
Abstract
Background and Aims
Longitudinal assessment of body composition following bariatric surgery allows monitoring of health status. Our aim was to elucidate trends of anthropometric and clinical outcomes 3 years following sleeve gastrectomy (SG).
Methods
A prospective cohort study of 60 patients who underwent SG. Anthropometrics including body composition analysis measured by multi-frequency bioelectrical impedance analysis, blood tests, liver fat content measured by abdominal ultrasound and habitual physical activity were evaluated at baseline and at 6 (M6), 12 (M12), and 36 (M36) months post-surgery.
Results
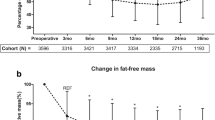
Sixty patients (55% women, age 44.7 ± 8.7 years) who completed the entire follow-up were included. Fat mass (FM) was reduced significantly 1 year post-surgery (55.8 ± 11.3 to 26.7 ± 8.3 kg; P < 0.001) and then increased between 1 and 3 years post-operatively, but remained below baseline level (26.7 ± 8.3 to 33.1 ± 11.1 kg; P < 0.001). Fat free mass (FFM) decreased significantly during the first 6 months (64.7 ± 14.3 to 56.9 ± 11.8 kg; P < 0.001), slightly decreased between M6 and M12 and then reached a plateau through M36. Weight loss “failure” (< 50% excess weight loss) was noticed in 5.0% and 28.3% of patients at M12 and M36, respectively. Markers of lipid and glucose metabolism changed thereafter in parallel to the changes observed in FM, with the exception of HDL-C, which increased continuingly from M6 throughout the whole period analyzed (45.0 ± 10.2 to 59.5 ± 15.4 mg/dl; P < 0.001) and HbA1c which continued to decrease between M12 and M36 (5.5 ± 0.4 to 5.3 ± 0.4%; P < 0.001). There were marked within-person variations in trends of anthropometric and clinical parameters during the 3-year follow-up.
Conclusions
Weight regain primarily attributed to FM with no further decrease in FFM occurs between 1 and 3 years post-SG. FM increase at mid-term may underlie the recurrence of metabolic risk factors and can govern clinical interventions.



Similar content being viewed by others


Abbreviations
- BIA:
-
Bioelectrical impedance analysis
- BMI:
-
Body mass index
- CRP:
-
C-reactive protein
- DEXA:
-
Dual X-ray absorptiometry
- EWL:
-
Excess weight loss
- FFM:
-
Fat free mass
- FM:
-
Fat mass
- HbA1C:
-
Hemoglobin A1c
- HRI:
-
Hepato-renal index
- HDL-C:
-
High-density lipoprotein cholesterol
- HOMA:
-
Homeostasis model assessment
- IBW:
-
Ideal body weight
- IR:
-
Insulin resistance
- LDL-C:
-
Low-density lipoprotein cholesterol
- NAFLD:
-
Nonalcoholic fatty liver disease
- RCT:
-
Randomized clinical trial
- RYGB:
-
Roux-en-Y gastric bypass
- RMR:
-
Resting metabolic rate
- SG:
-
Sleeve gastrectomy
- TC:
-
Total cholesterol
- WC:
-
Waist circumference
References
Angrisani L, Santonicola A, Iovino P, et al. IFSO Worldwide Survey 2016: primary, endoluminal, and revisional procedures. Obes Surg. 2018.
Lauti M, Kularatna M, Hill AG, et al. Weight regain following sleeve gastrectomy—a systematic review. Obes Surg. 2016;26(6):1326–34.
Felsenreich DM, Langer FB, Prager G. Weight loss and resolution of comorbidities after sleeve gastrectomy: a review of long-term results. Scand J Surg. 2018;6:1457496918798192.
Azagury D, Mokhtari TE, Garcia L, et al. Heterogeneity of weight loss after gastric bypass, sleeve gastrectomy, and adjustable gastric banding. Surgery 2018.
Clapp B, Wynn M, Martyn C, et al. Long term (7 or more years) outcomes of the sleeve gastrectomy: a meta-analysis. Surg Obes Relat Dis. 2018;14:741–7.
Golomb I, Ben David M, Glass A, et al. Long-term metabolic effects of laparoscopic sleeve gastrectomy. JAMA Surg. 2015;150(11):1051–7.
Faria SL, Faria OP, Cardeal MD, et al. Validation study of multi-frequency bioelectrical impedance with dual-energy X-ray absorptiometry among obese patients. Obes Surg. 2014;24(9):1476–80.
Tewari N, Awad S, Macdonald IA, et al. A comparison of three methods to assess body composition. Nutrition. 2018;47:1–5.
Friedrich AE, Damms-Machado A, Meile T, et al. Laparoscopic sleeve gastrectomy compared to a multidisciplinary weight loss program for obesity—effects on body composition and protein status. Obes Surg. 2013;23(12):1957–65.
Wolfe BM, Schoeller DA, McCrady-Spitzer SK, et al. Resting metabolic rate, total daily energy expenditure, and metabolic adaptation 6 months and 24 months after bariatric surgery. Obesity (Silver Spring, Md). 2018;26(5):862–8.
Skogar M, Holmback U, Hedberg J, et al. Preserved fat-free mass after gastric bypass and duodenal switch. Obes Surg. 2017;27(7):1735–40.
Sherf Dagan S, Tovim TB, Keidar A, et al. Inadequate protein intake after laparoscopic sleeve gastrectomy surgery is associated with a greater fat free mass loss. Surg Obes Relat Dis. 2017;13(1):101–9.
Golzarand M, Toolabi K, Djafarian K. Changes in body composition, dietary intake, and substrate oxidation in patients underwent laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy: a comparative prospective study. Obes Surg. 2018.
Guida B, Cataldi M, Busetto L, et al. Predictors of fat-free mass loss 1 year after laparoscopic sleeve gastrectomy. J Endocrinol Investig. 2018;41(11):1307–15.
de Cleva R, Mota FC, Gadducci AV, et al. Resting metabolic rate and weight loss after bariatric surgery. Surg Obes Relat Dis. 2018;14(6):803–7.
Vazquez-Velazquez V, Rodriguez Gonzalez A, Ordonez Ortega S, et al. Differences in body composition in patients with obesity 1 year after Roux-En-Y gastric bypass: successful vs. unsuccessful weight loss. Obes Surg. 2018;28(3):864–8.
Crisp AH, Verlengia R, Ravelli MN, et al. Changes in physical activities and body composition after Roux-Y gastric bypass surgery. Obes Surg. 2018;28(6):1665–71.
Sans A, Bailly L, Anty R, et al. Baseline anthropometric and metabolic parameters correlate with weight loss in women 1-year after laparoscopic Roux-En-Y gastric bypass. Obes Surg. 2017;27(11):2940–9.
Wells J, Miller M, Perry B, et al. Preservation of fat-free mass after bariatric surgery: a comparison of malabsorptive and restrictive procedures. Am Surg. 2015;81(8):812–5.
Otto M, Elrefai M, Krammer J, et al. Sleeve Gastrectomy and Roux-en-Y gastric bypass lead to comparable changes in body composition after adjustment for initial body mass index. Obes Surg. 2016;26(3):479–85.
Adamczyk P, Buzga M, Holeczy P, et al. Body size, bone mineral density, and body composition in obese women after laparoscopic sleeve Gastrectomy: a 1-year longitudinal study. Horm Metab Res. 2015;47(12):873–9.
Vaurs C, Dimeglio C, Charras L, et al. Determinants of changes in muscle mass after bariatric surgery. Diabetes Metab. 2015;41(5):416–21.
Bazzocchi A, Ponti F, Cariani S, et al. Visceral fat and body composition changes in a female population after RYGBP: a two-year follow-up by DXA. Obes Surg. 2015;25(3):443–51.
Iannelli A, Martini F, Rodolphe A, et al. Body composition, anthropometrics, energy expenditure, systemic inflammation, in premenopausal women 1 year after laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2014;28(2):500–7.
Andreu A, Moize V, Rodriguez L, et al. Protein intake, body composition, and protein status following bariatric surgery. Obes Surg. 2010;20(11):1509–15.
Kim G, Tan CS, Tan KW, Lim SPY, So JBY, Shabbir A. Sleeve gastrectomy and Roux-En-Y gastric bypass lead to comparable changes in body composition in a multiethnic Asian population. J Gastrointest Surg. 2018.
Gomez-Ambrosi J, Andrada P, Valenti V, et al. Dissociation of body mass index, excess weight loss and body fat percentage trajectories after 3 years of gastric bypass: relationship with metabolic outcomes. Int J Obes (2005). 2017;41(9):1379–87.
Cole AJ, Kuchnia AJ, Beckman LM, et al. Long-term body composition changes in women following Roux-en-Y gastric bypass surgery. JPEN J Parenter Enteral Nutr. 2017;41(4):583–91.
Nicoletti CF, Camelo Jr JS, dos Santos JE, et al. Bioelectrical impedance vector analysis in obese women before and after bariatric surgery: changes in body composition. Nutrition. 2014;30(5):569–74.
Johnson Stoklossa C, Atwal S. Nutrition care for patients with weight regain after bariatric surgery. Gastroenterol Res Pract. 2013;2013:256145.
Sherf-Dagan S, Zelber-Sagi S, Zilberman-Schapira G, et al. Probiotics administration following sleeve gastrectomy surgery: a randomized double-blind trial. Int J Obes. 2018;42(2):147–55.
Brethauer SA, Kim J, el Chaar M, et al. Standardized outcomes reporting in metabolic and bariatric surgery. Surg Obes Relat Dis. 2015;11(3):489–506.
De Lorenzo A, Soldati L, Sarlo F, et al. New obesity classification criteria as a tool for bariatric surgery indication. World J Gastroenterol: WJG. 2016;22(2):681–703.
Snitker S. Use of body fatness cutoff points. Mayo Clin Proc. 2010;85(11):1057. author reply -8
Ruiz-Lozano T, Vidal J, de Hollanda A, et al. Timing of food intake is associated with weight loss evolution in severe obese patients after bariatric surgery. Clin Nutr. 2016;35(6):1308–14.
Becroft L, Ooi G, Forsyth A, et al. Validity of multi-frequency bioelectric impedance methods to measure body composition in obese patients: a systematic review. Int J Obes (2005). 2018.
Webb M, Yeshua H, Zelber-Sagi S, et al. Diagnostic value of a computerized hepatorenal index for sonographic quantification of liver steatosis. AJR Am J Roentgenol. 2009;192(4):909–14.
Sakai S, Tanimoto K, Imbe A, et al. Decreased beta-cell function is associated with reduced skeletal muscle mass in Japanese subjects without diabetes. PloS One. 2016;11(9):e0162603.
Kriska AM, Caspersen CJ. Introduction to a collection of physical activity questionnaires. Med Sci Sports Exerc. 1997;29:5–9.
Otto M, Kautt S, Kremer M, et al. Handgrip strength as a predictor for post bariatric body composition. Obes Surg. 2014;24(12):2082–8.
Belfiore A, Cataldi M, Minichini L, et al. Short-term changes in body composition and response to micronutrient supplementation after laparoscopic sleeve gastrectomy. Obes Surg. 2015;25(12):2344–51.
Verger EO, Aron-Wisnewsky J, Dao MC, et al. Micronutrient and protein deficiencies after gastric bypass and sleeve gastrectomy: a 1-year follow-up. Obes Surg. 2015.
Dulloo AG, Jacquet J, Miles-Chan JL, et al. Passive and active roles of fat-free mass in the control of energy intake and body composition regulation. Eur J Clin Nutr. 2017;71(3):353–7.
Vigilante A, Signorini F, Marani M, et al. Impact on dyslipidemia after laparoscopic sleeve gastrectomy. Obes Surg. 2018;28:3111–5.
Aminian A, Zelisko A, Kirwan JP, et al. Exploring the impact of bariatric surgery on high density lipoprotein. Surg Obes Relat Dis. 2015;11(1):238–47.
Algooneh A, Almazeedi S, Al-Sabah S, et al. Non-alcoholic fatty liver disease resolution following sleeve gastrectomy. Surg Endosc. 2016;30(5):1983–7.
Berry MA, Urrutia L, Lamoza P, et al. Sleeve gastrectomy outcomes in patients with BMI between 30 and 35–3 years of follow-up. Obes Surg. 2018;28(3):649–55.
De Luca M, Angrisani L, Himpens J, et al. Indications for surgery for obesity and weight-related diseases: position statements from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg. 2016;26(8):1659–96.
Haverkort EB, Reijven PL, Binnekade JM, de van der Schueren MA, Earthman CP, Gouma DJ, et al. Bioelectrical impedance analysis to estimate body composition in surgical and oncological patients: a systematic review.European journal of clinical nutrition. 2015;69:3-13.
Beato GC, Ravelli MN, Crisp AH, et al. Agreement between body composition assessed by bioelectrical impedance analysis and doubly labeled water in obese women submitted to bariatric surgery : body composition, BIA, and DLW. Obes Surg. 2018.
Funding
This study was supported (in part) by grant no. 3-10470 from the Chief Scientist Office of the Ministry of Health, Israel. The funding source did not have a role in the design, conduct, and analysis of the study or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows—SSD, OS, SZS, NS, DG, AR, and AD designed the research; SSD, AB, NB, and MW performed the research; SSD and SZS analyzed the data; SSD, SZS, and OS wrote the manuscript. All authors critically revised the manuscript, agree to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in this study were approved by the institutional review board and in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The RCT study was pre-registered in the NIH registration website (TRIAL no. NCT01922830).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sherf-Dagan, S., Zelber-Sagi, S., Buch, A. et al. Prospective Longitudinal Trends in Body Composition and Clinical Outcomes 3 Years Following Sleeve Gastrectomy. OBES SURG 29, 3833–3841 (2019). https://doi.org/10.1007/s11695-019-04057-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-04057-2