
Abstract
Background
Roux-en-Y gastric bypass (RYGB) is considered effective for weight loss and for treatment of many obesity-related metabolic diseases. Ghrelin is an essential orexigenic peptide that plays an indispensable role in controlling body weight and energy homeostasis of post-operative patients. This systematic review and meta-analysis aimed to investigate changes in the level of fasting total ghrelin following RYGB.
Methods
A systematic literature search of PubMed, EMBASE, and the Cochrane Library until April 2018 with keywords “ghrelin” and “gastric bypass” was performed in accordance with the MOOSE guidelines and PRISMA statement. Three reviewers independently selected the studies and extracted data. Quality assessment of the included studies was undergone. A random effects model was employed to calculate overall effect sizes. Subgroup analyses and meta-regression were subsequently performed.
Results
Sixteen studies with 325 patients were included. We found ghrelin levels had an increasing tendency (SMD = 0.30; 95% CI = 0.04 to 0.57) despite moderate heterogeneity (I2 = 58%). Subsequent subgroup analysis indicated that ghrelin levels decreased (SMD = − 0.49; 95% CI = − 0.98 to 0.00) in the short term (≤ 3 months) and increased (SMD = 0.46; 95% CI = 0.22 to 0.69) in the long term (> 3 months) after RYGB. Meta-regression showed that gastric pouch volume, alimentary limb length and biliopancreatic limb length were not associated with changes in ghrelin levels.
Conclusion
Fasting total ghrelin levels decreased in the short term (≤ 3 months) and increased in the long term (> 3 months) after RYGB.
Similar content being viewed by others


Introduction
With the improvement in human living standards, overweight [body mass index (BMI) ≥ 25 kg/m2] and obesity (BMI ≥ 30 kg/m2) have become a worldwide problem for decades, beginning in the last century [1]. Under present circumstances, several weight loss treatments have emerged, including lifestyle modification, medication, and surgery. Among these treatments, bariatric surgery is considered the most effective for long-term treatment of morbid obesity [2]. Roux-en-Y gastric bypass (RYGB), as one of many described surgerical procedures, was shown to be effective for long-term weight loss and improvement in obesity-related comorbidities and quality of life [3]. Briefly, RYGB creates a small gastric pouch and attaches it to the mid-jejunum, bypassing most of the stomach and the proximal jejunum [4]. Other than the gastric pouch, there are two limb characteristics of RYGB: one is the alimentary limb where food passes and the other is the biliopancreatic limb which permits biliopancreatic secretion [5]. Despite of its effectiveness, the underlying mechanisms resulting in weight loss and metabolic improvements remain not adequately understood. Numerous studies suggest that leptin and gastrointestinal (GI) hormones, including ghrelin, peptide YY (PYY), and glucagon-like peptide 1 (GLP-1), important regulators in the control of eating, meal-related glycemia, and obesity all display significant changes in levels after RYGB. Thus, it is believed that GI hormone alterations are closely related to the physiological changes after RYGB, which involves complex gut-brain signaling [6, 7].
Ghrelin, a 28-amino acid peptide that was discovered in extracts of rat stomach in 1999 [8] was involved in regulating of food intake and energy balance [9]. Studies indicate ghrelin stimulates appetite [10], affecting glucose utilization rates in adipose tissue [11], and promoting hepatic lipogenesis [12]. In healthy individuals, ghrelin expression increased in the fasting status but decreased significantly after meals [13]. Interestingly, Tschöp M et al. found that circulating ghrelin levels significantly decreased in obese people and were negatively correlated with BMI [14]. As mentioned earlier, ghrelin levels change after undergoing RYGB. However, the outcomes are controversial. In some observational studies, ghrelin levels after RYGB substantially increased [15, 16]. By contrast, other studies reported that levels decreased [17, 18]. To date, there has been no meta-analysis to settle this dispute. Thus, we performed this systematic review and meta-analysis to determine the relationship between ghrelin levels and RYGB. Furthermore, we discussed the possible mechanisms of ghrelin levels change after RYGB.
Methods
This was a systematic review and meta-analysis conducted and reported in accordance with the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines [19] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [20]. The review was registered at PROSPERO (https://www.crd.york.ac.uk/PROSPERO/) as registration number CRD42018100014.
Databases and Search Strategy
The literature review was performed based on three online databases: PubMed, EMBASE, and the Cochrane Library (until April 2018). The Medical Subject Headings (MeSH) included in the search strategy were “ghrelin” and “gastric bypass,” and the free terms were searched in PubMed. The key terms and free terms were used in every possible combination. The full search strategies for all databases can be found in Supplementary Table 1. Three authors independently reviewed and cross-checked the articles. All agreed that the relevant studies were qualified. We supplemented the search by reviewing references lists of pertinent articles manually. Disagreements among the reviewers were resolved by consensus.
Study Selection and Criteria
Inclusion criteria were as follows: (i) original comparative reports with ≥ 5 patients; (ii) written in English; (iii) conducted on human subjects; and (iv) reporting fasting total ghrelin levels pre- and post-RYGB.
Exclusion criteria were as follows: (i) non-human studies; (ii) non-RYGB interventions; (iii) letters and comments, reviews, and meta-analyses; and (iv) data not presented as mean ± standard deviation (SD).
Data Collection and Quality Assessment
Three reviewers independently browsed the studies eligible for this meta-analysis and extracted the corresponding data to fill in a predefined form. Final discrepancies were resolved by discussion. The following data were extracted: study characteristics (author, country, publication year, study design, number of study participants); patient characteristics [age, gender, BMI, diabetes, fasting blood glucose, fasting plasma insulin, the homeostasis model assessment of insulin resistance (HOMA-IR), HbA1c]; outcomes (ghrelin levels); and RYGB features (operative technique, gastric pouch volume, alimentary limb length, and biliopancreatic limb length). We did not contact authors to obtain unpublished data.
Quality of included studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS) for observational cohort studies [21]. The quality assessment criteria were as follows: (i) whether the patients included in the study really represented all people in the population who had undergone RYGB surgery; (ii) whether the non-exposed group was from the same population as the RYGB group; (iii) whether the RYGB had a confirmed surgical record; (iv) whether ghrelin levels had been known before RYGB; (v) whether the study considered the comparability of RYGB and non-RYGB groups in design and statistical analysis; (vi) whether the results of the study had file records; (vii) whether the follow-up time for the population was sufficiently long; and (viii) whether the follow-up in RYGB group was complete. The maximum score attainable was 9 and studies with a score equal to or higher than 6 were considered be eligible for our meta-analysis.
As for randomized clinical trials (RCT), we used the Cochrane methodology to assess their quality. The quality evaluation criteria included (i) random sequence generation; (ii) allocation concealment; (iii) blinding of participants and personnel; (iv) blinding of outcome assessment; (v) incomplete outcome data; (vi) selective reporting; and (vii) other bias. Each criterion was judged as high, unknown, or low-risk bias. The results of the assertions were placed in a risk-of-bias summary.
Data Synthesis and Analysis
We calculated the standard mean difference (SMD) in ghrelin levels post- and pre-RYGB with 95% confidence intervals (CIs). Cochran’s Q (chi-square) test was used to quantify the heterogeneity, and the I2 statistic was used to assess the extent of inconsistency: (1) low> 25%, (2) moderate> 50%, and (3) high> 75%. [22]. A two-sided P value of less than 0.05 was defined as statistical significance. Random effects models were employed to estimate pooled effect sizes [23]. Publication bias was assessed by Begg’s test [24] and Egger’s test [25]. Subgroup analysis was performed according to time course, diabetes mellitus (DM), blood sample, measuring method, study design, and operative technique. Finally, we did a meta-regression to analyze the relationship between surgical technical characteristics (including gastric pouch volume, alimentary limb length, and biliopancreatic limb length) and change of ghrelin levels. All statistical analyses were conducted using the Review Manager (RevMan 5.3) statistical software and Stata (version 14; Stata, College Station, TX, USA).
Results
Literature Search
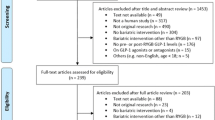
The flow diagram outlining the searching procedures is presented in Fig. 1. A total of 735 potential articles were identified. After checking duplicates, reviewing titles, abstracts, and full text, 16 eligible articles [15, 16, 26,27,28,29,30,31,32,33,34,35,36,37,38,39] were included in our meta-analysis. Thereinto, one article was identified through reference [37]. The publication dates of the included articles ranged from 2006 to 2017. The sample size of the trials ranged from nine to 96. Quality assessment of the included studies is presented in Supplementary Table 2 (for cohort studies) and Supplementary Fig. 1 [for randomized controlled trials (RCT)].

PRISMA flow diagram showing selection of articles for review
Patient Characteristics
Through layers of screening, 325 patients were finally enrolled in our meta-analysis. Detailed characteristics are displayed in Table 1. The BMI of all the participants were more than 40 kg/m2 and some of the patients were diagnosed with DM. Fasting plasma and serum total ghrelin levels were examined by the means of enzyme-linked immunosorbent assay (ELISA) or radioimmunoassay (RIA). Data of RYGB features (gastric pouch volume, alimentary limb length, and biliopancreatic limb length) are listed in Supplementary Table 3.
Overall Analysis
As demonstrated in Fig. 2, ghrelin levels after RYGB were significantly higher than pre-surgery levels [SMD = 0.30; 95% CI (0.04 and 0.57), P = 0.03]. The SMD from studies that exhibited significant heterogeneity was assessed by a random effect model (I2 = 58%, P = 0.002). No Publication bias was found using both Begg’s test (P = 0.322) and Egger’s test (P = 0.061).

Forest plot of fasting total ghrelin levels before and after RYGB (random effects model)
Subgroup Analysis
We divided these studies into two subgroups: short term (measuring time within or equal to 3 months) and long term (measuring time exceeding 3 months). The short-term subgroup consisted of three studies [27, 30, 37] and the analysis showed that fasting total ghrelin levels after RYGB were significantly lower than pre-surgery levels [SMD = − 0.49; 95% CI (− 0.98 and 0.00), P = 0.05, I2 = 0%]. The measuring time of ghrelin in 13 studies [15, 16, 26, 28, 29, 31,32,33,34,35,36, 38, 39] was longer than 3 months. These studies showed that ghrelin levels after RYGB surgery were markedly higher than pre-surgery levels [SMD = 0.46; 95% CI (0.22 and 0.69), P = 0.0002, I2 = 42%]. These results are shown in Fig. 3.

Forest plot of fasting total ghrelin levels in the short term or long term before and after RYGB (random effects model)
In the subsequent analysis, we analyzed other subgroups classified by DM (yes, no or yes/no), blood sample (plasma or serum), measuring method (ELISA or RIA), study type (RCT or cohort study), and operative technique (laparoscopic, open/laparoscopic or unknown). However, as illustrated in Table 2, the outcomes showed either no significance or high heterogeneity based on the presented evidence.
Meta-regression Analysis
Meta-regression analysis (Table 3) indicated that gastric pouch volume, alimentary limb length, and biliopancreatic limb length were not significant predictors of the change in fasting total ghrelin after RYGB (P > 0.05 for all).
Discussion
In our meta-analysis, we found that fasting total ghrelin levels changed after RYGB and this change was associated with time course of the surgery. To the best of our knowledge, this was the first systematic review and meta-analysis to use statistical methods to observe and analyze clinical trials of total ghrelin level changes. Using subgroup analysis, we attempted to seek the source from which heterogeneity of post-operative ghrelin levels were generated.
Previous studies suggested that most patients’ appetite and preference for food changed after undergoing RYGB. Their preference for high-fat diet was far less than it was prior to surgery, and this high-fat aversion may be another cause of energy intake reduction in addition to malabsorption [26, 40]. We believe that hormones relating to food intake, including ghrelin, GLP-1, leptin, and PYY, may play vital roles in alteration of eating behavior. Regarding post-RYGB ghrelin levels, however, divergence emerged. Hence, we tried to reconcile disparate reports and draw a rational conclusion as to how ghrelin levels change.
While screening articles obtained from databases, we found 16 pieces met our criteria. In the process of extracting data, we focused on the ghrelin level at various time points after RYGB and other factors as well that may influence it. In the overall analysis, the time points we selected were closest to 1 year. From the forest plot (Fig. 2), we found that, at this time, post-operative ghrelin levels increased significantly (P = 0.03). However, moderate heterogeneity (I2 = 58%) suggested some confounding factors may have been responsible. Consequently, we performed subgroup analysis attempting to reduce or eliminate the heterogeneity.
In the subgroup analysis, the interval between the operative time and testing time was assumed to be an important factor, since previous studies had found this problem but failed to provide an answer [6]. To reduce the heterogeneity, the groups were divided into short-term (≤ 3 months) and long-term (> 3 months) subgroups. The forest plot is shown as Fig. 3. Ghrelin levels decreased in the short term but increased significantly in the long term. Considering the bias of short-term ghrelin levels that might be generated by small sample size (only three studies with 33 patients), we also extracted data of ghrelin levels within 3 months from these 16 articles. There are total six articles [26, 27, 30, 36,37,38] mentioning short-term ghrelin levels and we found a similar outcome [SMD = − 0.23; 95% CI (− 0.51 and 0.05), P = 0.70, I2 = 0%] to Fig. 3. Rodent data by Williams DL et al. suggested that the vagus nerve mediated secretion of ghrelin [41]. Sundbom M et al. found that ghrelin levels fell transiently after RYGB which they hypothesized possibly due to vagal dysfunction [42]. Moreover, Lin et al. reported that the most significant declines of ghrelin levels were observed following division of the stomach to create a small gastric pouch [43]. Another clinical trial by Cummings DE et al. suggested that gastric restriction as one mechanism by which RYGB suppressed ghrelin secretion [17], since gastric restriction caused impaired ghrelin secretory capacity [6]. As for long-term outcomes, post-operative ghrelin levels were higher than pre-surgery levels that were similar to those of healthy individuals [44]. Randy J. Seeley suggested that weight loss or dynamic adaptation of the GI tract may result in such gradual normalization of ghrelin secretion after RYGB [45].
So far, the mechanisms of weight-losing effects of RYGB are not clear. Based on our present study, we believe that ghrelin may play a role in the weight loss of the patients undergoing RYGB in the short term. But in the long term (about 1 year after RYGB), ghrelin levels did not keep decreasing while weight of the patients continued to decline, indicating ghrelin might not be involved in the weight-losing effects of RYGB in the long term. There might exist other factors contributing to it. Despite of the weight loss in the earlier stage, as reported in a clinical study, a portion of patients suffered weight regain as time passed for some reasons [46]. The elevation of ghrelin levels could explain the fact. Work of Tamboli RA et al. suggested that increased ghrelin levels could be detected in patients who experienced weight regain [47]. In turn, we assume that the elevation of ghrelin may indicate the weight regain in the future although the weight of patients might not rebound yet at that time. Interestingly, in the study mentioned earlier, the authors concluded that ghrelin level was not correlated with weight regain in 5 ± 4-year post-RYGB [46]. Further research may better define potential associations between ghrelin levels and weight change after RYGB. In our analysis, the post-operative BMI did not rebound as the ghrelin increased in the long term post-RYGB [SMD = − 3.23; 95% CI (− 3.84 and − 2.63), P < 0.00001, I2 = 73%, data not shown]. This outcome might be the result of shorter follow-up time compared with the abovementioned studies. Moreover, our results indicated that ghrelin levels (12 months after RYGB) were negative related to weight loss (β = − 0.08, P = 0.001, data not shown).
We also observed and analyzed other factors that could affect ghrelin levels, including DM, blood sample, measuring methods, study type, and operative technique (Table 2). However, subgroup analysis did not show reduced heterogeneity. Hence, based on our present extracted data, the abovementioned factors might not be the causes accounting for the overall analysis heterogeneity.
Collectively, our work determined the connections between ghrelin levels and time course of RYGB. As mentioned earlier, many other hormones may contribute to the effectiveness after RYGB except for ghrelin. Changes in levels of leptin, PYY, and GLP-1 after RYGB were also reported in some of the included studies [27, 30, 35, 37]. To speak of GLP-1, a meta-analysis of Pichamol Jirapinyo et al. indicated that fasting levels remained unchanged while post-prandial GLP-1 levels increased after RYGB and the latter were negative related with alimentary limb length [48]. However, our meta-regression results did not support a relationship between ghrelin levels and RYGB surgical technical characteristics (including gastric pouch volume, alimentary limb length, and biliopancreatic limb length).
Limitations should be considered when interpreting our meta-analysis. First, the total number of included studies was only 16, with 325 patients having sufficient data. Second, comorbidities that could also affect ghrelin levels were found in many patients enrolled in the studies, including hypertension and asthma. Future study should focus on the relationship between post-RYGB weight change in longer term and ghrelin levels to further explore the effects of ghrelin on bariatric surgery.
Conclusions
On the basis of the current evidence, levels of ghrelin decreased in the short term (≤ 3 months) and increased in the long term (> 3 months) after RYGB. Meta-regression did not indicate associations between gastric pouch volume, alimentary limb length and biliopancreatic limb length, and ghrelin levels. Additional clinical trials with larger sample sizes and more available data with diverse time intervals may clarify these issues.
Change history
10 April 2019
This article was initially published with incorrect copyright information. Upon publication of this correction, the copyright of this article changed to “The Author(s).” The original article has been corrected.
References
Finucane MM, Stevens GA, Cowan MJ, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet. 2011;377(9765):557–67.
Bray GA, Fruhbeck G, Ryan DH, et al. Management of obesity. Lancet. 2016;387(10031):1947–56.
Suter M, Donadini A, Romy S, et al. Laparoscopic Roux-en-Y gastric bypass: significant long-term weight loss, improvement of obesity-related comorbidities and quality of life. Ann Surg. 2011;254(2):267–73.
Bariatric surgical procedures for obese and morbidly obese patients: a review of comparative clinical and cost-effectiveness, and guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2014.
Kalfarentzos F, Skroubis G, Karamanakos S, et al. Biliopancreatic diversion with Roux-en-Y gastric bypass and long limbs: advances in surgical treatment for super-obesity. Obes Surg. 2011;21(12):1849–58.
Steinert RE, Feinle-Bisset C, Asarian L, et al. Ghrelin, CCK, GLP-1, and PYY(3-36): secretory controls and physiological roles in eating and Glycemia in health, obesity, and after RYGB. Physiol Rev. 2017;97(1):411–63.
Pucci A, Batterham RL. Mechanisms underlying the weight loss effects of RYGB and SG: similar, yet different. J Endocrinol Investig; 2018.
Kojima M, Hosoda H, Date Y, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656–60.
Tschop M, Smiley DL, Heiman ML. Ghrelin induces adiposity in rodents. Nature. 2000;407(6806):908–13.
De Smet B, Depoortere I, Moechars D, et al. Energy homeostasis and gastric emptying in ghrelin knockout mice. J Pharmacol Exp Ther. 2006;316(1):431–9.
Theander-Carrillo C, Wiedmer P, Cettour-Rose P, et al. Ghrelin action in the brain controls adipocyte metabolism. J Clin Invest. 2006;116(7):1983–93.
Li Z, Xu G, Qin Y, et al. Ghrelin promotes hepatic lipogenesis by activation of mTOR-PPARgamma signaling pathway. Proc Natl Acad Sci U S A. 2014;111(36):13163–8.
Cummings DE, Purnell JQ, Frayo RS, et al. A preprandial rise in plasma ghrelin levels suggests a role in meal initiation in humans. Diabetes. 2001;50(8):1714–9.
Tschop M, Weyer C, Tataranni PA, et al. Circulating ghrelin levels are decreased in human obesity. Diabetes. 2001;50(4):707–9.
Garcia-Fuentes E, Garrido-Sanchez L, Garcia-Almeida JM, et al. Different effect of laparoscopic Roux-en-Y gastric bypass and open biliopancreatic diversion of Scopinaro on serum PYY and ghrelin levels. Obes Surg. 2008;18(11):1424–9.
Perez-Romero N, Serra A, Granada ML, et al. Effects of two variants of Roux-en-Y gastric bypass on metabolism behaviour: focus on plasma ghrelin concentrations over a 2-year follow-up. Obes Surg. 2010;20(5):600–9.
Cummings DE, Weigle DS, Frayo RS, et al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med. 2002;346(21):1623–30.
Korner J, Inabnet W, Febres G, et al. Prospective study of gut hormone and metabolic changes after adjustable gastric banding and Roux-en-Y gastric bypass. Int J Obes. 2009;33(7):786–95.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Chronaiou A, Tsoli M, Kehagias I, et al. Lower ghrelin levels and exaggerated postprandial peptide-YY, glucagon-like peptide-1, and insulin responses, after gastric fundus resection, in patients undergoing Roux-en-Y gastric bypass: a randomized clinical trial. Obes Surg. 2012;22(11):1761–70.
Olivan B, Teixeira J, Bose M, et al. Effect of weight loss by diet or gastric bypass surgery on peptide YY3-36 levels. Ann Surg. 2009;249(6):948–53.
O'Brien CS, Wang G, McGinty J, et al. Effects of gastrogastric fistula repair on weight loss and gut hormone levels. Obes Surg. 2013;23(8):1294–301.
Bryant EJ, King NA, Falken Y, et al. Relationships among tonic and episodic aspects of motivation to eat, gut peptides, and weight before and after bariatric surgery. Surg Obes Relat Dis. 2013;9(5):802–8.
Hansen EN, Tamboli RA, Isbell JM, et al. Role of the foregut in the early improvement in glucose tolerance and insulin sensitivity following Roux-en-Y gastric bypass surgery. Am J Physiol Gastrointest Liver Physiol. 2011;300(5):G795–802.
van der Zwaal EM, de Weijer BA, van de Giessen EM, et al. Striatal dopamine D2/3 receptor availability increases after long-term bariatric surgery-induced weight loss. Eur Neuropsychopharmacol. 2016;26(7):1190–200.
Carrasco F, Basfi-Fer K, Rojas P, et al. Changes in bone mineral density after sleeve gastrectomy or gastric bypass: relationships with variations in vitamin D, ghrelin, and adiponectin levels. Obes Surg. 2014;24(6):877–84.
Nosso G, Griffo E, Cotugno M, et al. Comparative effects of Roux-en-Y gastric bypass and sleeve gastrectomy on glucose homeostasis and incretin hormones in obese type 2 diabetic patients: a one-year prospective study. Horm Metab Res. 2016;48(5):312–7.
Mancini MC, Costa AP, de Melo ME, et al. Effect of gastric bypass on spontaneous growth hormone and ghrelin release profiles. Obesity (Silver Spring). 2006;14(3):383–7.
Bose M, Machineni S, Olivan B, et al. Superior appetite hormone profile after equivalent weight loss by gastric bypass compared to gastric banding. Obesity (Silver Spring). 2010;18(6):1085–91.
Kalinowski P, Paluszkiewicz R, Wroblewski T, et al. Ghrelin, leptin, and glycemic control after sleeve gastrectomy versus Roux-en-Y gastric bypass-results of a randomized clinical trial. Surg Obes Relat Dis. 2017;13(2):181–8.
Peterli R, Wolnerhanssen B, Peters T, et al. Improvement in glucose metabolism after bariatric surgery: comparison of laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy: a prospective randomized trial. Ann Surg. 2009;250(2):234–41.
Karamanakos SN, Vagenas K, Kalfarentzos F, et al. Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gastric bypass and sleeve gastrectomy: a prospective, double blind study. Ann Surg. 2008;247(3):401–7.
Terra X, Auguet T, Guiu-Jurado E, et al. Long-term changes in leptin, chemerin and ghrelin levels following different bariatric surgery procedures: Roux-en-Y gastric bypass and sleeve gastrectomy. Obes Surg. 2013;23(11):1790–8.
Zakeri R, Batterham RL. Potential mechanisms underlying the effect of bariatric surgery on eating behaviour. Curr Opin Endocrinol Diabetes Obes. 2018;25(1):3–11.
Williams DL, Grill HJ, Cummings DE, et al. Vagotomy dissociates short- and long-term controls of circulating ghrelin. Endocrinology. 2003;144(12):5184–7.
Sundbom M, Holdstock C, Engstrom BE, et al. Early changes in ghrelin following Roux-en-Y gastric bypass: influence of vagal nerve functionality? Obes Surg. 2007;17(3):304–10.
Lin E, Gletsu N, Fugate K, et al. The effects of gastric surgery on systemic ghrelin levels in the morbidly obese. Arch Surg. 2004;139(7):780–4.
Holdstock C, Engstrom BE, Ohrvall M, et al. Ghrelin and adipose tissue regulatory peptides: effect of gastric bypass surgery in obese humans. J Clin Endocrinol Metab. 2003;88(7):3177–83.
Seeley RJ, Chambers AP, Sandoval DA. The role of gut adaptation in the potent effects of multiple bariatric surgeries on obesity and diabetes. Cell Metab. 2015;21(3):369–78.
Abu Dayyeh BK, Jirapinyo P, Thompson CC. Plasma ghrelin levels and weight regain after Roux-en-Y gastric bypass surgery. Obes Surg. 2017;27(4):1031–6.
Tamboli RA, Breitman I, Marks-Shulman PA, et al. Early weight regain after gastric bypass does not affect insulin sensitivity but is associated with elevated ghrelin. Obesity (Silver Spring). 2014;22(7):1617–22.
Jirapinyo P, Jin DX, Qazi T, et al. A meta-analysis of GLP-1 after Roux-en-Y gastric bypass: impact of surgical technique and measurement strategy. Obes Surg. 2018;28(3):615–26.
Funding
This work received financial support from the National Natural Science Foundation of China (No. 31371168 and 31872791).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
Does not apply.
Informed Consent
Does not apply.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Supplementary Table 1
Search strategy. (DOCX 18 kb)
Supplementary Table 2
Quality assessment of included cohort studies. (DOCX 35 kb)
Supplementary Table 3
Baseline characteristics of the enrolled studies. (DOCX 40 kb)
Supplementary Figure 1
Quality assessment of included randomized controlled trials. Green: low risk of bias; Yellow: unclear risk of bias; Red: high risk of bias. (PNG 254 kb)
Rights and permissions
OpenAccess This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Xu, HC., Pang, YC., Chen, JW. et al. Systematic Review and Meta-analysis of the Change in Ghrelin Levels After Roux-en-Y Gastric Bypass. OBES SURG 29, 1343–1351 (2019). https://doi.org/10.1007/s11695-018-03686-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-03686-3