
Abstract
To analyze operating room (OR) efficiency by evaluating fixed and variable OR times for open (OPN) and robotic-assisted partial nephrectomies (RAPN). We analyzed consecutive OPN and RAPN performed by one surgeon over a 24-month period. All patients were placed in the lateral decubitus position and secured with a beanbag regardless of approach. Fixed (non-procedural) OR times were prospectively collected and defined as: in-room to anesthesia-release time (IRAT), anesthesia release to cut time (ARCT), and close to wheels-out time (CTWO). Variable OR time was procedural cut to close time (CTCT). Comparisons of fixed and variable OR time points between OPN and RAPN were performed using the Wilcoxon rank-sum test. 146 RAPN and 31 OPN were evaluated from 2019–2020. Median IRAT was similar for RAPN versus OPN [20 min (IQR: 16–25) vs. 20 min (IQR: 16–26), P = 0.57]. Median ARCT was longer for RAPN than it was for OPN [40 min (IQR: 36–46) vs. 34 min (IQR: 30–39), P < 0.001]. Median CTWO was similar for OPN (12 min, IQR: 9–14) and RAPN (11 min, IQR: 7–15) (P = 0.89). Median CTCT was longer for RAPN (202 min, IQR: 170–236) compared to OPN (164 min, IQR: 154–184) (P < 0.001). In a single surgeon, partial nephrectomy series with the same patient positioning, utilization of robotic technology was associated with longer surgeon operating time as well as less efficient fixed OR times, specifically ARCT.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nephron-sparing partial nephrectomy is an important therapeutic option for patients with renal cell carcinoma, and is supported by clinical practice guidelines as the preferred surgical approach for patients with small renal masses [1]. Recent reports have evaluated the effects of surgical approach, including robotic-assisted partial nephrectomy (RAPN) and open partial nephrectomy (OPN), on functional outcomes [2], complications [3], and disease-free survival after surgery [2]. However, the potential impact of surgical approach on operating room efficiency is less well understood.
Optimizing operating room (OR) efficiency is essential for ensuring timely patient access to surgical care. OR efficiency is often looked at through the perspective of evaluating surgeon operating time, although non-procedural OR time may contribute more to total operating time in urologic surgery than initially realized. A recent study demonstrated that fixed operating room time points made up a significant portion of total procedure time in robotic-assisted urologic surgery (up to 49% in some cases) [4]. Thus, efforts to optimize OR efficiency, including potential differences between open and robotic-assisted procedures, must take into account both procedural and non-procedural times.
Therefore, our primary objective was to evaluate RAPN and OPN OR efficiency by evaluating a novel concept of fixed (non-procedural) and variable (procedural) time points. A secondary objective of our analysis was to evaluate the impact of procedure start time on the efficiency of fixed and variable operating room time points for RAPN and OPN. Fixed time points are times throughout the procedure that should have minimal variation between procedures and should not be affected by patient, surgeon, or disease characteristics—including delivering the patient to the OR, intubating the patient, placing the anesthesia lines, surgical patient positioning, sterilizing the operative field, reversing the patient from anesthesia, and stabilizing the patient before they leave the OR. Variable time points are surgeon operating times, which will have greater variation due to patient and surgeon factors.
Methods
Study cohort
Operating room data on 177 consecutive partial nephrectomy procedures performed by one surgeon (146 RAPN and 31 OPN) were prospectively collected over the course of 24 months (2019–2020). All RAPN procedures were completed using the Da Vinci Xi surgical system (Intuitive Surgical Company Sunnyvale, CA, USA).
Variable definitions
Total operating room time was broken into fixed and variable time points (Fig. 1) [4]. Fixed OR times were defined as in-room time to anesthesia-release time (IRAT), anesthesia-release time to cut time (ARCT), in-room time to cut time (IRCT: a combination of IRAT and ARCT), and close time to wheels-out time (CTWO). Variable time was defined as surgeon operating time, cut time to close time (CTCT).

Operating room timeline illustrating the fixed (non-procedural) and variable (procedural) time points. IRAT in-room to anesthesia-release time, ARCT anesthesia release to cut time, IRCT in- room to cut time, CTCT cut to close time, CTWO close to wheels-out time. Reprinted with permission from the Journal of Endourology [4]
IRAT included safely delivering the patient to the operating table, safely intubating the patient, and placement of the anesthesia lines. ARCT involved correctly positioning the patient on the operating table and sterilizing the operative field. CTWO consisted of awaking the patient from anesthesia and stabilizing them prior to transport to the post-anesthesia care unit.
Evaluation of the impact procedure start time had on OR efficiency was performed by dividing procedures into morning starts (incision before 12 pm) and afternoon starts (incision at or after 12 pm).
Patient positioning
For both RAPN and OPN, patients were placed in the supine position for induction of general anesthesia and line placement. Urethral catheters and orogastric tubes are placed in all patients.
Generally, two peripheral intravenous lines and an arterial line are placed.
Patients are then placed in the lateral decubitus position with the target flank placed up (Fig. 2A). An inflatable bean bag is used in all patients. Care is taken to cushion all pressure points including ankles, knees, hips, wrists, and elbows. The legs are separated with three pillows. The patient’s arms are placed over their head on foam pillows and secured with tape. The patient’s body is secured to the operating room table with tape.

Images taken from the operating room illustrating: A the lateral decubitus patient positioning utilized during both robotic and open partial nephrectomies, B placement of the four ports and the Da Vinci Xi robot utilized during RAPN, C the four arms of the docked robot utilized during RAPN, and D the Omni Tract retractor utilized during OPN. Abbreviations: OPN open partial nephrectomy, RAPN robotic-assisted partial nephrectomy
For RAPN, pneumoperitoneum is established with the Veress needle technique. Access is gained to the abdomen with a direct visualizing port and zero-degree lens. All RAPN patients had surgery performed with four robotic arms and one 12 mm assistant port (Fig. 2B, C).
For OPN, a subcostal incision was made two fingerbreadths below the costal margin for all patients. Once intra-abdominal access was achieved, an Omni Tract retractor (Integra LifeSciences Corporation Cincinnati, OH, USA) was placed (Fig. 2D).
Statistical analysis
Box plots were used to graphically display the distributions of fixed and variable OR time points separately for RAPN and OPN procedures. The median and interquartile range (IQR) were used to descriptively summarize fixed and variable OR times. The Wilcoxon rank-sum test was used to compare fixed OR times between procedure types (RAPN vs. OPN). The Wilcoxon rank-sum test was also used to compare fixed and variable OR times between morning and afternoon procedures (morning vs. afternoon) separately for RAPN and OPN. Two-sided P values less than 0.05 were considered statistically significant. R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) was utilized for statistical analysis and creation of boxplots.
Results
177 partial nephrectomies were evaluated (146 RAPN and 31 OPN). Median total OR time for OPN was 237 min (IQR: 220–252) and for RAPN was 273 min (IQR: 244–308) (P < 0.001). Median percent of total OR time occupied by fixed time points was 28.8% (IQR: 25.3–32.7%) for OPN and 26.6% (IQR: 22.9–30.8%) for RAPN.
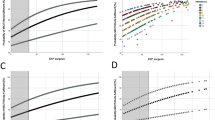
A descriptive summary of all fixed and variable OR time points for each of the partial nephrectomy procedures is shown in (Table 1). (Fig. 3A, B) illustrates fixed time points for OPN and RAPN procedures. (Fig. 3C) demonstrates variable time points for both OPN and RAPN. IRAT and CTWO times were not significantly different between the two procedures (P = 0.57 and P = 0.89, respectively). ARCT, IRCT, and CTCT were all significantly faster for OPN. ARCT median time for OPN was 34 min (IQR: 30–39) and for RAPN was 40 min (IQR: 36–46) (P < 0.001). Median IRCT time for OPN was 55 min (IQR: 54–60) and for RAPN was 62 min (IQR: 56–68) (P = 0.005). CTCT median time for OPN was 164 min (IQR: 154–184) and for RAPN was 202 min (IQR: 170–236) (P < 0.001).

Boxplots comparing fixed (non-procedural) and variable operating room time points for OPN versus RAPN. A IRCT, B CTWO, and C CTCT. Abbreviations: IRCT in-room to cut time, CTWO close to wheels-out time, CTCT cut time to close time, OPN open partial nephrectomy, RAPN robotic-assisted partial nephrectomy
68% (21/31) of OPN and 53% (77/146) of RAPN had start times prior to noon (AM surgeries). (Table 2) shows a comparison of fixed and variable OR time points between OPN that started in the morning and those that started in the afternoon. All OPN fixed OR time points had a difference in medians of less than 4 min between their morning and afternoon times (P ≥ 0.54). The median surgeon operating time for OPN was 8 min longer in the morning compared to the afternoon (median CTCT: 166 vs. 158 min, P = 0.50). Table 3 shows a comparison between morning and afternoon fixed and variable OR time points for RAPN. All RAPN fixed operating time points had a difference in medians of 2 min or less between their morning and afternoon times (all P ≥ 0.097). Median CTCT time for RAPN was 5 min shorter in the morning than the afternoon (197 vs. 202 min, P = 0.40).
Discussion
To our knowledge, this analysis is the first to observe that the use of robotic equipment may decrease the efficiency of fixed operating room time during partial nephrectomy. RAPN was less efficient than OPN at all operating time points in this single-surgeon experience, including ARCT, IRCT, and CTCT time. Breaking procedures into these time points is especially helpful to surgeons when comparing RAPN to OPN as it highlights opportunities to improve OR efficiency both within and outside of the surgeon’s control. Knowledge of these differences between OPN and RAPN may be helpful in perioperative resource planning and may allow OR administrators to account for expected differences in procedure duration, personnel and equipment needs when seeking to optimize OR workflow.
Lee et al. and Kowalewski et al. recently found that total OR time was longer for RAPN than it was for OPN, 173.3 min versus 149.0 min and 157 min versus 143 min, respectively [2, 3]. In our study, we also found RAPN to have a longer median OR time than OPN (273 vs. 237 min). Lee et al. looked at a smaller number of cases 67 OPN and 67 RAPN. They also only included procedures on patients with a single mass ≥ 4 cm with a normal contralateral kidney [2]. Kowalewski et al. examined a larger sample of patients than we did, 166 OPN and 83 RAPN. They case matched their patients 2:1 with age, BMI, RENAL score, gender, and tumor size [3]. It should be noted that resident trainees were involved in 100% of the surgical procedures performed at our institution.
A study performed by Catchpole et al. categorized RAPN into four phases: pre-robot, abdominal insufflation and robot docking, surgical intervention (surgeon on robot), and surgeon off robot and robot undocking [5]. Flow disruptions during these phases and the impact these disruptions had on efficiency were analyzed. They found that information often had to be repeated if the OR was noisy or because of issues with the microphone when the surgeon was at the console [5]. These factors may have contributed to the increase we found in variable time (surgeon operating time) for RAPN procedures (273 min) in comparison to OPN procedures (237 min). The surgeon being away from the operating table and the personnel assisting in the operation during RAPN may contribute to the decrease in efficiency compared to OPN.
We found that procedure start time did not have a significant impact on fixed (non-procedural) or variable (procedural) OR times for OPN or RAPN. Our analysis demonstrates morning and afternoon procedures maintained the same level of efficiency. This demonstrates that staff shift changes and time of day did not affect the duration of procedure time points or the efficiency in which these tasks were performed. Sugunes et al. performed a study looking at the impact of time of day on renal transplant patient outcomes [6]. They defined “day-time” as 8am–8 pm and “night-time” as 8 pm-8am, while our procedures were evaluated based on morning (before 12 pm) versus afternoon (at or after 12 pm) start times. Of the procedures we evaluated, the earliest in-room time was 7:20am and the latest in-room time was 3:40 pm. Sugunes et al. found that kidney recipients with night procedures had more wound complications, but that ultimately time of day did not impact CTCT (surgeon operating time) efficiency or the risk of an adverse event occurring [6].
Our study was limited by the exclusion of patient-specific factors from the analysis. Through analyzing fixed (non-procedural) OR times, we attempted to remove surgeon and clinical factors. However, it has been reported that obese patients are more difficult to intubate [7], which may impact the duration of ARCT time. It has also been shown that the sex of the patient (male vs. female) impacts robotic set-up time, which is a variable (procedural) time in the OR [8]. Another limitation was the inclusion of the COVID-19 era in our analysis. The impact of COVID-19 on OR efficiency is still being studied. The COVID era impacted different aspects of surgical practices across the world in various ways. To make our operative data as “normal” as possible so that it could be utilized in the post-COVID era, we only performed partial nephrectomies on COVID-negative patients. All procedures included in this analysis were on patients confirmed negative for COVID-19 (with nasopharyngeal swabbing and reverse transcription polymerase chain reaction testing) within 48 h of their procedure.
Conclusion
In this single-surgeon series of partial nephrectomies, utilization of robotic technology was associated with less-efficient fixed operating room time points, specifically ARCT. These data suggest that OR efficiency analyses for partial nephrectomy cases should be adjusted for surgical approach.
References
Wu Z, Li M, Liu B et al (2014) Robotic versus open partial nephrectomy: a systematic review and meta-analysis. PLoS ONE 9(4):e94878
Lee S, Ryu H, Lee JW (2021) Open partial nephrectomy vs robot-assisted partial nephrectomy for a renal tumor larger than 4 cm: a propensity score matching analysis. J Korean Med Sci. https://doi.org/10.3346/jkms.2021.36.e135
Kowalewski KF, Muller D, Kirchner M et al (2021) Robotic-assisted versus conventional open partial nephrectomy (robocop): a propensity score-matched analysis of 249 patients. Urol Int 105(5–6):490–498
Geldmaker LE, Hasse CH, Baird B et al (2021) Analysis of operating room (or) efficiency during robotic-assisted urologic surgeries utilizing fixed (nonprocedural) operative times. J Endourol 36(5):654–660
Catchpole KR, Hallett E, Curtis S et al (2018) Diagnosing barriers to safety and efficiency in robotic surgery. Ergonomics 61(1):26–39
Sugunes N, Bichmann A, Biernath N et al (2019) Analysis of the effects of day-time vs. night-time surgery on renal transplant patient outcomes. J Clin Med. https://doi.org/10.3390/jcm8071051
Shailaja S, Nichelle SM, Shetty AK et al (2014) Comparing ease of intubation in obese and lean patients using intubation difficulty scale. Anesth Essays Res 8(2):168–174
Kozminski DJ, Cerf MJ, Feustel PJ et al (2020) Robot set-up time in urologic surgery: an opportunity for quality improvement. J Robot Surg 14(5):745–752
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by LG, CH, and Dr. DT. Formal statistical analysis was performed by Colleen Ball and MW. The first draft of the manuscript was written by LG and Dr. DT and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Dr. David Thiel and Dr. Raymond Pak are both shareholders in Auris Robotics. The remaining authors have no relevant financial or non-financial interests to disclose. All authors certify they have no financial disclosures to report.
Ethics approval
This study was approved by the Mayo Clinic Institutional Review Board, #20–008079.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Geldmaker, L.E., Hasse, C.H., Baird, B.A. et al. Analysis of fixed and variable operating room (or) time point efficiency in partial nephrectomies: open versus robotic-assisted. J Robotic Surg 17, 853–858 (2023). https://doi.org/10.1007/s11701-022-01477-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-022-01477-8