
ABSTRACT
BACKGROUND
The quality of code status discussions (CSDs) is suboptimal as physicians often fail to discuss patients’ goals of care and resuscitation outcomes. We previously demonstrated that internal medicine residents randomized to a communication skills intervention scored higher than controls on a CSD checklist using a standardized patient. However, the impact of this training on CSD content is unknown.
OBJECTIVE
Compare CSD content between intervention and control residents.
DESIGN
We conducted qualitative analysis of simulated CSDs. Augmenting a priori codes with constant comparative analysis, we identified key themes associated with resident determination of code status. We dichotomized each theme as present or absent. We used chi-square tests to evaluate the association between training and presence of each theme.
PARTICIPANTS
Fifty-six residents rotating on the internal medicine service in July 2010 were randomized to intervention (n = 25) or control (n = 31).
INTERVENTION
Intervention residents completed CSD skills training (lectures, deliberate practice, and self-study). Six months later, all 56 residents completed a simulated CSD.
MAIN MEASURE
Comparison of key themes identified in CSDs among intervention and controls.
KEY RESULTS
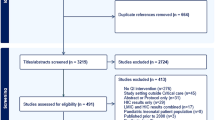
Fifty-one transcripts were recorded and reviewed. Themes identified included: exploration of patient values/goals, framing code status as a patient decision, discussion of resuscitation outcomes and quality of life, and making a recommendation regarding code status. Intervention residents were more likely than controls to explore patient values/goals (p = 0.002) and make a recommendation (p < 0.001); and less likely to frame the decision as one solely to be made by the patient (p = 0.01). Less than one-third of residents discussed resuscitation outcomes or quality of life.
CONCLUSION
Training positively influenced CSD content in key domains, including exploration of patient values/goals, making a recommendation regarding code status, and not framing code status as solely a patient decision. However, despite the intervention, residents infrequently discussed resuscitation outcomes and quality of life.

Similar content being viewed by others

REFERENCES
Tulsky JA, Chesney MA, Lo B. How do medical residents discuss resuscitation with patients? J Gen Intern Med. 1995;10(8):436–442.
Fischer GS, Tulsky JA, Rose MR, Siminoff LA, Arnold RM. Patient knowledge and physician predictions of treatment preferences after discussion of advance directives. J Gen Intern Med. 1998;13(7):447–454.
Gehlbach TG, Shinkunas LA, Forman-Hoffman VL, Thomas KW, Schmidt GA, Kaldjian LC. Code status orders and goals of care in the medical ICU. Chest. 2011;139(4):802–809.
Kaldjian LC, Erekson ZD, Haberle TH, et al. Code status discussions and goals of care among hospitalised adults. J Med Ethics. 2009;35(6):338–342.
Heyland DK, Frank C, Groll D, et al. Understanding cardiopulmonary resuscitation decision making: perspectives of seriously ill hospitalized patients and family members. Chest. 2006;130(2):419–428.
Loertscher LL, Beckman TJ, Cha SS, Reed DA. Code status discussions: agreement between internal medicine residents and hospitalized patients. Teach Learn Med. 2010;22(4):251–256.
Deep KS, Griffith CH, Wilson JF. Discussing preferences for cardiopulmonary resuscitation: what do resident physicians and their hospitalized patients think was decided? Patient Educ Couns. 2008;72(1):20–25.
Siddiqui MF, Holley JL. Residents’ practices and perceptions about do not resuscitate orders and pronouncing death: an opportunity for clinical training. Am J Hosp Palliat Care. 2011;28(2):94–97.
Deep KS, Griffith CH, Wilson JF. Communication and decision making about life-sustaining treatment: examining the experiences of resident physicians and seriously-ill hospitalized patients. J Gen Intern Med. 2008;23(11):1877–1882.
Alexander SC, Keitz SA, Sloane R, Tulsky JA. A controlled trial of a short course to improve residents’ communication with patients at the end of life. Acad Med. 2006;81(11):1008–1012.
Kelley AS, Back AL, Arnold RM, et al. Geritalk: communication skills training for geriatric and palliative medicine fellows. J Am Geriatr Soc. 2012;60(2):332–337.
Clayton JM, Butow PM, Waters A, et al. Evaluation of a novel individualised communication-skills training intervention to improve doctors’ confidence and skills in end-of-life communication. Palliat Med. 2012;27(3):236–243.
Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med. 2007;167(5):453–460.
Szmuilowicz E, El-Jawahri A, Chiappetta L, Kamdar M, Block S. Improving residents’ end-of-life communication skills with a short retreat: a randomized controlled trial. J Palliat Med. 2010;13(4):439–452.
Colletti L, Gruppen L, Barclay M, Stern D. Teaching students to break bad news. Am J Surg. 2001;182(1):20–23.
Williams DM, Fisicaro T, Veloski JJ, Berg D. Development and evaluation of a program to strengthen first year Residents’ proficiency in leading end-of-life discussions. Am J Hosp Palliat Care. 2011;28(5):328–334.
Han PK, Keranen LB, Lescisin DA, Arnold RM. The palliative care clinical evaluation exercise (CEX): an experience-based intervention for teaching end-of-life communication skills. Acad Med. 2005;80(7):669–676.
Szmuilowicz E, Neely KJ, Sharma RK, Cohen ER, McGaghie WC, Wayne DB. Improving residents’ code status discussion skills: a randomized trial. J Palliat Med. 2012;15(7):768–774.
Wayne DB, Moazed F, Cohen ER, Sharma RK, McGaghie WC, Szmuilowicz E. Code status discussion skill retention in internal medicine residents: one-year follow-up. J Palliat Med. 2012;15(12):1325–1328.
Downar J, Hawryluck L. What should we say when discussing “code status” and life support with a patient? A Delphi analysis. J Palliat Med. 2010;13(2):185–195.
White DB, Braddock CH III, Bereknyei S, Curtis JR. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med. 2007;167(5):461–467.
Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49(5):651–661.
Curtis JR, White DB. Practical guidance for evidence-based ICU family conferences. Chest. 2008;134(4):835–843.
Acknowledgements
We would like to thank all of the residents who participated in the study. Rashmi Sharma is supported in part by Grant Number K12 HD055884 from the Eunice Kennedy Shriver National Institute of Child Health & Human Development. Funding source: none. Data from this paper were presented at the Academy of Hospice and Palliative Medicine Annual Meeting in New Orleans, LA (15 March 2013) and at the Society of General Internal Medicine Annual Meeting in Denver, CO (25 April 2013).
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sharma, R.K., Jain, N., Peswani, N. et al. Unpacking Resident-Led Code Status Discussions: Results from a Mixed Methods Study. J GEN INTERN MED 29, 750–757 (2014). https://doi.org/10.1007/s11606-014-2791-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-014-2791-3