
Abstract
Objectives
We sought to determine whether an AVR performed though a partial upper hemisternotomy (“mini-AVR”) resulted in a greater incidence of patient–prosthesis mismatch (PPM) than those through a full median sternotomy (“AVR”).
Methods
Patients undergoing isolated aortic valve replacement from 2008 to 2013 were identified. Moderate PPM was defined as an in vivo effective orifice area ≤0.85 cm2/m2 body surface area; severe PPM was defined as ≤0.65 cm2/m2. A propensity score-matched analysis was utilized to compare the incidence of PPM between these groups.
Results
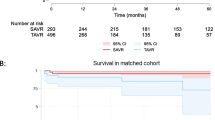
Of the 630 patients undergoing aortic valve surgery, 90 (14.3 %) received mini-AVRs and 540 (85.7 %) received regular AVRs. After propensity matching, we established two cohorts of 85 patients receiving each procedure. Both cohorts were similar with regard to all preoperative covariates including mean age (65.5 vs. 65.1, p = 0.85), diabetes (17.7 vs. 22.4 %), mean BMI (28.3 vs. 28.6, p = 0.73), mean EF (56.9 vs. 55.6, p = 0.43), proportion of patients with aortic stenosis (70.6 vs. 71.8 %, p = 1.00), preoperative valve area (0.88 vs. 0.93 cm2, p = 0.67), and proportion who received a bioprosthesis (85.9 vs. 83.5 %, p = 0.59). Postoperatively, 27.4 % of mini-AVRs and 26.8 % of AVRs had moderate PPM (p = 0.93); 2.4 and 1.2 % had severe PPM (p = 0.66). Kaplan–Meier analysis also failed to reveal a difference in 1-year survival between mini and regular AVRs (93.7 vs. 90.5 %, p = 0.49).
Conclusions
After propensity matching, mini-AVRs are not associated with a greater incidence of PPM than regular AVRs. Severe PPM was rare across both procedure types in this surgical series.
Similar content being viewed by others


References
Rahimtoola SH. The problem of valve prosthesis-patient mismatch. Circulation. 1978;1:20–4.
Pibarot P, Dumesnil JG. Hemodynamic and clinical impact of prosthesis-patient mismatch in the aortic valve position and its prevention. J Am Coll Cardiol. 2000;4:1131–41.
Howell NJ, Keogh BE, Barnet V, Bonser RS, Graham TR, Rooney SJ, et al. Patient–prosthesis mismatch does not affect survival following aortic valve replacement. Eur J Cardiothorac Surg. 2006;1:10–4.
Blais C, Dumesnil JG, Baillot R, Simard S, Doyle D, Pibarot P. Impact of valve prosthesis-patient mismatch on short-term mortality after aortic valve replacement. Circulation. 2003;8:983–8.
Mohty D, Dumesnil JG, Echahidi N, Mathieu P, Dagenais F, Voisine P, et al. Impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: influence of age, obesity, and left ventricular dysfunction. J Am Coll Cardiol. 2009;1:39–47.
Price J, Toeg H, Lam BK, Lapierre H, Mesana TG, Ruel M. The impact of prosthesis-patient mismatch after aortic valve replacement varies according to age at operation. Heart. 2014;14:1099–106.
Ruel M, Al-Faleh H, Kulik A, Chan KL, Mesana TG, Burwash IG. Prosthesis-patient mismatch after aortic valve replacement predominantly affects patients with preexisting left ventricular dysfunction: effect on survival, freedom from heart failure, and left ventricular mass regression. J Thorac Cardiovasc Surg. 2006;5:1036–44.
Chen J, Lin Y, Kang B, Wang Z. Indexed effective orifice area is a significant predictor of higher mid- and long-term mortality rates following aortic valve replacement in patients with prosthesis-patient mismatch. Eur J Cardiothorac Surg. 2014;2:234–40.
Tabata M, Umakanthan R, Cohn LH, Bolman RM 3rd, Shekar PS, Chen FY, et al. Early and late outcomes of 1000 minimally invasive aortic valve operations. Eur J Cardiothorac Surg. 2008;4:537–41.
Bonacchi M, Prifti E, Giunti G, Frati G, Sani G. Does ministernotomy improve postoperative outcome in aortic valve operation? A prospective randomized study. Ann Thorac Surg. 2002;2:460–5 (discussion 465–6).
Machler HE, Bergmann P, Anelli-Monti M, Dacar D, Rehak P, Knez I, et al. Minimally invasive versus conventional aortic valve operations: a prospective study in 120 patients. Ann Thorac Surg. 1999;4:1001–5.
Doll N, Borger MA, Hain J, Bucerius J, Walther T, Gummert JF, et al. Minimal access aortic valve replacement: effects on morbidity and resource utilization. Ann Thorac Surg. 2002;4:S1318–22.
Lee JW, Lee SK, Choo SJ, Song H, Song MG. Routine minimally invasive aortic valve procedures. Cardiovasc Surg. 2000;6:484–90.
Yilmaz A, Sjatskig J, van Boven WJ, Waanders FG, Kelder JC, Sonker U, et al. J-shaped versus median sternotomy for aortic valve replacement with minimal extracorporeal circuit. Scand Cardiovasc J. 2011;6:379–84.
Christiansen S, Stypmann J, Tjan TD, Wichter T, Van Aken H, Scheld HH, et al. Minimally-invasive versus conventional aortic valve replacement–perioperative course and mid-term results. Eur J Cardiothorac Surg. 1999;6:647–52.
Murtuza B, Pepper JR, Stanbridge RD, Darzi A, Athanasiou T. Does minimal-access aortic valve replacement reduce the incidence of postoperative atrial fibrillation? Tex Heart Inst J. 2008;4:428–38.
Bakir I, Casselman FP, Onan B, Van Praet F, Vermeulen Y, Degrieck I. Does a minimally invasive approach increase the incidence of patient–prosthesis mismatch in aortic valve replacement? J Heart Valve Dis. 2014;2:161–7.
Dumesnil JG, Pibarot P. Prosthesis-patient mismatch: an update. Curr Cardiol Rep. 2011;3:250–7.
Freeman M, Webb JG, Willson AB, Wheeler M, Blanke P, Moss RR, et al. Multidetector CT predictors of prosthesis-patient mismatch in transcatheter aortic valve replacement. J Cardiovasc Comput Tomogr. 2013;4:248–55.
Devereux RB, Pini R, Aurigemma GP, Roman MJ. Measurement of left ventricular mass: methodology and expertise. J Hypertens. 1997;15:801–9.
Kaminishi Y, Misawa Y, Kobayashi J, Konishi H, Miyata H, Motomura N, et al. Patient–prosthesis mismatch in patients with aortic valve replacement. Gen Thorac Cardiovasc Surg. 2013;5:274–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Rights and permissions
About this article

Cite this article
Magruder, J.T., Grimm, J.C., Kilic, A. et al. Mini-aortic valve replacements are not associated with an increased incidence of patient–prosthesis mismatch: a propensity-scored analysis. Gen Thorac Cardiovasc Surg 64, 144–148 (2016). https://doi.org/10.1007/s11748-015-0614-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-015-0614-z