overweight (body mass index [BMI]: 26.0–29.0), 21.9% for being obese (BMI: ≥29.0), and 30.3% for receiving prepregnancy health counseling [6]. Based on this report, many more women would benefit from preconception health counseling.
Before becoming pregnant, it is advised that women with asthma undergo a complete assessment of asthma control and be switched to preferred controller medications, as well as receive information on the importance of controlled asthma for fetal health. It may take several months to adjust medications and obtain good control of asthma, which is optimal prior to attempting conception. Since asthma has a variable course during pregnancy, it is important to discuss an asthma action plan during the preconception period [7]. Additional measures, like avoiding triggers for asthma exacerbations, can be instituted during the preconception period to minimize the severity or frequency of asthma symptoms during pregnancy, and thus decrease reliance on, and fetal exposure to, medications. Since a significant percentage of child-bearing age asthmatic women do not have asthma optimally controlled [4], primary care providers play a crucial role in counseling, treating, and referring them to specialists in a timely manner. Early pregnancy is a critical time in fetal development because the major part of organogenesis is over by 8 weeks of gestation. A significant number of pregnant women do not visit their obstetrician until several weeks or even months into pregnancy.
A study conducted by Nettleman et al. [8] reported that the recommended appointment times by obstetric clinics ranged from immediately upon discovery of pregnancy (approximately 4 weeks of gestation) to 10.6 weeks, or an average of 6.37 weeks. Twenty-five percent of clinics recommended a first appointment at ≥8 weeks of gestation. Thus, some women, even with full-coverage health insurance, may not have their first prenatal visit until near the end of the first trimester [8]. Primary care providers could help women in optimally managing their asthma during the preconception period and first few weeks of pregnancy. This could lead to better outcomes.
Epidemiology of Asthma During Pregnancy
Overall, the prevalence and morbidity of asthma are increasing, although mortality has gone down [9]. According to a large epidemiologic study by Kwon and colleagues [4], asthma was estimated to affect approximately 8.4–8.8% of pregnant women in the United States during 2000–2003. The study showed that only half of the women who took controller medication before pregnancy took them during pregnancy. In addition, only about half of women who had daily symptoms during pregnancy took any controller medication during pregnancy, reflecting poorly controlled asthma [4]. The need for emergency department care in the year prior to pregnancy was predictive of emergency visits during pregnancy [4]. Approximately 10% of women cared for by asthma specialists (a referral population) required emergency care or hospitalization for asthma during pregnancy [10]. Younger women and women with normal BMI were less likely to take controller medications regularly during pregnancy. Well-educated women, older women, and overweight or obese women were more likely to take them [4].
Carroll et al. [11] conducted a population—based cohort study of asthma-related morbidity in 4,315 black and white pregnant women enrolled in the Tennessee Medicaid Program, TennCare, from 1995 to 2001. This low-income population of pregnant asthmatics had high asthma-related morbidity. During pregnancy, 12.7% of women received rescue corticosteroids, 11.1% of women had asthma related ER visits, and 6.3% of women were hospitalized for asthma. Blacks were more likely than whites to receive a course of rescue corticosteroids, have an emergency department visit, or be hospitalized for asthma.
Chung et al. [12] conducted a historical cohort study in New Jersey between 1989 and 1993 (N = 556,597). The study looked at racial/ethnic disparities in the rate of asthma during pregnancy and examined insurance type, maternal education, and prenatal care as potential determinants of disparities. The study found that Medicaid and HealthStart enrollees were more often diagnosed with asthma symptoms in pregnancy than women with standard insurance. When such factors that reflected socioeconomic status were included in the analysis, the effect of race was decreased, and insurance type was determined to be the most important socioeconomic factor and accounted for most of the racial disparity [12].
Normal Physiology During Pregnancy
Multiple physiologic changes during pregnancy interact with the pathophysiology of asthma. During normal pregnancy there is a 20% increase in oxygen consumption and a 15% increase in the maternal metabolic rate. These demands are met by several physiologic changes during pregnancy [13].
Respiratory Changes During Pregnancy
To compensate for the increased oxygen demand of pregnancy, minute volume is increased by 40–50%. This hyperventilation is due to an increasing tidal volume. These changes are due to the stimulatory effect of progesterone on the respiratory center. The respiratory rate remains relatively unchanged during pregnancy. Therefore, tachypnea during pregnancy (respiratory rate >20) is an abnormal finding and should be further investigated. Hyperventilation leads to respiratory alkalosis that is compensated by metabolic acidosis. Typical blood gases in early pregnancy have a pH of 7.40–7.45, a pCO2 of 28–32 mmHg, and a pO2 of 106–110 mmHg (Table 1). The pO2 in the umbilical vein is lower than that in the placental arteriovenous capillary network due to the decrease in oxygen tension in transfer from the maternal placental channels to the fetal interfacing blood supply; thus, maternal hypoxemia (<95 mmHg) quickly results in a decreased oxygen supply to the fetus. Chronic hypoxemia could lead to restricted intrauterine growth and lowered birth weight. When interpreting maternal ABGs, a normal-looking pCO2 for a nonpregnant person actually reflects a maternal hypercapnic environment. A low pCO2 is essential for fetal acid–base balance and increased maternal pCO2 will cause fetal acidosis.
As the uterus enlarges, it pushes the diaphragm upward approximately 4–5 cm resulting in a reduction in the functional residual capacity (FRC) of about 18%. Because of this change, pregnant women more rapidly desaturate during hypopneic periods due to loss of reserve lung volume. Pregnancy does not change forced expiratory volume in one second (FEV1) or peak expiratory flow rate (PEFR). As in the general population, FEV1 and PEFR during pregnancy correlate well with asthma symptoms and exacerbations making them acceptable measurements to help monitor asthma control [14] (Table 2).
Cardiovascular Changes
Many of the significant physiologic changes occur in the cardiovascular system. Most of these changes occur in the first trimester, plateau in the second trimester, and peak again in the third trimester. The important changes to mention are a fall in systemic vascular resistance (SVR); a rise in heart rate (HR), an increase in cardiac output (CO), and a decrease in blood pressure (BP).
Falling of the SVR is likely due to peripheral arterial vasodilatation in early pregnancy mediated by progesterone [15]. The conversion of the uteroplacental circulation from high to low resistance flow acts to further reduce SVR. HR goes up as a compensatory mechanism to the falling SVR. BP also falls in early pregnancy because of the decrease in SVR. Fall in SVR and SBP reach a nadir at approximately 24 weeks of gestation and return to pre-pregnancy values at term. Fall in SVR also triggers a 40–50% increase in CO and the glomerular filtration rate.
Blood volume starts to rise during the first trimester and reaches a maximum by the third trimester that is 40–50% above the prepregnant state. Because plasma volume increases more than red cell mass, the hematocrit generally falls, resulting in the “physiologic anemia of pregnancy.”
Dyspnea During Pregnancy and Diagnosis of Asthma
Sixty to seventy percent of women experience dyspnea during the course of normal pregnancy. Dyspnea of pregnancy is often described as “air hunger” [16]. Dyspnea of pregnancy may be due to increased awareness of the “physiologic hyperventilation of pregnancy” [17]. Dyspnea of pregnancy is usually worse in the sitting position and is not exertional. It starts in the first or second trimester and peaks in the second trimester, then becomes relatively stable in third trimester. Normal dyspnea of pregnancy has a gradual onset. Dyspnea during pregnancy could be thus physiologic, but when it is accompanied by wheezing and/or coughing, it is likely to be caused by asthma. A diagnosis of asthma should be based on the history, the physical examination, and pulmonary function tests. Symptoms of asthma are wheezing, cough, chest tightness and dyspnea. Typically, asthma symptoms get worse in the presence of environmental stimuli and at night. Patients usually have a known history of asthma. On examination, the clinician may notice some expiratory wheezing. Spirometry may only be abnormal during an acute attack. The demonstration of a reduced FEV1 or FEV1/FVC ratio with a 12% or more improvement in FEV1 with bronchodilator confirms the diagnosis of asthma in pregnancy. Patients with asthma usually show reversibility on spirometry but some patients need oral corticosteroid therapy in order to show the reversibility [18]. Clinicians should consider the diagnosis of asthma when pregnant women present with intermittent shortness of breath that is at least partially reversible and when other causes of dyspnea are ruled out.
To estimate the prevalence of asthma as a cause of dyspnea during pregnancy, Bidad et al. [19] conducted a study in Tehran University, Iran, on 165 pregnant women who had been referred to the prenatal clinic for the complaint of dyspnea. Exclusion criteria included: any pulmonary disease other than asthma, gestational hypertension, major congenital anomalies, or multiple gestations. This study showed asthma as a cause of dyspnea in 38.8% cases, while dyspnea was determined to be physiologic in 36.4% of cases, and 24.8% of cases were diagnosed as having probable asthma (normal spirometry but symptoms and signs suggestive of asthma) [19]. Interestingly, this study showed that 25.4% of the women diagnosed as having definite asthma were newly identified and had no previous diagnosis of asthma by a physician.
Differential Diagnosis of Asthma During Pregnancy
Differential diagnosis of asthma during pregnancy should include the following:
-
1.
Dyspnea of pregnancy due to hyperventilation.
-
2.
Pulmonary embolism: Pregnancy is a procoagulable state, which can increase the risk for thromboembolism [15], particularly in those with additional risk factors like smoking.
-
3.
Amniotic fluid embolism.
-
4.
Bronchitis or pneumonia.
-
5.
Postnasal drip due to allergic rhinitis or sinusitis.
-
6.
Congestive heart failure, cardiomyopathy or pulmonary edema.
-
7.
Gastroesophageal reflux disease.
-
8.
Vocal cord dysfunction.
Diagnostic Work-up of Asthma During Pregnancy
A clinical impression of asthma should be confirmed by reversible airway obstruction on spirometry [18]. Women with a clinical presentation consistent with the new onset of asthma but whose pulmonary function tests failed to show the reversibility should be treated for asthma (e.g., normal FEV1 prior to bronchodilator and failure to improve further). Methacholine testing is contraindicated during pregnancy but can be done in the postpartum period if needed [20]. Smith et al. [21] compared formal allergy assessment (structured history and skin test) in making an accurate allergy diagnosis with a structured allergy history alone or the patient’s self-report. Self-reporting commonly resulted in misclassification of the allergy diagnosis with underestimation of dust mite and pollen sensitivities. A structured history obtained by the health care provider alone resulted in false positive rates for sensitivity to dust mites of 75%, grass pollen of 48%, tree pollen of 54%, cat of 32% and dog of 27% compared with formal allergy evaluation by an allergy specialist that included skin prick testing. Coming up with accurate allergy diagnosis is very important during pregnancy as most asthmatics are atopic and avoidance of allergen triggers is part of management. However, skin tests are not generally recommended during pregnancy because skin testing with potent antigens may rarely cause systemic allergic reactions [1, 20]. Instead, blood tests for specific IgE measurement can be utilized. Both positive and negative results would help the patient and clinician in coming up with better trigger avoidance strategies.
The Risk of Congenital Malformations and Low Birth Weight
Maternal asthma exacerbations have been found to be associated with a 50% increased risk of congenital malformations [2].
According to a study published by Blais et al. in 2010 [22], the prevalence of any congenital malformation was 9.5% and 7.5% for women with and without asthma, respectively. Another study by Blais et al. from 2008 [2] showed the prevalence of malformations was 12.8% and 8.9%, respectively, for women who had and those who did not have an asthma exacerbation during pregnancy. The risk seems even higher for women who did not fill any prescriptions for oral corticosteroids during pregnancy, with a two-fold increase for women with an exacerbation during the first trimester who did not have oral corticosteroids on hand. Filling a prescription for an oral corticosteroid does not mean that the individual necessarily used it, but may indicate that the patient has excellent medical care with an asthma action plan that includes an oral corticosteroid if needed.
In a meta-analysis, Murphy et al. found that women with an asthma exacerbation during pregnancy are at increased risk of having low-birth-weight babies when compared to women without asthma [23]. Severe and poorly controlled asthma may cause prematurity, increased need for Cesarean section delivery, preeclampsia, growth restriction and increased maternal mortality and morbidity [24, 25]. Bakhireva et al. [26] studied a voluntary sample of 486 asthmatic pregnant women and 486 nonasthmatic pregnant controls. The study findings suggest that overall perinatal outcomes for women with well-controlled asthma during pregnancy are comparable to those of nonasthmatic pregnant women.
Effect of Pregnancy on Asthma
Pregnancy can influence the disease course of asthma. The risk of asthma exacerbations requiring intervention in pregnant women is higher than in nonpregnant female asthmatics [10]. About 18% of all pregnant women had at least one ED visit [10] and up to 62% of women with asthma exacerbations required hospitalization in one study [27]. Kircher et al. [28] noted improvement of asthma control during pregnancy in 33.6%, worsening in 36.3%, unchanged control in 26.4%, and the course was uncertain in 3.7% of women. Worsening of asthma during pregnancy is related to the baseline asthma severity. Schatz et al. [29] enrolled 1,739 pregnant asthmatics before 26 weeks of gestation and classified them into mild, moderate, and severe disease groups. They noted correlation between severity of asthma and outcome of the pregnancy, with 51.9% of those in the severe group having an asthma exacerbation, 25.7% of the moderate group, and 12.6% of the mild group. The variable course of asthma was also reflected in this cohort, with 30% of pregnant women whose asthma was classified as mild at the beginning switched to either the moderate or severe group, 23% of the initially moderate-severe asthma patients reclassified as mild later in pregnancy. These findings emphasize the need for close follow–up of all pregnant asthmatics. The same group previously reported that pregnant women were more likely to get asthma exacerbations between 29 and 36 weeks and likely to have less frequent and less severe attacks during the last 4 weeks of pregnancy [30]. With successive pregnancies, asthma was noted to have the same course as experienced in previous pregnancies [30].
According to a study done by Belanger et al., the pre-pregnancy severity of asthma and use of medication according to Global Initiative for Asthma guidelines had more effect than other factors like age, race, BMI, parity, and smoking on the course of asthma during pregnancy [31–32]. Women with only intermittent asthma who had appropriate treatment got the most benefit: a 62% decreased risk for worsening asthma. Women with mild persistent asthma also showed a 52% decreased risk of worsened asthma; however, if asthma medications were stopped, even mild asthma was at risk to become severe and poorly-controlled [32]. This is further support for the American College of Obstetricians and Gynecologists' position that asthma medications be continued during pregnancy for the well-being of mother and fetus [9].
Asthma Management During Pregnancy
Successful management of asthma depends on a comprehensive approach. To achieve adequate control of asthma, EPR-3 recommends routine monitoring of asthma control during all prenatal visits, use of albuterol (salbutamol outside of the United States) as the preferred SABA when needed; use of inhaled corticosteroids (ICS), and specifically budesonide, as the preferred long-term controller medication, and use of intranasal corticosteroids to treat concomitant allergic rhinitis, if present [18].
The Expert Panel Report of the Working Group on Asthma and Pregnancy—2004 Update stressed four important components of asthma management [1].
-
1.
Objective monitoring of maternal lung function and fetal well-being as guide to the therapy.
Asthma control should be assessed according to the frequency and severity of symptoms and functional limitation, frequency of rescue inhaler use, history of exacerbations requiring oral corticosteroid therapy, emergency department visits, or hospitalizations (Table 3) [1, 20]. Patients often underestimate the severity of their asthma symptoms and may have difficulty in recognizing early signs of worsening symptoms of asthma. Asthma symptoms are usually greatest at night and in the morning. Women who are having frequent symptoms should monitor PEFR twice a day: upon awakening and 12 h later. At office visits, spirometry should be the preferred method of assessing asthma control [20]. Schatz et al. [33] reported that lower function (FEV1) during pregnancy is associated with an increased incidence of gestational hypertension and prematurity. Early ultrasound of the fetus, between 12 and 20 weeks gestation, is recommended to determine the gestational age as accurately as possible and to provide a benchmark against which future fetal growth can be measured. Pregnant asthmatics should have follow-up in the clinic once every 1–2 weeks until asthma is controlled and then monthly throughout pregnancy (Table 3).
-
2.
Patient education. All women should be educated about the interrelationship of asthma and pregnancy and be made aware of complications of poorly controlled asthma (recommended resource: March of Dimes website www.marchofdimes.com/complications_asthma.html). Women should be taught about initial home management of asthma exacerbations according to a treatment plan (Table 4) [1], technique of using an inhaler, adherence to medications, and control of environmental triggers. Asthma management during pregnancy is most successful when a woman receives regular care, and follows her treatment plan. A study done by Murphy et al. [34] indicated a significant improvement in asthma self-management skills following the implementation of an educational program. Providing information to women on asthma education resources would be very useful. Providers should inform patients that the outcome is most favorable for the mother and baby when asthma is well-controlled during pregnancy. Also, pregnant asthmatic women should be informed that it is safer to take asthma medications than it is to have asthma that is not optimally controlled. Women who smoke must be informed of the adverse effects of smoking on the fetus and on asthma control.
Table 4 Pregnancy categories for frequently prescribed and over the counter asthma and allergy medications -
3.
Control of environmental triggers and co-morbid conditions of asthma. Avoiding or controlling asthma triggers can reduce symptoms. Seventy to eighty percent patients with asthma have positive skin tests for common allergens, including animal dander, dust mites, cockroach, pollen, and molds, for which environmental control measures may be helpful (Table 5) [1, 20, 25]. Immunotherapy should not be started during pregnancy [35]. If the patient is on maintenance or near-maintenance allergen immunotherapy and not having any adverse reactions to the injections, and having clinical benefit, continuation of immunotherapy is recommended without any further increase in dose. Dose reduction may be considered to further reduce the risk of anaphylaxis. All pregnant asthmatic women should be up to date on influenza and pneumococcal vaccines as respiratory infections are frequent triggers for asthma exacerbation. Live vaccines should be avoided during pregnancy. Non-immunologic triggers that should be avoided include tobacco and marijuana smoke, air pollution, and in some sensitive patients, high levels of sulfites in foods, aspirin or NSAIDs. Beta blockers should be avoided. Patients with exercise-induced asthma should be encouraged to take SABA about 10 min before the exercise. Co-morbid conditions that can potentially cause asthma to flare up such as GERD or allergic rhinitis should be treated appropriately.
Table 4 Management of asthma exacerbation during pregnancy and lactation: home treatment or asthma action plan -
4.
Pharmacotherapy. About half of asthmatic women stop their asthma controller medications during pregnancy; non-adherence is consequently a major cause of worsening asthma symptoms. Medication adherence can be improved by education that highlights the benefits to fetal and maternal health when asthma control medications are continued. Since the recent data on safety of ICS during pregnancy is reassuring, health care providers should encourage pregnant women to continue asthma medications throughout pregnancy [36]. If asthma is not controlled despite consideration of the nonpharmacological strategies stated above, it is recommended to increase therapy by one step (Fig. 1). A two-step increase and/or a course of oral corticosteroids are recommended for women with very poorly controlled asthma. Most medications used in non-pregnant women can also be used in pregnancy, but there are a few exceptions (Tables 6 and 7). Zileuton should not used during pregnancy. On step 3 therapy, medium strength ICS (pregnancy category B) are preferred over low-potency ICS + LABA (category C). Studies show that pregnant women with poorly controlled asthma symptoms use more rescue medications and less controller medication. Louik et al. conducted a study on a random sample of 3,609 mothers of nonmalformed infants born in Massachusetts between 1998 and 2006. LTRA were used by only 3.4% of asthmatic women; ICS use increased only from 19% during 1997–1999 to 23.3% in 2003–2005 but use of beta(2) agonists exceeded 50% in both periods. Less than 40% of women with poorly controlled asthma reported use of controller medications [37], thus there is much room for improvement in pharmacotherapy.
Fig. 1 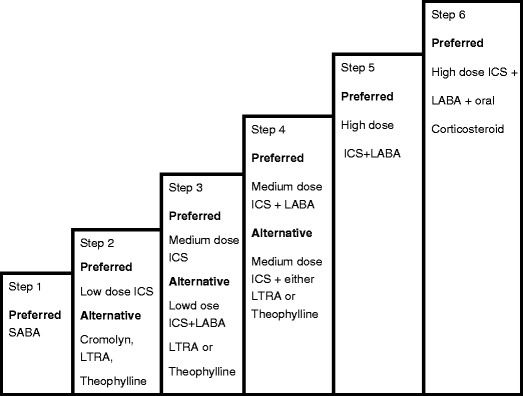
Stepwise approach for managing asthma in pregnant women SABA short acting beta agonist; ICS inhaled corticosteroid; LABA long acting beta agonist, LTRA Leukotriene receptor antagonist Data adopted and modified from National Heart, Lung and Blood institute, National Asthma Education and Prevention Program. Expert panel report 3 Guidelines for the diagnosis and management of asthma 2007 update [1].
Table 5 Summary of control measures for environmental factors that can make asthma worse Table 7 US Food and Drug Administration pregnancy category for fetal risk

Management of Asthma Exacerbation During Pregnancy
In addition to preventing maternal and fetal hypoxia, the goals of acute asthma exacerbation treatment in pregnant patients should be the same as in nonpregnant patients [38]. Intense fetal and maternal monitoring is recommended. Blood gases should be interpreted with caution. A pCO2 >35 mmHg and/or a pO2 <70 mmHg during an acute asthma exacerbation represents severe compromise. Maternal oxygen saturation should be kept above 95% if possible for fetal health. Prior to discharge from the ED or hospital, it is advisable to do ambulatory pulse oximetry to make sure pregnant women do not desaturate with their day-to-day activities [39]. Blood sugars should be monitored closely in pregnant women receiving systemic corticosteroids because of the significant effects of hyperglycemia on the fetus.
Obstetrical Care
Women with asthma that is not well controlled may benefit from increased fetal surveillance. During labor and delivery, only 10% to 20% of asthmatic women have symptoms [40]. Women who required systemic corticosteroids in the past year may need stress-dose corticosteroid during this period, for example, 100 mg hydrocortisone IV every 8 h during labor and delivery and for 24 h post-partum. Clinicians should try to maintain adequate hydration. If preterm labor occurs, tocolytic therapy may be considered. Magnesium sulfate and terbutaline are preferred because of their bronchodilatory effects, but indomethacin may induce bronchospasm, especially in aspirin sensitive patients, and thus should be avoided. Dinoprost, ergotamine, and other ergot derivatives may cause bronchospasm, especially when used in combination with general anesthesia and should be avoided in asthmatic patients during delivery [39]. Oxytocin is the drug of choice for induction of labor and control of postpartum hemorrhage [10]. If prostaglandin treatment is needed, E1 or E2 can be used. Narcotics (besides fentanyl) release histamine and may worsen bronchospasm. Analgesia should be maintained during labor and delivery as pain is associated with asthma exacerbations; analgesia should not compromise patient’s respiratory status [20]. Lumbar epidural analgesia is preferred for pain control. If a Cesarean section needed, preanesthetic atropine and glycopyrrolate may augment bronchodilation and ketamine is a preferred anesthetic agent [1]. During pregnancy, reduced FRC and increased O2 consumption may lower O2 reserve. This can cause a precipitous drop in the PaO2 due to apnea at the time of intubation. Preoxygenation of pregnant women with 100% oxygen is helpful before intubation and cricoid pressure must be maintained to prevent gastric content aspiration.
In most women, asthma reverts back to the pre-pregnancy level of severity within 3 months after delivery [30]. The NAEPP reports no contraindication for the use of prednisone, theophylline, antihistamines, ICS or inhaled beta-2 agonists during breast feeding [1]. Patients should be encouraged to continue their asthma medications during the postpartum.
Influenza Infection During Pregnancy
Pandemic novel influenza A (H1N1) infection is a substantial threat to pregnant women. Miller et al. [41] conducted an observational study on 18 pregnant women who were admitted to the hospital with the diagnosis of H1N1 from May 18 to June 24, 2009. Demographically, 11% were health care workers, 83% were Black, 11% were Hispanics and 6% were White. Half of the pregnant women presented with gastrointestinal or abdominal complaints, and 72% met the criteria for sepsis. The most common co-morbid conditions were asthma, diabetes, sickle cell disease, smoking, and obesity [41–43]. Admitted pregnant women with H1N1 were found to be at increased risk for fetal distress, premature birth, emergency Cesarean section, and fetal death. A reverse transcriptase polymerase chain reaction detection assay was reported superior to the antigen-based rapid test for diagnosis [44]. Antiviral treatment with oseltamivir within 2 days of symptom onset was associated with an 84% reduction in the odds of admission to an intensive care unit [41, 45]. In future pandemics, efforts should be made to ensure vaccinations and antiviral drugs are promptly provided to pregnant women, especially in primary care settings. Special efforts to educate asthmatic women of child-bearing age on the importance of annual influenza vaccination are recommended.
Tobacco Smoking in the Pregnant Asthmatic
Smoking during pregnancy is a significant risk factor for poor perinatal outcome, including low birth weights, premature birth, and infant mortality [46]. In a large study of pregnant asthmatics, Newman et al. [47] found that active smokers had significantly more days with asthma symptoms as well as small for gestational age infants and lower mean birth weight compared to nonsmokers and those with passive smoke exposure. During pregnancy, many women will be highly motivated to quit smoking and will be receptive to targeted interventions that will help them achieve success. The U.S. Preventive Services Task Force (USPSTF) recommends asking all pregnant women during prenatal visits about tobacco use and providing augmented, pregnancy-tailored counseling for those who smoke [48]. The USPSTF has concluded that the use of nicotine replacement products or other pharmaceuticals for smoking cessation aids during pregnancy and lactation have not been sufficiently evaluated to determine their efficacy or safety [48]. Unfortunately, within one year of delivery, over half of women who quit smoking will resume the habit.
Maternal Factors that Affect the Incidence of Asthma in Offspring
-
1.
Overweight and obesity in the pre-pregnancy period. A population-based study of children (N = 1971) born in U.S. cities in 1998–2000 showed children had a 52% higher risk of having an asthma diagnosis by age 3 if their mothers were obese in the pre-pregnancy period [49]. A separate study that was done in the Netherlands corroborated these results. This was a prospective birth cohort study of 3,963 children and their mothers with follow-up for 8 years; the study showed that the child’s risk of asthma increased with increasing maternal BMI in children with a predisposition for asthma (one parent with allergy or asthma), irrespective of the child’s BMI. Maternal obesity (BMI ≥30) before pregnancy (versus normal weight) was more strongly associated with asthma at 8 years than maternal moderate overweight (BMI >25 and <30) (versus normal weight). The author postulated this increased incidence of asthma could be from increased inflammation in obese/overweight women resulting in an intergenerational linkage of obesity and asthma. These findings stress the importance of counseling patients to reach and maintain an ideal body weight in the preconception period.
-
2.
Control and severity of asthma during pregnancy. Martel et al. [50] conducted a cohort study on 8,226 children of asthmatic mothers and found that compared with children of mild, well-controlled asthmatic mothers, children whose mothers had moderate-to-severe, uncontrolled asthma during pregnancy had an increased incidence of asthma.
-
3.
Maternal diet and childhood asthma. There is interest in more complete characterization of environmental influences on the development of childhood asthma, including maternal diet, however, there is no data yet of sufficient strength to change current practice. Willers et al. [51] conducted a study of 4,146 pregnant women (1,327 atopic and 2,819 nonatopic) and followed their children over 8 years. The study showed no associations between maternal vegetable, fish, egg, milk, or milk products consumption during pregnancy and childhood asthma symptoms until age of 8, except tree nuts and peanuts or their products. The study indicated an increased risk of asthma in children with maternal daily consumption of nut products during pregnancy [51]. A major limitation of the study was that the questionnaire did not have information on specific foods or portion sizes.
-
4.
Tobacco smoking. Karmaus et al. [52] assessed the joint effect of a risk triad involving recurrent lower respiratory tract infections (RLRTI), maternal smoking during pregnancy, and breast feeding for less than 3 months. This study showed a stronger association of the above triad with asthma at ages 4 and 10 compared to other risk triads (like maternal smoking, breast feeding less than 3 months but no RLRTI) (RR was 3.1). The authors concluded that a proportion of asthma cases in childhood can be prevented by avoiding smoking during pregnancy, promoting breast feeding and avoidance of RLRTI in early childhood [52]. Midodzi et al. [53] looked at risk factors for the development of asthma in preschool children (2–5 years). The study reported maternal smoking during pregnancy, male sex, single parent, low birth weight, childhood allergies, parental atopy, and low socioeconomic status as independent risk factors for development of childhood asthma. The hazard ratio for maternal smoking (more than five cigarettes a day) was 1.34. Protective factors including breast feeding more than 3 months, frequent upper respiratory infection, older siblings, early day care attendance, and living in rural areas [53].
-
5.
Maternal anxiety. Symptoms of maternal anxiety as an indicator of stress during fetal life may increase the risk of asthma in childhood. Cookson et al. [54] conducted a longitudinal study on 5,810 children. They found a higher likelihood of asthma at age 7.5 years (odds ratio, 1.64; 95% CI, 1.25–2.17) in children of mothers in the highest compared with lowest quartile of anxiety scores at 32 weeks of gestation [54].
Conclusion
Asthma is a common morbidity during pregnancy but can be well-controlled in most cases. The consequences of poorly-controlled asthma are potentially severe and devastating. Increased awareness of the critical importance of asthma control by physicians who care for women of child-bearing age may improve outcomes, primarily through patient education as to the importance of medication adherence, keeping in mind that about half of women deliberately stop their asthma medications in pregnancy. The management of asthma during pregnancy should be based upon objective assessment, trigger avoidance, patient education, and step therapy. Poorly-controlled asthma is a greater risk to the fetus than asthma medications [1]. It is recommended that pregnant asthmatics have follow-up every 1–2 weeks until asthma control is achieved and then, at least every month throughout the pregnancy [20]. All asthma medications should be continued during pregnancy and lactation.
References
NAEPP expert panel report (2005) Managing asthma during pregnancy: recommendations for pharmacologic treatment—2004 update. J Allergy Clin Immunol 115(1):34–46
Blais L, Forget A (2008) Asthma exacerbations during the first trimester of pregnancy and the risk of congenital malformations among asthmatic women. J Allergy Clin Immunol 121(6):1379–1384, 84 e1
Kwon HL, Belanger K, Bracken MB (2003) Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol 13(5):317–324
Kwon HL, Triche EW, Belanger K, Bracken MB (2006) The epidemiology of asthma during pregnancy: prevalence, diagnosis, and symptoms. Immunol Allergy Clin North Am 26(1):29–62
Grubbs S, Brundage SC (2002) Preconception management of chronic diseases. J S C Med Assoc 98(6):270–276
D’Angelo D, Williams L, Morrow B et al (2007) Preconception and interconception health status of women who recently gave birth to a live-born infant—Pregnancy Risk Assessment Monitoring System (PRAMS), United States, 26 reporting areas, 2004. MMWR Surveill Summ 56(10):1–35
Cragan JD, Friedman JM, Holmes LB et al (2006) Ensuring the safe and effective use of medications during pregnancy: planning and prevention through preconception care. Matern Child Health J 10(5 Suppl):S129–S135
Nettleman MD, Brewer J, Stafford M (2010) Scheduling the first prenatal visit: office-based delays. Am J Obstet Gynecol 203(3):207, e1–e3
Dombrowski MP, Schatz M (2008) ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 90, February 2008: asthma in pregnancy. Obstet Gynecol 111(2 Pt 1):457–464
Hanania NA, Belfort MA (2005) Acute asthma in pregnancy. Crit Care Med 33(10 Suppl):S319–S324
Carroll KN, Griffin MR, Gebretsadik T et al (2005) Racial differences in asthma morbidity during pregnancy. Obstet Gynecol 106(1):66–72
Chung KD, Demissie K, Rhoads GG (2004) Asthma in pregnancy—its relationship with race, insurance, maternal education, and prenatal care utilization. J Natl Med Assoc 96(11):1414–1421
Nelson-Piercy C, Waldron M, Moore-Gillon J (1994) Respiratory disease in pregnancy. Br J Hosp Med 51(8):398–401
Hardy-Fairbanks AJ, Baker ER (2010) Asthma in pregnancy: pathophysiology, diagnosis and management. Obstet Gynecol Clin North Am 37(2):159–172
Carlin A, Alfirevic Z (2008) Physiological changes of pregnancy and monitoring. Best Pract Res Clin Obstet Gynaecol 22(5):801–823
Simon PM, Schwartzstein RM, Weiss JW et al (1990) Distinguishable types of dyspnea in patients with shortness of breath. Am Rev Respir Dis 142(5):1009–1014
Gilbert R, Auchincloss JH Jr (1966) Dyspnea of pregnancy. Clinical and physiological observations. Am J Med Sci 252(3):270–276
Urbano FL (2008) Review of the NAEPP 2007 Expert Panel Report (EPR-3) on Asthma Diagnosis and Treatment Guidelines. J Manag Care Pharm 14(1):41–49
Bidad K, Heidarnazhad H, Pourpak Z et al (2010) Frequency of asthma as the cause of dyspnea in pregnancy. Int J Gynaecol Obstet
Schatz M, Dombrowski MP (2009) Clinical practice. Asthma in pregnancy. N Engl J Med 360(18):1862–1869
Smith HE, Hogger C, Lallemant C et al (2009) Is structured allergy history sufficient when assessing patients with asthma and rhinitis in general practice? J Allergy Clin Immunol 123(3):646–650
Blais L, Kettani FZ, Elftouh N, Forget A (2010) Effect of maternal asthma on the risk of specific congenital malformations: A population-based cohort study. Birth Defects Res A Clin Mol Teratol 88(4):216–222
Murphy VE, Clifton VL, Gibson PG (2006) Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax 61(2):169–176
Dombrowski MP (2006) Asthma and pregnancy. Obstet Gynecol 108(3 Pt 1):667–681
Dombrowski MP, Schatz M (2010) Asthma in pregnancy. Clin Obstet Gynecol 53(2):301–310
Bakhireva LN, Schatz M, Jones KL, Chambers CD (2008) Asthma control during pregnancy and the risk of preterm delivery or impaired fetal growth. Ann Allergy Asthma Immunol 101(2):137–143
Wendel PJ, Ramin SM, Barnett-Hamm C et al (1996) Asthma treatment in pregnancy: a randomized controlled study. Am J Obstet Gynecol 175(1):150–154
Kircher S, Schatz M, Long L (2002) Variables affecting asthma course during pregnancy. Ann Allergy Asthma Immunol 89(5):463–466
Schatz M, Dombrowski MP, Wise R et al (2003) Asthma morbidity during pregnancy can be predicted by severity classification. J Allergy Clin Immunol 112(2):283–288
Schatz M, Harden K, Forsythe A et al (1988) The course of asthma during pregnancy, post partum, and with successive pregnancies: a prospective analysis. J Allergy Clin Immunol 81(3):509–517
Kroegel C (2007) Global Initiative for Asthma Management and Prevention—GINA 2006. Pneumologie 61(5):295–304
Belanger K, Hellenbrand ME, Holford TR, Bracken M (2010) Effect of pregnancy on maternal asthma symptoms and medication use. Obstet Gynecol 115(3):559–567
Schatz M, Dombrowski MP, Wise R et al (2006) Spirometry is related to perinatal outcomes in pregnant women with asthma. Am J Obstet Gynecol 194(1):120–126
Murphy VE, Gibson PG, Talbot PI et al (2005) Asthma self-management skills and the use of asthma education during pregnancy. Eur Respir J 26(3):435–441
Cox L, Nelson H, Lockey R, et al (2011) Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol 127:S1–55
Blais L, Beauchesne MF, Rey E et al (2007) Use of inhaled corticosteroids during the first trimester of pregnancy and the risk of congenital malformations among women with asthma. Thorax 62(4):320–328
Louik C, Schatz M, Hernandez-Diaz S et al (2010) Asthma in pregnancy and its pharmacologic treatment. Ann Allergy Asthma Immunol 105(2):110–117
Cydulka RK (2006) Acute asthma during pregnancy. Immunol Allergy Clin North Am 26(1):103–117
Powrie RO, Larson L, Miller M (2006) Managing asthma in expectant mothers. Treat Respir Med 5(1):1–10
Gluck JC, Gluck PA (2006) The effect of pregnancy on the course of asthma. Immunol Allergy Clin North Am 26(1):63–80
Miller AC, Safi F, Hussain S et al (2010) Novel influenza A(H1N1) virus among gravid admissions. Arch Intern Med 170(10):868–873
Yates L, Pierce M, Stephens S et al (2010) Influenza A/H1N1v in pregnancy: an investigation of the characteristics and management of affected women and the relationship to pregnancy outcomes for mother and infant. Health Technol Assess 14(34):109–182
Skret-Magierlo J, Florek A, Skret A et al (2010) Severe A/H1N1 influenza in four pregnant women in Podkarpacie Province of Poland. Ginekol Pol 81(3):227–231
Farley MM (2010) 2009 H1N1 influenza: a twenty-first century pandemic with roots in the early twentieth century. Am J Med Sci 340(3):202–208
Jain S, Kamimoto L, Bramley AM et al (2009) Hospitalized patients with 2009 H1N1 influenza in the United States, April–June 2009. N Engl J Med 361(20):1935–1944
Einarson A, Riordan S (2009) Smoking in pregnancy and lactation: a review of risks and cessation strategies. Eur J Clin Pharmacol 65(4):325–330
Newman RB, Momirova V, Dombrowski MP et al (2010) The effect of active and passive household cigarette smoke exposure on pregnant women with asthma. Chest 137(3):601–608
(2009) Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women: U.S. Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med 150(8):551–555
Reichman NE, Nepomnyaschy L (2008) Maternal pre-pregnancy obesity and diagnosis of asthma in offspring at age 3 years. Matern Child Health J 12(6):725–733
Martel MJ, Rey E, Beauchesne MF et al (2009) Control and severity of asthma during pregnancy are associated with asthma incidence in offspring: two-stage case-control study. Eur Respir J 34(3):579–587
Willers SM, Wijga AH, Brunekreef B et al (2008) Maternal food consumption during pregnancy and the longitudinal development of childhood asthma. Am J Respir Crit Care Med 178(2):124–131
Karmaus W, Dobai AL, Ogbuanu I et al (2008) Long-term effects of breastfeeding, maternal smoking during pregnancy, and recurrent lower respiratory tract infections on asthma in children. J Asthma 45(8):688–695
Midodzi WK, Rowe BH, Majaesic CM et al (2010) Early life factors associated with incidence of physician-diagnosed asthma in preschool children: results from the Canadian Early Childhood Development cohort study. J Asthma 47(1):7–13
Cookson H, Granell R, Joinson C et al (2009) Mothers’ anxiety during pregnancy is associated with asthma in their children. J Allergy Clin Immunol 123(4):847–853, e11
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vatti, R.R., Teuber, S.S. Asthma and Pregnancy. Clinic Rev Allerg Immunol 43, 45–56 (2012). https://doi.org/10.1007/s12016-011-8277-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12016-011-8277-8