Abstract
Objectives
New-onset post-operative atrial fibrillation (POAF) is a frequent adverse event following major thoracic surgery and is associated with increased risk of perioperative morbidity, length of stay and stroke. It is managed initially with rate and rhythm control therapy; however, optimal duration and the need for anticoagulation are poorly understood. This study aims to assess practice variation regarding POAF management and duration.
Methods
This retrospective, single-center cohort study included patients who underwent major thoracic surgery and developed POAF between 2008 and 2017, managed with rate and rhythm control therapy alone. Demographic, clinical, and surgical variables/outcomes, POAF management, and incidence of POAF recurrence in the 30-day post-operative period were collected. Chi-square and T-tests determined significance.
Results
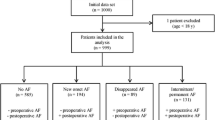
Of 2054 patients undergoing thoracic surgery, 155 (75%) patients developed POAF. Different rate and rhythm control agents were used, most commonly metoprolol. 107 (69%) continued rate and rhythm control therapy upon hospital discharge for a mean of 56 days. Among the 48 patients with discontinuation of rate and rhythm control therapy on discharge, none demonstrated recurrence of POAF; in contrast to 3 of 107 patients who continued on therapy. Among patients with CHA2DS2-VASc score ≥ 2, 15% were prescribed anticoagulation on discharge.
Conclusions
Use of rate and rhythm control therapy and anticoagulation for POAF is significantly varied in practice. Many patients are not continued on rate and rhythm control after hospital discharge, which does not appear to impact risk of POAF recurrence. Further research to inform guidelines for POAF management, including therapy duration and indications for anticoagulation is warranted.

Similar content being viewed by others

References
Joshi KK, Tiru M, Chin T, et al. Post-operative atrial fibrillation in patients undergoing non-cardiac non-thoracic surgery: a practical approach for the hospitalist. Postoperative. 1995;2016(43):235–44. https://doi.org/10.1080/21548331.2015.1096181.
Imperatori A, Mariscalco G, Riganti G, Rotolo N, Conti V, Dominioni L. Atrial fibrillation after pulmonary lobectomy for lung cancer affects long-term survival in a prospective single-center study. J Cardiothorac Surg. 2012;7:4. https://doi.org/10.1186/1749-8090-7-4.
Gialdini G, Nearing K, Bhave PD, et al. Perioperative atrial fibrillation and the long-term risk of ischemic stroke. J Am Med Assoc. 2014;312(6):616–22. https://doi.org/10.1001/jama.2014.9143.
Butt JH, Olesen JB, Havers-Borgersen E, et al. Risk of thromboembolism associated with atrial fibrillation following noncardiac surgery. J Am Coll Cardiol. 2018;72(17):2027–36. https://doi.org/10.1016/j.jacc.2018.07.088.
Lee JK, Klein GJ, Krahn AD, et al. Rate-control versus conversion strategy in postoperative atrial fibrillation: a prospective, randomized pilot study. Am Heart J. 2000;140(6):871–7. https://doi.org/10.1067/mhj.2000.111104.
Smith H, Yeung C, Gowing S, et al. A review and analysis of strategies for prediction, prevention and management of post-operative atrial fibrillation after non-cardiac thoracic surgery. J Thorac Dis. 2018;10(Suppl 32):S3799–808. https://doi.org/10.21037/jtd.2018.09.144.
Frendl G, Sodickson AC, Chung MK, et al. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. Executive summary. J Thorac Cardiovasc Surg. 2014;148(3):772–91. https://doi.org/10.1016/j.jtcvs.2014.06.037.
Alonso-Coello P, Cook D, Xu SC, et al. Predictors, prognosis, and management of new clinically important atrial fibrillation after noncardiac surgery: a prospective cohort study. Anesth Analg. 2017;125(1):162–9. https://doi.org/10.1213/ANE.0000000000002111.
Lin MH, Kamel H, Singer DE, Wu YL, Lee M, Ovbiagele B. Perioperative/postoperative atrial fibrillation and risk of subsequent stroke and/or mortality: a meta-analysis. Stroke. 2019;50(6):1364–71. https://doi.org/10.1161/STROKEAHA.118.023921.
Olesen JB, Torp-Pedersen C, Hansen ML, Lip GYH. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0–1: a nationwide cohort study. Thromb Haemost. 2012;107(6):1172–9. https://doi.org/10.1160/TH12-03-0175.
Seely AJE, Ivanovic J, Threader J, et al. Systematic classification of morbidity and mortality after thoracic surgery. Ann Thorac Surg. 2010;90(3):936–42. https://doi.org/10.1016/j.athoracsur.2010.05.014.
Rena O, Papalia E, Oliaro A, et al. Supraventricular arrhythmias after resection surgery of the lung. Eur J Cardio-Thorac Surg. 2001;20(4):688–93. https://doi.org/10.1016/s1010-7940(01)00890-9.
Postoperative AD, Fibrillation A. Postoperative atrial fibrillation. Heart Dis Hagerstown Md. 2001;4:117–23. https://doi.org/10.1097/00132580-200203000-00009.
Garner M, Routledge T, King JE, et al. New-onset atrial fibrillation after anatomic lung resection: predictive factors, treatment and follow-up in a UK thoracic centre. Interact Cardiovasc Thorac Surg. 2017;24(2):260–4. https://doi.org/10.1093/icvts/ivw348.
Kowey PR, Stebbins D, Igidbashian L, et al. Clinical outcome of patients who develop PAF after CABG surgery. Pacing Clin Electrophysiol. 2001;24(2):191–3.
Izhar U, Ad N, Rudis E, et al. When should we discontinue antiarrhythmic therapy for atrial fibrillation after coronary artery bypass grafting? A prospective randomized study. J Thorac Cardiovasc Surg. 2005;129(2):401–6. https://doi.org/10.1016/j.jtcvs.2004.06.029.
To L, Kalus J, Nemerovski C, Jennings D. Readmission rates in patients with post-operative atrial fibrillation after cardiothoracic surgery and the impact of pharmacotherapy. Pharmacotherapy. 2014;34:E184.
ClinicalTrials.gov (2019) The ASPIRE-AF Trial. https://clinicaltrials.gov/ct2/show/NCT03968393
Smith H, Li H, Brandts-Longtin O, et al. External validity of a model to predict postoperative atrial fibrillation after thoracic surgery. Eur J Cardio-Thorac Surg. 2020;57(5):874–80. https://doi.org/10.1093/ejcts/ezz341.
Acknowledgements
The authors have no conflict of interest or disclosures to report.
Funding
No funding to report.
Author information
Authors and Affiliations
Contributions
Conception or design of the work: HS, AS. Data collection: HL, OBL. Data analysis and interpretation: HL, HS, OBL. Drafting the article: HL, HS. Critical revision of the article: HL, HS, AS, OBL, DM, SG, PV, SS, AS. Final approval of the version to be published: HL, HS, AS, OBL, DM, SG, PV, SS, AS.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, H.OY., Smith, H.A., Brandts-Longtin, O. et al. Variation in management of post-operative atrial fibrillation (POAF) after thoracic surgery. Gen Thorac Cardiovasc Surg 69, 1230–1235 (2021). https://doi.org/10.1007/s11748-020-01574-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-020-01574-1