
Abstract
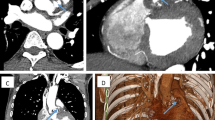
A 67-year-old man with persistent fever and moderate aortic valve regurgitation was transferred. He suffered from incomplete atrioventricular block (AVB), and temporary pacing was needed. Left-to-right shunt flow from the aorta to the right atrium was found without an aneurysm. Operative findings indicated that the aortic valve was highly calcified. The orifice of an aortocavitary fistula (ACF) was detected in the sinus of Valsalva and the right atrium. Patch repair of the aortic annulus with complete débridement of the abscess cavity was performed, a procedure that consisted of aortic valve replacement directly to the Gore-Tex patch and aortic root replacement. His postoperative course was uneventful, but a pacemaker was implanted owing to complete AVB. To our knowledge, this is a rare case in which infective endocarditis was complicated by ACF without an aneurysm of the sinus of valsalva (SV) on the noncoronary cusp to the right atrium and transient incomplete AVB (Mobitz type II) occurring simultaneously.
Similar content being viewed by others


References
Chu CS, Sheu CC, Lee KT, Lee ST, Cheng KH, Voon WC, et al. Ruptured sinus of Valsalva and complete atrioventricular block complicating fulminant course of infective endocarditis: a case report and literature review. Kaohsiung J Med Sci 2006;22:398–403.
David TE, Komeda M, Brofman PR. Surgical treatment of aortic root abscess. Circulation 1989;80(suppl I):I-269–I-274.
Baumgartner FJ, Omari BO, Robertson JM, Nelson RJ, Pandya A, Pandya A, et al. Annular abscess in surgical endocarditis: anatomic, clinical, and operative features. Ann Thorac Surg 2000;70:442–447.
Anguera I, Miro JM, Vilacosta I, Almirante B, Anguita M, Munoz P, et al. Aorto-cavitary fistulous tract formation in infective endocarditis: clinical and echocardiographic features of 76 cases and risk factors for motality. Eur Heart J 2005;26:288–297.
Anguera I, Quaglio G, Miro JM, Pare C, Azqueta M, Marco F, et al. Aortocardiac fistulas complicating infective endocarditis. Am J Cardiol 2001;87:652–654.
Hwang SW, Yucel EK, Bernard S. Aortic root abscess with fistula formation. Chest 1997;111:1436–1438.
Nishi I, Ishizu T, Sakamoto K, Eda K, Ishimitsu T, Watanabe S, et al. A case of sinus of Valsalva-right ventricle fistula without a typical aneurysm, and a single origin of the coronary arteries. Int Heart J 2005;46:531–536.
Takiguchi M, Watanabe H, Shibairi M, Utsumi K, Nagase Y, Ukita H. Surgical treatment for active infective endocarditis with sinus of Valsalva and right atrium fistula. Jpn J Cardiovasc Surg 2001;30:149–151.
Akowuah EF, Casula R, Cooper GJ. Aorto-right atrial fistula associated with native tricuspid valve endocarditis. J Cardiovasc Surg 2002;43:841–842.
Cho Y, Suzuki S, Haga Y. Rare complication of dissection of Valsalva sinus with aorto-left atrial fistula in active aortic valve endocarditis. Jpn J Thorac Cardivasc Surg 2005;53:272–275.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kawahira, T., Iwahashi, K. & Okada, M. Aortocavitary fistula without aneurysm and transient incomplete atrioventricular block due to infective endocarditis. Gen Thorac Cardiovasc Surg 58, 45–48 (2010). https://doi.org/10.1007/s11748-009-0473-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-009-0473-6