
Abstract
Objective
To evaluate the magnitude of the morbidity related to the system used for gastric banding Methods Between January 1997 and December 2004, 286 consecutive patients underwent laparoscopic gastric banding (LAGB) in one center. We used 4 models of LapBand® 9.75, 10, 11 and Vanguard with pars flacida route. Recalibration of band was performed in our consultation unit without systematic radiologic control. We considered four kinds of complication: port displacement, port rupture, band rupture and others problems.
Results
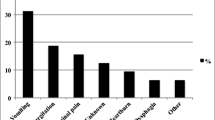
The mean follow up was 3.3±2.8 years with a median 2.9 years. Complications occurred within a mean time of 2.2±1.9 years. For the models vanguard and size 11, there were no rupture and 15 (27.7%) displacements whereas for size 9.75 and 10 there were 39 ruptures (14.7%) and 15 (5.6%) displacements. Types of complications were related to the bands used i.e. more port displacements for the models vanguard and size 11and more band and port ruptures for the models size 9.75 and 10. But when we considered the respective follow up according to the type of band these differences were no longer significant. Moreover rupture rate was significantly high but decreased after March 2002 because of changing of junction between port and catheter. Mean excess weight loss (35.2±27.7%) was not different in group whether the patients were reoperated or not.
Conclusion
Band and port related morbidity is an important aspect of bariatric surgery. We have to pay attention to material evolution and to our follow up for calibration. Some new recent technical advancement could improve the management of these patients.




Similar content being viewed by others

References
O’Brien PE, Dixon JB, Laurie C, Skinner S, Proietto J, McNeil J, et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial. Ann Intern Med. 2006;144:625–33.
Van Dielen FM, Soeters PB, de Brauw LM, Greve JW. Laparoscopic adjustable gastric banding versus open vertical banded gastroplasty: a prospective randomized trial. Obes Surg. 2005;15:1292–8.
Morino M, Toppino M, Bonnet G, del Genio G. Laparoscopic adjustable silicone gastric banding versus vertical banded gastroplasty in morbidly obese patients: a prospective randomized controlled clinical trial. Ann Surg. 2003;238:835–41.
O’Brien PE, McPhail T, Chaston TB, Dixon JB. Systematic review of medium-term weight loss after bariatric operations. Obes Surg. 2006;16:1032–40.
Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–37.
Basdevant A, Paita M, Rodde-Dunet MH, Marty M, Nogues F, Slim K, et al. A nationwide survey on bariatric surgery in France: two years prospective follow-up. Obes Surg. 2007;17:39–44.
Kwiatkowski F, Girard M, Hacène K, et al. SEM: a statistical software suitable for research in oncology. Bull Cancer. 2000;87:715–21.
Fried M, Peskova M, Kasalicky M. Bariatric surgery at First Surgical Department in Prague–Czech Republic–history and some technical aspects of the procedures. Sb Lek. 1998;99:291–5.
Belachew M, Legrand M, Vincent V, Lismonde M, Le Docte N, Deschamps V. Laparoscopic adjustable gastric banding. World J Surg. 1998;22:955–63.
Westling A, Bjurling K, Ohrvall M, Gustavsson S. Silicone-adjustable gastric banding: disappointing results. Obes Surg. 1998;8:467–74.
Kasalicky M, Fried M, Peskova M. Some complications after laparoscopic nonadjustable gastric banding. Obes Surg. 1999;9:443–5.
De Wit LT, Mathus-Vliegen L, Hey C, Rademaker B, Gouma DJ, Obertop H. Open versus laparoscopic adjustable silicone gastric banding: a prospective randomized trial for treatment of morbid obesity. Ann Surg. 1999;230:800–5; discussion 805–7.
Toppino M, Morino M, Bonnet G, Nigra I, Siliquini R. Laparoscopic surgery for morbid obesity: preliminary results from SICE registry (Italian Society of Endoscopic and Minimally Invasive Surgery). Obes Surg. 1999;9:62–5.
Suter M, Bettschart V, Giusti V, Heraief E, Jayet A. A 3-year experience with laparoscopic gastric banding for obesity. Surg Endosc. 2000;14:532–6.
Bajardi G, Ricevuto G, Mastrandrea G, Branca M, Rinaudo G, Cali F, et al. Surgical treatment of morbid obesity with biliopancreatic diversion and gastric banding: report on an 8-year experience involving 235 cases. Ann Chir. 2000;125:155–62.
Doldi SB, Micheletto G, Lattuada E, Zappa MA, Bona D, Sonvico U. Adjustable gastric banding: 5-year experience. Obes Surg. 2000;10:171–3.
Msika S. Surgery for morbid obesity: 2. Complications. Results of a technologic evaluation by the ANAES. J Chir. 2003;140:4–21.
Susmallian S, Ezri T, Elis M, Charuzi I. Access-port complications after laparoscopic gastric banding. Obes Surg. 2003;13:128–31.
Keidar A, Carmon E, Szold A, Abu-Abeid S. Port complications following laparoscopic adjustable gastric banding for morbid obesity. Obes Surg. 2005 Mar;15(3):361–5.
Chevallier JM, Zinzindohoué F, Douard R, Blanche JP, Berta JL, Altman JJ, et al. Complications after laparoscopic adjustable gastric banding for morbid obesity: experience with 1,000 patients over 7 years. Obes Surg. 2004 Mar;14(3):407–14.
Martin LF, Smits GJ, Greenstein RJ. Treating morbid obesity with laparoscopic adjustable gastric banding. Am J Surg. 2007 Sep;194(3):333–43; discussion 344–8.
Eid GM, Gourash W, Collins JL. A novel technique for fascial fixation of laparoscopic adjustable gastric band ports. Surg Endosc. 2006 Apr;20(4):697–9. Epub 2006 Jan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Launay-Savary, M.V., Slim, K., Brugère, C. et al. Band and Port-Related Morbidity After Bariatric Surgery: An Underestimated Problem. OBES SURG 18, 1406–1410 (2008). https://doi.org/10.1007/s11695-008-9493-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9493-z