
Abstract
Background
Anastomotic stricture after gastric bypass for morbid obesity has been reported as the most frequent complication after surgery. The objective of this study is to determine in a prospective and consecutive endoscopic evaluation the true incidence of this complication early and late after gastric bypass.
Methods
A total of 441 morbidly obese patients were included in this prospective study. They were 358 women and 97 men, with a mean age of 41 years and a mean body mass index of 43 kg/m2. In all an endoscopic evaluation was performed 1 month after surgery, which was repeated in 315 patients (71.6%) 17 months after surgery, independent of the presence or not of symptoms. Anastomotic diameter was measured and strictures were classified as: (a) mild, with a diameter of 7 to 9 mm, (b) moderate with a diameter of 5 to 6 mm, and (c) difficult or critical with a diameter equal or less to 4 mm. Two methods of dilatation were employed: the endoscope itself or Savary–Gilliard dilators. Patients were submitted to laparotomic resectional gastric bypass in whom a circular stapler 25 was employed for gastrojejunal anastomosis or to laparoscopic gastric bypass, in whom hand-sewn one layer continuous suture was employed.
Results
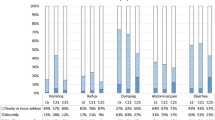
One month after surgery, 23% of patients after open gastric bypass employing circular stapler 25 presented anastomotic stricture, being 22% of them critical. After laparoscopic gastric bypass employing hand-sewn anastomosis, 36% of the patients presented strictures, being critical 10% (p > 0.17). Patients with mild or moderate strictures needed one or two dilatations. Patients with critical strictures needed three to five dilatations. There were no complications associated to dilatation. Moderate and severe strictures were symptomatic; however 29% of patients with mild strictures were asymptomatic. Endoscopy was repeated in 71% of the whole group 17 months after surgery, demonstrating normal anastomosis in all.
Conclusions
Stricture at the gastrojejunal anastomosis after gastric bypass is the commonest complication early after surgery. Near 60% present a mild stricture (with a diameter between 7 and 9 mm), being 28% asymptomatic. This complication is easily treated by endoscopic procedure if it is diagnosed early (3 to 4 weeks) after surgery. Routine endoscopy 1 month after surgery is the only objective scientific way to determine the real true incidence of this complication.
Similar content being viewed by others


References
Swartz DE, González V, Felix EL. Anastomotic stenosis after Roux-en-Y gastric bypass: a rational approach to treatment. Surg Obes Relat Dis. 2006;2:632–6.
Lujan JA, Frutos MD, Hernández Q, Cuenca JR, Valero G, Parrilla P. Experience with the circular stapler for the gastrojejunostomy in laparoscopic gastric bypass. Obes Surg. 2005;15:1096–102.
Catalano MF, Chua TY, Rudic G. Endoscopic balloon dilatation of stomal stenosis following gastric bypass. Obes Surg. 2007;17:298–303.
Schwartz ML, Drew RL, Roiger RW, Ketover SR, Chozen-Caldie M. Stenosis of the gastroenterostomy after laparoscopic gastric bypass. Obes Surg. 2004;14:484–91.
Vance PL, DeLange EE, Shaffer HA, Schirmer B. Gastric outlet obstruction following surgery for morbid obesity: efficacy of fluoroscopically guided balloon dilatation. Radiology 2002;222:70–2.
Bell RL, Reinhardt KE, Flowers JL. Surgeon performed endoscopic dilatation of symptomatic gastrojejunal anastomosis strictures following laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2003;13:728–33.
Szomstein S, Kaidar-Person O, Noberezny K, Cruz-Correa M, Rosenthal R. Correlation of radiographic and endoscopic evaluation of gastrojejunal anastomosis after Roux-en-y gastric bypass. Surg Obes Relat Dis. 2006;2:617–21.
Raman R, Raman B, Raman P, Rossiter S, Curet MJ, Mindelzun R, Morton JM. Abnormal findings on routine upper GI series following laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2007;17:311–6.
Carrodeguas L, Szomstein S, Zundel N, LoMenzo E, Rosenthal R. Gastrojejunal anastomotic strictures following laparoscopic Roux-en-Y gastric bypass surgery: analysis of 1291 patients. Surg Obes Relat Dis. 2006;2:92–7.
Escalona A, Devaud N, Boza C, Pérez G, Fernández J, Ibáñez L, Guzmán S. Gastrojejunal anastomotic stricture after Roux-en-Y gastric bypass: ambularoty management with the Savary-Gilliard dilator. Surg Endosc. 2007;21:765–8.
Peifer KJ, Shills AJ, Azar R, Rivera RE, Eagar JC, Jonnalagadda S. Successful endoscopic management of gastrojejunal anastomotic strictures after Roux-en-Y gastric bypass. Gastroint Endosc. 2007;66:248–56.
Nguyen NT, Stevens CM, Wolfe BM. Incidence and outcome of anastomotic stricture after laparoscopic gastric bypass. J Gastrointest Surg. 2003;7:997–1003.
Perugini RA, Mason R, Czerniach DR, Noirtsky YW, Baker S, Litwin DEM, Kelly JJ. Predictors of complication and suboptimal weight loss after laparoscopic Roux-en-Y gastric bypass. Arch Surg. 2003;138:541–6.
Ahmad J, Martin J, Ikamuddin S, Schau.er P, Seivka A. Endoscopic balloon dilation of gastroenteric anastomotic stricture after laparoscopic gastric bypass. Endoscopy 2003;35:725–8.
Rossi TR, Dynda DI, Ester NC, Marshall JS. Stricture dilation after laparoscopic Roux-en-Y gastric bypass. Am J Surg. 2005;189:357–60.
Blackstone RP, Rivera LA. Predicting stricture in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass: a logistic regression analysis. J Gastrointest Surg. 2007;11:403–9.
Csendes A, Burdiles P, Papapietro K, Díaz JC, Maluenda F, Burgos AM, Rojas J. Results of gastric bypass plus resection of the distal excluded gastric segment in patients with morbid obesity. J Gastrointest Surg. 2005;9:121–31.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Csendes, A., Burgos, A.M. & Burdiles, P. Incidence of Anastomotic Strictures after Gastric Bypass: A Prospective Consecutive Routine Endoscopic Study 1 Month and 17 Months After Surgery in 441 Patients with Morbid Obesity. OBES SURG 19, 269–273 (2009). https://doi.org/10.1007/s11695-008-9625-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9625-5