
Abstract
Background
Patients frequently experience suboptimal transitions from the hospital to the community, which can increase the likelihood of readmission. It is not known which care coordination services can lead to improvements in readmission rates.
Objective
To evaluate the effects of two care coordination interventions on 30-day readmission rates.
Design
Prospective multicenter observational study of hospitalized patients eligible for two care coordination services between January 1, 2013, and October 31, 2015. Readmission rates were compared for patients who received each care coordination intervention versus those who did not using multivariable generalized estimating equation logistic regression models.
Participants
A total of 25,628 patients hospitalized in medicine, neurosciences, or surgical sciences units.
Interventions
Patients discharged home and deemed to be at high risk for readmission were assigned a nurse Transition Guide (TG) for 30 days post-discharge. All other patients were assigned the Patient Access Line (PAL) intervention, which provided a post-discharge phone call from a registered nurse.
Setting
Two large academic hospitals in Baltimore, MD.
Main Measures
Thirty-day all-cause readmission to any Maryland hospital.
Key Results
Among all patients, 14.2% (2409/16,993) of those referred for the PAL intervention and 22.8% (1973/8635) of those referred for the TG intervention were readmitted. PAL-referred patients who did not receive the intervention had an adjusted odds ratio (aOR) for readmission of 1.27 (95% confidence interval [95% CI] 1.12–1.44, p < 0.001) compared with patients who did. TG-referred patients who did not receive the TG intervention had an aOR of 1.83 (95% CI 1.60–2.10, p < 0.001) compared with patients who received the intervention. Younger age, male sex, having more comorbidities, and being discharged from a medicine unit were associated with not receiving an assigned intervention. These characteristics were also associated with higher readmission rates.
Conclusions
PAL and TG care coordination interventions were associated with lower rates of 30-day readmission. Our findings underscore the importance of determining the appropriate intervention for the hardest-to-reach patients, who are also at the highest risk of being readmitted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Over 30 million patients are discharged from US hospitals each year.1 Many of these patients experience deficits in care that result in poor outcomes. In particular, suboptimal transition from the hospital to the community setting has been recognized as a common source of care deficit.2 The Centers for Medicare & Medicaid Services (CMS) has sought to promote strategies that reduce healthcare costs, improve the quality of care, and improve the health of hospitalized patients.3
Hospitals often fail to integrate care processes when patients transition to receiving community-based services. Poor coordination of care transitions increases the risk of post-discharge complications, which sometimes result in unplanned rehospitalization.4 There are many reasons for avoidable readmission, including complex factors such as underlying comorbid conditions, socioeconomic characteristics, and health behaviors.5,6, – 7 A number of demonstration projects implemented by CMS and others have been shown to improve transitions of care through better communication within the healthcare team and with the patient around the time of discharge.8,9,10,11, – 12 These strategies include early risk screening to identify patients who warrant intensified post-discharge support services, promoting follow-up with primary or specialty care, patient education, optimized medication management, post-discharge phone calls, and transition coaches.13,14,15, – 16 While some studies have suggested improved outcomes, systematic reviews have reported mixed results overall. Thus it is unclear which interventions are effective in improving 30-day readmissions and whether it would be more effective to combine different interventions.16
This study was part of a larger effort evaluating a bundle of care coordination strategies implemented within the Johns Hopkins Health System.17 Efforts to improve care transitions began in 2010 and were augmented in 2012 through an award from the Center for Medicare & Medicaid Innovation (CMMI) to improve access to healthcare and care coordination processes for patients cared for at Johns Hopkins Hospital and Johns Hopkins Bayview Medical Center. The bundle of inpatient and post-acute care transition strategies was built on early demonstration projects and focused on interdisciplinary planning and prioritizing provider hand-offs. The interventions we evaluate here were the Transition Guides (TG) and Patient Access Line (PAL) interventions. Broad inclusion criteria were used, so that all patients discharged home without home care services were eligible to receive one of the two interventions. In brief, higher-risk patients were assigned to the TG intervention, which connected the patient with an RN who facilitated care and stayed in contact with the patient for 30 days following discharge, and when appropriate, would visit the patient at home to assist in self-care management. All other patients were assigned to the PAL intervention, which consisted in phone calls from specialized nurses to patients within 48 h of discharge to review the discharge instructions and identify potential problems (e.g. new symptoms or inability to get prescriptions filled). These calls often took over 20 min to complete and were intended to review discharge instructions in detail; if problems were identified, PAL nurses reached out to the discharging team.
In this study we sought to evaluate whether these coordination strategies were associated with a reduction in 30-day readmission to any hospital in the state of Maryland. We also sought to describe patient characteristics that were associated with receipt of an intervention, since not all patients assigned to interventions received them.
METHODS
Study Design, Population, and Setting
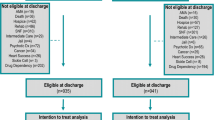
We conducted a prospective multicenter observational study of patients who were discharged from two urban academic medical centers and who were eligible for care coordination services to reduce 30-day readmissions. The two centers—The Johns Hopkins Hospital (JHH), a 1000-bed hospital, and the Johns Hopkins Bayview Medical Center (JHBMC), a 428-bed hospital—are urban academic medical centers in Baltimore, MD. Although the two provide similar levels of care, there are differences in the populations served. JHBMC provides care to an older patient population with a greater number of comorbid, chronic conditions and a higher proportion of Medicaid patients. Clinical units involved in this study were primarily in the departments of medicine, neurosciences, and surgical sciences across both campuses. Discharges occurred between January 1, 2013, and October 31, 2015, for patients referred for TG services, and between July 1, 2013, and October 31, 2015, for patients referred for PAL services. Patients discharged to other healthcare facilities (acute or subacute) and patients receiving skilled home care services were not eligible for these interventions, to avoid duplication of effort (Fig. 1).

Thirty-day readmission rates based on receipt or non-receipt of care coordination intervention. The diagram shows the number of patients who were referred for each intervention, based on risk screening (e.g. Early Screen for Discharge Planning [ESDP] score, care coordination rounds), as well as the unadjusted readmission scores for patients receiving versus not receiving the two interventions. Abbreviations: SNF, skilled nursing facility.
Care Coordination Strategies
The approach to transforming care coordination at both institutions included the goals of aligning daily care processes around the needs of all hospitalized patients, increasing accountability for patient outcomes, selecting an evidenced-based bundle of strategies based on patient risk, and engaging patients and families in taking responsibility for their own healthcare outcomes. The TG and PAL interventions were developed within this framework.
For both interventions, the interdisciplinary team, including care coordination case managers and social workers, participated in daily multidisciplinary rounds on the project nursing units and identified eligible patients. During these rounds, the care coordination team provided advice on transitional care to the inpatient providers and recommended post-discharge services. To help target the appropriate intervention, all patients admitted to the units underwent an early risk screening process using the Early Screen for Discharge Planning (ESDP), a decision support tool for identifying patients at high risk for post-discharge complications who might benefit from post-acute services and referrals.15 In general, patients with high ESDP scores (≥10) and those identified as high-risk through discussion at multidisciplinary rounds were offered higher-intensity services at discharge.
The TG intervention was targeted to patients identified as high risk for readmission, but who lacked skilled nursing needs to qualify for home care services or placement in a skilled nursing facility. TGs were home care nurses who were assigned to monitor, communicate, and, when needed, visit the patient at home for up to 30 days post-discharge. The role of the TG, modeled after the “transition coaches” used in Eric Coleman’s care transition program,13 was to assist patients and caregivers with post-discharge self-care management, including setting goals and identifying behaviors or barriers that might lead to self-care management failure. This was accomplished through individualized care: reinforcing discharge instructions, performing medication reconciliation, ensuring receipt of critical medication prescriptions, ensuring provider follow-up and transportation to post-discharge appointments, referring patients to post-acute care appointments for ongoing or new problems, recommending patient safety measures for the home environment, referring patients to community agencies for social needs, and facilitating hand-offs to primary care and medical home services.
Patients who were not deemed to be at high risk for post-discharge care management failure and those high-risk patients who refused the TG intervention were assigned to the PAL intervention: a single, structured post-discharge phone call from a trained nurse within 24–48 h after discharge. The PAL intervention was informed by prior studies such as Project RED (Re-Engineered Discharge).18 , 19 Using a structured survey tool, and guided by discharge instructions documented in the electronic health record, PAL nurses reviewed with patients key components of the discharge instructions. During the phone calls, nurses and patients discussed discharge medications, self-care management instructions, “red flag” signs and symptoms, and follow-up appointments and patients’ ability to keep them. Nurses were trained to use motivational interviewing and “teach-back” techniques to reinforce instructions and highlight important aspects of self-care management.20 When problems were discovered, PAL nurses could intervene by notifying the discharging providers and, if available, outpatient providers, and by making referrals for additional post-acute support, such as home care services. PAL calls typically lasted 20–30 min.
Primary Outcome: 30-Day Readmission
The primary outcome was unplanned rehospitalization to any acute-care hospital in Maryland within 30 days of discharge from the two project hospitals. All unplanned readmissions in Maryland are tracked, enabling the calculation of readmissions to both the same hospital and other hospitals.21 Unplanned readmissions were defined by the Maryland Health Services Cost Review Commission (HSCRC) using an algorithm to exclude readmissions that were likely scheduled, based on the index admission diagnosis and readmission diagnosis; this algorithm is based on the CMS all-cause readmission measure.22 , 23
Data Source and Covariates
Data were derived from several sources. Documentation of patient eligibility and receipt of the PAL and TG interventions were recorded in a Research Electronic Data Capture (REDCap) database. These data were updated daily. The Johns Hopkins Hospital CaseMix/Data Mart database, used for mandatory reporting to the state of Maryland, provided the following patient data: age, gender, race/ethnicity, payer (Medicare, Medicaid, other) as a proxy for socioeconomic status,24 hospital service upon discharge, hospital length of stay (LOS), Agency for Healthcare Research and Quality (AHRQ) comorbidity index (an updated version of the Elixhauser index25), and All-Patient–Refined Diagnosis-Related Group (APR-DRG) and severity of illness (SOI) combinations (3M Health Information Systems, Salt Lake City, UT).26 The Maryland HSCRC provided the state’s readmission rates for each APR-DRG/SOI combination, which served as the expected readmission rate. This risk stratification methodology is similar to the approach used in previous studies.27 , 28
Statistical Analysis
Analyses were performed separately for patients referred for PAL and TG interventions. Descriptive statistics were calculated for patient characteristics. Multivariable generalized estimating equation (GEE) logistic regression models were used to predict 30-day readmission while controlling for covariates: age, sex, race, payer, hospital service, AHRQ comorbidity index, LOS, HSCRC APR-DRG/SOI expected 30-day readmission rate, whether patients received the intervention, and the facility. The GEE models were used to account for the correlation between repeated observations occurring when a single patient had multiple admissions. Additionally, a propensity score analysis was performed as a sensitivity analysis. A patient’s propensity for receiving the intervention was calculated using GEE logistic regression, with the same covariates as noted above (entered non-parsimoniously) used as independent variables. The propensity score for each patient was then used as an adjustor variable to predict readmissions with each intervention. Separate multivariable GEE logistic regression models were also used to predict patient receipt versus non-receipt of the intervention while controlling for the covariates mentioned above. Adjusted odds ratios (ORs) were calculated for each regression model. Before its inclusion in the logistic regression model, we confirmed a lack of multicollinearity in the multivariable regression model using variance inflation factors. To determine the number needed to treat for each intervention, the GEE logistic regression models were used to calculate the absolute adjusted 30-day readmission rates for the patients who received the intervention versus those who did not. Statistical significance was defined as a two-sided p < 0.05. Data were analyzed with R (version 3.1; http://www.r-project.org). This study was approved by the Johns Hopkins Institutional Review Board.
RESULTS
Patient Characteristics
A total of 8635 and 16,993 patients were referred for the TG and PAL interventions, respectively. Figure 1 shows the number of patients who were referred for each intervention based on their risk assessment, as well as the unadjusted readmission rates for patients who received versus did not receive an intervention. The proportion of referred patients receiving the interventions was similar between the PAL and TG groups, with 64% and 60%, respectively. Consistent with the program’s risk stratification procedures, 78% (13,293/16,993) of PAL-referred patients had ESDP scores of <10, suggesting they were at lower risk for readmission prior to receiving the intervention than those receiving TGs, of whom 65% (5593/8635) had ESDP scores of <10. In addition to higher ESDP scores, patients referred to the TG intervention also had higher unadjusted readmission rates, as shown in Figure 1.
Table 1 shows the demographic and clinical characteristics of patients referred for PAL and TG interventions. Based on APR-DRG-designated severity of illness, TG-referred patients had a higher AHRQ comorbidity index, longer LOS, and a higher expected readmission rate than patients referred for PAL.
Patient Characteristics Associated with Receiving the Interventions
Table 2 shows the results of the adjusted analyses examining patient characteristics associated with not receiving the TG or PAL intervention. Among referred patients, factors significantly associated with a higher likelihood of not receiving the TG intervention included younger age, male sex, discharge from a medicine unit, having a greater number of comorbidities, and a higher expected readmission rate based on their APR-DRG-designated severity of illness. Similarly, factors significantly associated with a higher likelihood of not receiving the PAL intervention were younger age, male sex, black race, Medicaid insurance, discharge from a medicine unit, and having a greater number of comorbidities. We also observed a small but significant difference between hospital sites, in that patients at the JHBMC campus were less likely than JHH patients to receive either intervention.
Association Between Intervention Received and 30-Day Readmission
Table 3 summarizes the multivariable adjusted and propensity-adjusted analyses. Patients who received no intervention had a significantly higher likelihood of readmission than patients receiving an intervention. For PAL-referred patients, compared with patients who received the intervention, patients who did not receive the intervention had an adjusted OR and 95% confidence interval (95% CI) of 1.27 (95% CI 1.12–1.44, p < 0.001) and 1.24 (1.08–1.43, p = 0.003) of being readmitted within 30 days in the adjusted and propensity score-adjusted analyses, respectively. The number of patients needed to receive the PAL intervention to prevent one readmission was 50.0 (95% CI 43.5–58.8). Compared with TG-referred patients who received the intervention, patients who did not receive the intervention had an adjusted OR of 1.83 (95% CI 1.60–2.10, p < 0.001) and 1.81 (1.58–2.07, p < 0.001) of being readmitted within 30 days in the adjusted and propensity score-adjusted analyses, respectively. The number of patients needed to receive the TG intervention to prevent one readmission was 11.2 (95% CI 9.9–12.8).
DISCUSSION
We investigated the impact that two care coordination interventions had on 30-day readmissions in two academic medical centers in Maryland. Receipt of the TG intervention was associated with significantly lower readmission rates, which persisted after adjustment. The PAL intervention was associated with modestly lower readmission rates. Overall, this finding is consistent with the notion that managing patients with varying levels of care coordination interventions, based on risk assessment, may be an effective strategy for improving transitions from the hospital and reducing readmissions.
Although the causes of hospital readmission are numerous, preventing readmissions is largely dependent on a patient’s ability and willingness to carry out a series of complex and multifaceted self-care activities. We reasoned that the care coordination interventions at our institutions were successful because they were designed to assess a patient’s ability to perform self-care management and to assist patients when they were unable to do this for themselves. Patients targeted to receive the more intensive TG intervention frequently demonstrated poor health literacy, problems with activation, or socioeconomic barriers that rendered them likely to benefit from continuous nurse support. In comparison, the PAL intervention operated on the premise that all patients were potentially at risk for care transition failure soon after hospital discharge based on factors such as confusing or incomplete instructions, challenges in filling prescriptions for medications, or the presence of new signs or symptoms. Thus, in addition to assessing self-management skills, PAL nurses also identified problems that could increase patient risk for rehospitalization, such as identification of errors in medications, incorrect or faulty equipment, or difficulty making it to post-discharge follow-up appointments. These problems were able to be addressed in a timely manner by linking patients with providers, offering additional education, or connecting patients with resources in the community.
Our study has limitations. Although the findings suggest an association between the care coordination interventions and 30-day readmissions, our study design does not allow us to establish causation with certainty. Patients were not randomly allocated to receipt versus non-receipt of interventions, and we used as controls the patients we intended to reach but could not. Thus there may have been differences in unmeasured factors such as social or socioeconomic context that were important in determining whether the patient could be reached after discharge.29 , 30 We sought to minimize the risk for residual confounding by adjusting for a number of potentially important variables, and we did identify significant predictors of intervention receipt versus non-receipt. Interestingly, many of the same variables that predicted non-receipt of the assigned intervention (such as young age, male sex, and more comorbidities) also predicted higher readmission rates. This suggests that the most vulnerable patients may also be the hardest to reach and to engage in care coordination interventions. Hence, we recognize that the patients who received the interventions may have been more engaged in their care and more willing to work with the healthcare team to improve their health, leading to potential confounding by indication. This may explain why the magnitude of the reduction in risk for readmission that we observed for the TG intervention was larger than might have been expected based on previously reported research.16
These findings underscore the importance of determining how best to engage these hardest-to-reach patients. A large body of evidence shows that engaged patients tend to have better outcomes.31,32, – 33 We found that nearly two-thirds of referred patients received the interventions, which is higher than the conversion rates typically reported in the literature. Although we did not directly evaluate patient engagement in this study, it is important to identify strategies that care coordination teams can use to engage patients.
CONCLUSIONS
We showed that it was feasible to risk-stratify patients and to assign higher-risk patients to a more intensive care transition intervention. Further, successful delivery of care coordination interventions was associated with reduced 30-day readmissions. However, patients at highest risk for rehospitalization were also the least likely to receive the assigned care coordination intervention. This highlights the importance of finding ways to engage the hardest-to-reach patients in efforts to improve the transition from hospital to home.
References
Centers for Disease Control and Prevention (CDC). Prevalence of disabilities and associated health conditions among adults—United States, 1999. MMWR Morb Mortal Wkly Rep. 2001;50(7):120–5.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–7.
Center for Medicare and Medicaid Services. CMS strategy: The road forward 2013-2017. [Accessed on September 13, 2017]. 2013 (March):https://www.cms.gov/About-CMS/Agency-Information/CMS-Strategy/Downloads/CMS-Strategy.pdf.
Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392–7. doi: https://doi.org/10.1002/jhm.666.
Annema C, Luttik ML, Jaarsma T. Reasons for readmission in heart failure: Perspectives of patients, caregivers, cardiologists, and heart failure nurses. Heart Lung. 2009;38(5):427–34. doi: https://doi.org/10.1016/j.hrtlng.2008.12.002.
Auerbach AD, Kripalani S, Vasilevskis EE, et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med. 2016;176(4):484–93. doi: https://doi.org/10.1001/jamainternmed.2015.7863.
Long T, Genao I, Horwitz LI. Reasons for readmission in an underserved high-risk population: A qualitative analysis of a series of inpatient interviews. BMJ Open. 2013;3(9):e003212-2013-003212. doi: https://doi.org/10.1136/bmjopen-2013-003212.
Gage B, Smith L, Morley M, et al. Post-acute care payment reform demonstration report to congress supplement-interim report. Centers for Medicare & Medicaid Services; Baltimore: 2011;0209853.005.001.
Naylor MD. A decade of transitional care research with vulnerable elders. J Cardiovasc Nurs. 2000;14(3):1–14; quiz 88–9.
Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: A randomized clinical trial. JAMA. 1999;281(7):613–20.
Coleman EA, Min SJ, Chomiak A, Kramer AM. Posthospital care transitions: Patterns, complications, and risk identification. Health Serv Res. 2004;39(5):1449–65. doi: https://doi.org/10.1111/j.1475-6773.2004.00298.x.
Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364–70. doi: https://doi.org/10.1002/jhm.510.
Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: Results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–28.
Kind AJ, Jensen L, Barczi S, et al. Low-cost transitional care with nurse managers making mostly phone contact with patients cut rehospitalization at a VA hospital. Health Aff (Millwood). 2012;31(12):2659–68. doi: https://doi.org/10.1377/hlthaff.2012.0366.
Holland DE, Knafl GJ, Bowles KH. Targeting hospitalised patients for early discharge planning intervention. J Clin Nurs. 2013;22(19-20):2696–703. doi: https://doi.org/10.1111/j.1365-2702.2012.04221.x.
Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med. 2011;155(8):520–8.
Hoyer EH, Odonkor CA, Bhatia SN, Leung C, Deutschendorf A, Brotman DJ. Association between days to complete inpatient discharge summaries with all-payer hospital readmissions in Maryland. J Hosp Med. 2016;11(6):393–400. doi: https://doi.org/10.1002/jhm.2556.
Meyer J. Clinical management: A review of the evidence and policy recommendations. MARYLAND HEALTH SERVICES COST REVIEW COMMISSION [http://hscrc.maryland.gov/documents/commission-meeting/2014/07-09/post/3-Clinical-Management-Report-2014-07-03.pdf]. 2014 (July). Accessed September 13, 2017.
Berkowitz RE, Fang Z, Helfand BK, Jones RN, Schreiber R, Paasche-Orlow MK. Project ReEngineered Discharge (RED) lowers hospital readmissions of patients discharged from a skilled nursing facility. J Am Med Dir Assoc. 2013;14(10):736–40. doi: https://doi.org/10.1016/j.jamda.2013.03.004.
Labson MC. Innovative and successful approaches to improving care transitions from hospital to home. Home Healthc Now. 2015;33(2):88–95. doi: https://doi.org/10.1097/NHH.0000000000000182.
Gonzalez AA, Shih T, Dimick JB, Ghaferi AA. Using same-hospital readmission rates to estimate all-hospital readmission rates. J Am Coll Surg. 2014;219(4):656–63. doi: https://doi.org/10.1016/j.jamcollsurg.2014.05.008.
Centers for Medicare & Medicaid Services (CMS) The Joint Commission. Centers for Medicare & Medicaid services, and the Joint Commission. Specifications Manual for National hospital Inpatient Quality Measures, version 4.4 a_1. http://cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Measure-Methodology.html. Updated 2015 Jan. Accessed April, 7, 2015.
Centers for Medicare & Medicaid Services (CMS). Unplanned readmission: Hospital-wide, all-cause unplanned readmission rate (HWR).http://cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Measure-Methodology.html. Accessed September 13, 2017.
Adler NE, Newman K. Socioeconomic disparities in health: Pathways and policies. Health Aff (Millwood). 2002;21(2):60–76.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27.
Healthcare Cost and Utilization Project. NIS Description of Data Elements. Healthcare Cost and Utilization Project (HCUP). September 2008. Agency for Healthcare Research and Quality, Rockville, MD. https://www.hcup-us.ahrq.gov/db/vars/aprdrg/nisnote.jsp. Accessed September 13, 2017.
Hoyer EH, Needham DM, Miller J, Deutschendorf A, Friedman M, Brotman DJ. Functional status impairment is associated with unplanned readmissions. Arch Phys Med Rehabil. 2013;94(10):1951–8. doi: https://doi.org/10.1016/j.apmr.2013.05.028.
Oduyebo I, Lehmann CU, Pollack CE, et al. Association of self-reported hospital discharge handoffs with 30-day readmissions. JAMA Intern Med. 2013;173(8):624–9.
Kind AJ, Jencks S, Brock J, et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: A retrospective cohort study. Ann Intern Med. 2014;161(11):765–74. doi: https://doi.org/10.7326/M13-2946.
Werner RM, Goldman LE, Dudley RA. Comparison of change in quality of care between safety-net and non-safety-net hospitals. JAMA. 2008;299(18):2180–7. doi: https://doi.org/10.1001/jama.299.18.2180.
Hibbard JH, Greene J. What the evidence shows about patient activation: Better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013;32(2):207–14. doi: https://doi.org/10.1377/hlthaff.2012.1061.
Kangovi S, Mitra N, Grande D, et al. Patient-centered community health worker intervention to improve posthospital outcomes: A randomized clinical trial. JAMA Intern Med. 2014;174(4):535–43. doi: https://doi.org/10.1001/jamainternmed.2013.14327.
Greene J, Hibbard JH. Why does patient activation matter? an examination of the relationships between patient activation and health-related outcomes. J Gen Intern Med. 2012;27(5):520–6. doi: https://doi.org/10.1007/s11606-011-1931-2.
Acknowledgements
We thank Albert W. Wu, MD, MPH, for his review and comments during the preparation of this manuscript.
Funding
The project described was supported by grant number 1C1CMS331053-01-00 from the U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the U.S. Department of Health and Human Services or any of its agencies. The research presented was conducted by the awardee. Results may or may not be consistent with or confirmed by the findings of the independent evaluation contractor.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Hoyer, E.H., Brotman, D.J., Apfel, A. et al. Improving Outcomes After Hospitalization: A Prospective Observational Multicenter Evaluation of Care Coordination Strategies for Reducing 30-Day Readmissions to Maryland Hospitals. J GEN INTERN MED 33, 621–627 (2018). https://doi.org/10.1007/s11606-017-4218-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-017-4218-4