
Abstract
The COVID-19 pandemic elicited fear. The Fear of COVID-19 Scale (FCV-19S) is a newly developed self-reported measure, originally developed in Persian to assess COVID-19-related fear. To date, the scale has been translated and validated in 19 other languages, among which Greek. This study, conducted through an online survey, aimed to further explore the validity of the Greek FCV-19S version, as well as to identify appropriate cutoff scores. A total of 538 respondents completed the sociodemographic data sheet, the Generalized Anxiety Disorder 7-item scale, the Short Health Anxiety Inventory, and the Posttraumatic Stress Disorder-8 inventory. According to the results, a cutoff point score of 16.5 or higher revealed a significant predictive power for anxiety, health anxiety, and posttraumatic stress symptoms. Altogether, although the cutoff scores of the Greek FCV-19S version were explored to further evaluate the scale’s validity, they may facilitate discrimination of adults with extreme COVID-19-related fear from those with normal fear reactions.
Similar content being viewed by others


The first confirmed COVID-19 case was reported in Greece on February 26, 2020, i.e., 2 weeks before COVID-19 was declared a “pandemic” by the World Health Organization (WHO 2020). As early as the next day, the Greek government canceled Greek Carnival festivals, a measure to prevent the spread of COVID-19. While the number of COVID-19 positive cases was constantly rising, restriction measures, including selective suspension of schools and cancelation of cultural events, were, at first, taken regionally. After the first COVID-19-related death on March 12, restriction measures were gradually escalated. Eventually, a 6-week national lockdown was imposed on March 23, after 695 confirmed COVID-19 cases and 17 COVID-19-related deaths had been reported (National Public Health Organization 2020). In summary, the Greek government timely declared strict restriction measures, i.e., in less than a month after the announcement of the first COVID-19 case.
The ongoing COVID-19 pandemic has triggered a multilevel global crisis. A central feature of its psychological impact is perceived fear. Feelings of fear and fear-related behaviors are usually magnified in situations of mass threats and are addressed both in scientific papers and media reports. The term “coronaphobia,” initially coined by media agencies, refers to a “persistent and excessive fear” (Arpaci et al. 2020) or “dysfunctional anxiety” (Lee 2020a) related with the novel SARS-CoV-2 virus and, although not precisely defined, the term is mentioned in various scientific papers (Amin 2020a, 2020b; Asmundson and Taylor 2020; Naguy et al. 2020). Still, “coronaphobia” is not a novel term. Similar terminology has been used during previous infectious disease outbreaks to describe exaggerated mass reactions. For instance, the term “fearbola” during the Ebola epidemic has been argued to “reflect an overestimation of the likelihood and severity of contamination during a global outbreak” (Blakey et al. 2015, p. 817).
From an evolutionary perspective, fear is a significant emotion, operating as a warning signal. Namely, fear increases the chances of survival against a perceived danger or threat by triggering adaptive and defensive responses, which involve emotional, psycho-physiological, and behavioral patterns of arousal (Hamm 2019). Although fear and anxiety are generally considered distinct emotional states, they seem to be interlinked. This interrelation is also depicted in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classification of anxiety disorders, which are characterized by both fear and anxiety (American Psychiatric Association [APA], 2013). The biological bases and underlying behavioral mechanisms are similar (Hamm 2019; Steimer 2002), encompassing heightened physiological arousal (Hyde et al. 2019). A differentiating feature between fear and anxiety is the nature of the perceived threat. Fear is related with a known or impending threat, whereas anxiety is mainly related to an imprecise or unknown threat, as well as with the anticipation of future threats (APA, 2013).
Beyond the threat of potential infection, a pandemic encompasses a high degree of uncertainty, which further elicits feelings of arousal and hypervigilance. Fear of the unknown contributes to the manifestation of anxiety symptoms, worsening the mental health status of even healthy individuals (Shigemura et al. 2020). A direct adverse experience is not a prerequisite for experiencing fear, since even verbal cues perceived as aversive stimuli may evoke negative thoughts and elicit fear (Presti et al. 2020). Previous experience with infectious disease outbreaks offers some insight into the psychological burden imposed on the general population across all phases of a pandemic continuum. Specifically, persistent fear and fear-related responses may result in a high incidence of psychological morbidities, exacerbation of psychiatric symptoms, and even indirect mortality (Ornell et al. 2020), related with increased risk of developing suicidal ideation (Gunnell et al. 2020). In addition to the apparent uncertainty and the exposure to fear-appeal messages via the mass media, specific concerns and worries about health issues may further increase fear of COVID-19 (Mertens et al. 2020). Intense and prolonged stressors, such as own and family health concerns, may amplify fear and deteriorate mental health (Fiorillo and Gorwood 2020). Elevated fear may also be related to increased prevalence of Hikikomori syndrome, an acute and prolonged social withdrawal for at least six consecutive months, typically considered a Japanese culture-bound syndrome, yet with emerging evidence of its global extent (Kato et al. 2019; Macedo et al. 2017) to prevent contamination (Taylor and Asmundson 2020) or as another adverse outcome of the current pandemic (Kato et al. 2020). A recent systematic review and meta-analysis summarizing the psychological impact of previous and current coronavirus epidemics reports persistent psychiatric symptoms, especially in those who had been seriously ill (Rogers et al. 2020). Moreover, trauma experiences (e.g., severe illness, death of significant others, exposure to infected individuals) pose a greater risk for the development of posttraumatic stress disorder (PTSD) (Dutheil et al. 2020; Blekas et al. 2020; Mucci et al. 2020).
On the other side, research highlights the adaptive, “functional” role of fear, suggesting that fear may promote health-compliant responses (Harper et al. 2020). It is worth mentioning that during the Ebola virus epidemic, a study reported a positive correlation between fear and the willingness to take anti-Ebola vaccination (Mesch and Schwirian 2019). Along the same lines, fear-appeal theories indicate that fear arousal due to fear-appeal messages may have a positive effect on individuals, enhancing health-promoting behaviors (Tannenbaum et al. 2015; Williams 2012). According to this line of research, fear may lessen if the pandemic is not prolonged and if other risk factors (e.g., prior mental health difficulties) are not enduring (Harper et al. 2020).
Although there are no conclusive findings about the current pandemic’s psychological impact, continuous research has provided evidence that the COVID-19-related distress and fear may affect various aspects of life both during the acute and the forthcoming phases. A series of mental screeners have been developed to assess mental health (Ransing et al. 2020). The use of mental screeners is crucial for the early identification of individuals at risk (Karamouzi et al. 2020; Parlapani et al. 2020a), allowing more vigorous implementation of appropriate interventions (Pakpour and Griffiths 2020). One of the newly developed self-reported scales is the Fear of COVID-19 Scale (FCV-19S), originally validated in Persian by Ahorsu et al. (2020), assessing severity of the COVID-19-related fear. A scale’s advantage is its brief structure, rendering administration easy for clinical use and research purposes (Pakpour et al. 2020). This scale, the only available and validated in the Greek language (Tsipropoulou et al. 2020), has been translated and validated in 18 other languages, that is, in Argentinian Spanish (Alomo et al. 2020), Arabic (Alyami et al. 2020), Bangla (Sakib et al. 2020), Brazilian Portuguese (Faro et al. 2020), Chinese (Chi et al. 2020), Cuban Spanish (Broche-Pérez et al. 2020), English (Perz et al. 2020; Winter et al. 2020), French (Mailliez et al. 2020), Hebrew (Bitan et al. 2020), Indian (Doshi et al. 2020), Italian (Soraci et al. 2020), Japanese (Masuyama et al. 2020), Malay (Pang et al. 2020), Russian-Belarusian (Reznik et al. 2020), Spanish (Barrios et al. 2020; Huarcaya-Victoria et al. 2020; Martínez-Lorca et al. 2020), Tamil (Bharatharaj et al. 2020), Turkish (Haktanir et al. 2020; Satici et al. 2020), and Urdu (Mahmood et al. 2020). The unidimensionality of the FCV-19S scale has been widely evaluated, yet a bifactorial solution (i.e., emotional responses and physiological responses) has also been proposed (Barrios et al. 2020; Bitan et al. 2020; Chi et al. 2020; Huarcaya-Victoria et al. 2020; Masuyama et al. 2020).
Both the original scale and the translated versions support the scale’s adequate psychometric properties. Higher overall scores indicate elevated levels of fear related to COVID-19. However, to date, no optimal cutoff score has been proposed. Therefore, the aim of this study was to further explore the scale’s validity and to identify the appropriate cutoff point scores to facilitate study outcomes’ interpretation, by discriminating adults with extreme fear of COVID-19 from those with a normal fear reaction.
Methods
Participants and Survey Procedure
This cross-sectional study was carried out online 2 weeks after the national lockdown measures in Greece had been lifted. It comprises part of a second phase research project, following a study of the psychological impact of the COVID-19 pandemic on the Greek general population during the quarantine (Parlapani et al. 2020b). The authors contacted one of the co-developers of the FCV-19S scale (Ahorsu et al. 2020) who gave permission to carry out analyses to determine a cutoff score. After the original synthesis of the survey’s material, a survey sample was distributed to eight mental health professionals, five psychiatrists and three psychologists during the pre-survey phase, to ensure adequate comprehension of the survey’s scope and to explore potential difficulties related to the completion of the survey’s material.
The survey was distributed through social networking platforms during a 5-day period in late May, 2020. Members of the Greek general population were invited to join the study anonymously and voluntarily. Inclusion criteria were as follows: (i) consent to participate; (ii) being adult; (iii) Greek as a native language; and (iv) full completion of the survey questionnaires. A total of 538 respondents fulfilling inclusion criteria entered the study. A priori statistical power analysis for sample size estimation, with an alpha = 0.05 and power = 0.80, revealed that the sample size needed using Cohen’s (1988) criteria and the GPower 3.1 software (Faul et al. 2007) was approximately N = 186. Thus, the sample size of N = 538 was more than adequate for the main objective of this study.
The study was performed in accordance with the Declaration of Helsinki (World Medical Association 2001) and ethical approval was granted from the Papageorgiou General Hospital Review Board (563/2020) prior to data collection. Informed consent was obtained by all participants before their enrollment.
Measures
The survey included sociodemographic questions about gender, age, educational level, and residential area. In addition, participants completed the Greek versions of the following self-administered psychometric scales:
-
1.
The Fear of COVID-19 Scale (FCV-19S) (Ahorsu et al. 2020; Tsipropoulou et al. 2020): FCV-19S is a brief instrument consisting of seven items, e.g., item 1, “I am most afraid of coronavirus-19;” item 5, “When watching news and stories about coronavirus-19 on social media, I become nervous or anxious.” Responders are asked to indicate their level of agreement with each of the seven statements using a five-item Likert type scale (1 = strongly disagree to 5 = strongly agree). Total scores range from 7 to 35. The internal consistency in the current sample was 0.87.
-
2.
The Generalized Anxiety Disorder 7-item (GAD-7) scale (Spitzer et al. 2006; Skapinakis 2007): GAD-7 is a useful tool for screening for generalized anxiety disorder, assessing severity of anxiety symptoms over the past 2 weeks. It consists of seven items, e.g., item 1, “Feeling nervous, anxious or on edge;” item 7, “Feeling afraid as if something awful might happen.” Each item is rated on a four-point severity scale (0 = not at all; 1 = several days; 2 = more than half the days; 3 = nearly every day). Total scores range from 0 to 21. Higher scores indicate more severe anxiety symptoms. The internal consistency in the current sample was 0.79.
-
3.
The Short Health Anxiety Inventory (SHAI) (Salkovskis et al. 2002; Leonidou and Panayiotou 2016): SHAI is widely used to assess levels of health concern, as well as to identify individuals with hypochondriasis or severe health anxiety. The scale has been used in both clinical samples and samples of healthy individuals (Abramowitz et al. 2007; Alberts et al. 2011; Alberts et al. 2013). The main section consists of 14 sets of four-choice statements in a multiple-choice format with anchors from 0 to 3 representing health worries and attention on ordinary and unusual bodily sensations, e.g., item 5, “As a rule I am not afraid that I have a serious illness; I am sometimes afraid that I have a serious illness; I am often afraid that I have a serious illness; I am always afraid that I have a serious illness.” The scale includes four additional statement sets addressing perceived negative consequences of an illness. These are mainly used as a measure of a treatment process and were therefore not applicable in the current study. The items are summed to generate a total score with higher scores indicating greater health anxiety. A score of 18 is considered the optimal cutoff for the 14-item SHAI (Clark and Oates 2014; Morriss et al. 2019). The internal consistency in the current sample was 0.75.
-
4.
The Posttraumatic Stress Disorder-8 (PTSD-8) inventory (Hansen et al. 2010): PTSD-8 is a useful tool for screening for probable PTSD. The scale originates from the Harvard Trauma Questionnaire (HTQ) (Mollica et al. 1992). It consists of eight items, e.g., item 5, “Avoiding activities that remind you of the event.” Each item is rated on a four-point severity scale (0 = not at all; 1 = rarely; 2 = sometimes; 3 = most of the time). Instead of a fixed cutoff score, positive screening requires concurrent rating of at least one item from each symptom cluster with a score of three or higher. The PTSD-8 scale was validated in the Greek population in a previous study, conducted in 3029 individuals during the COVID-19 pandemic (Parlapani et al. 2020b). The scale was translated into Greek according to the forward-backward translation method, following principal guidelines (Sousa and Rojjanasrirat 2011; Tsang et al. 2017). Two independent healthcare professionals, fluent in English, conducted the forward translation. Both Greek versions were translated back into English by one bilingual and one fluent in English healthcare professional, both of whom were blinded to the English version. To assure semantic and conceptual equivalence, an expert panel of four members compared all versions to the original scale. Pretesting was conducted in 30 individuals recruited from the Papageorgiou General Hospital. A dichotomous response choice (clear, not clear) was used to evaluate clarity of expression and content adequacy. The final Greek PTSD-8 version included all recommended changes. To validate the Greek PTSD-8 version, the Peritraumatic Distress Inventory (PDI) (Brunet et al. 2001) was used; PDI consists of 13 items, e.g., item 1, “I felt helpless to do more,” exploring the level of distress experienced during a traumatic crisis or immediately thereafter. Items are rated on a 5-point Likert-type scale (0 = not true at all; 1 = slightly true; 2 = somewhat true; 3 = very true; 4 = absolutely true). The results of the Confirmatory Factor Analysis of the Greek PTSD-8 version were as follows: Chi-square goodness of fit test = χ2(20) = 562.88, p < 0.001; root mean square error of approximation (RMSEA) = 0.10, 90%; confidence intervals (CI) = [0.09, 0.10]; comparative fit index (CFI) = 0.87; Tucker Lewis index (TLI) = 0.82; standardized root mean square residual (SRMR) = 0.05. Convergent validity was established by correlating PTSD-8 with the PDI [rp = 0.69, p < 0.001, 95% CI (0.67, 0.71)]. The internal consistency in the current sample was 0.83.
Data Analysis
The current analysis focuses on the association between the FCV-19S scale and other variables relevant to the participants’ psychological reaction to COVID-19, including anxiety, health anxiety, and posttraumatic stress symptomatology. Missing values appearing sporadically were addressed by filling them in with a value corresponding to a randomly chosen comparable case with regard to gender, age, and educational level, that is, by using a random Hot Deck (Andridge and Little 2010). Demographic and clinical data were summarized using descriptive statistics.
Receiver operating characteristic (ROC) analysis was used to define cutoff values for the FCV-19S scale in relation to the above-mentioned variables serving as external criteria. The Youden-Index was used to determine the optimal cutoff score and to reduce the risk of misclassification.
A dichotomous variable was created out of the total GAD-7 using the cutoff point of 10 to assess anxiety (Patient Centered Primary Care Institute, n.d.). A dichotomous variable was created out of the total SHAI using the cutoff point of 18 to assess health anxiety (Morriss et al. 2019). Finally, to evaluate posttraumatic stress symptomatology, a dichotomous variable was created out of the total PTSD-8 with the criterion of probable PTSD diagnosis. After identifying the cutoff points, participants with a sum-score above the given cutoff value were considered cases with extreme fear. Those below were regarded as non-cases.
Results
Among the 538 participants, 419 were female (77.9%) and 119 male (22.1%). Women’s age (Mage = 42.70, SD = 11.29) was slightly lower than men’s (Mage = 43.38, SD = 11.78) with no statistical significance (t(528) = 0.783, p > 0.001). The majority of the participants had a university degree (38.7%) were married (53%), and lived in an urban area (88.5%). Detailed sociodemographic data are presented in Table 1.
The highest positive correlation of fear of COVID-19 (assessed by FCV-19S) was found with anxiety [assessed by GAD-7 (r = 0.715, p < 0.001)] and the lowest was found with health anxiety [assessed by SHAI (r = 0.472, p < 0.001)] (Table 2).
ROC curves were performed to explore the predictive validity of FCV-19S for anxiety, health anxiety, and posttraumatic stress symptomatology. A cutoff point of 16.5 based on ROC analyses for these dimensions revealed the following:
-
a)
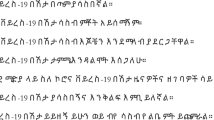
a significant predictive power of the FCV-19S scale for anxiety symptoms assessed by GAD-7 (anchor 1 = positive for anxiety) with AUC = 0.83, p < 0.001, 95% CI = 0.82–0.85, sensitivity 0.80, specificity 0.70, positive predictive values 62.7%, and negative predictive values 84.8% (Tables 3 and 4, Fig. 1).
-
b)
a significant predictive power of the FCV-19S scale for health anxiety symptoms assessed by SHAI (anchor 1 = positive for HA symptomatology) with AUC = 0.80, p < 0.001, 95% CI = 0.67–0.78, sensitivity 0.76, and specificity 0.68. A cutoff of 17.50 increased specificity (0.72) while retaining the rate of sensitivity, providing 76.5% positive predictive values and 72.5% negative predictive values (Tables 3 and 4, Fig. 1).
-
c)
a significant predictive power of the FCV-19S scale for posttraumatic stress symptomatology assessed by PTSD-8 (anchor 1 = probable PTSD diagnosis) with AUC = 0.88, p < 0.001, 95% CI = 0.78–0.85, sensitivity 0.94, and specificity 0.59. A cutoff of 18.50 decreased sensitivity (0.88) but increased specificity (0.72), providing 87.2% positive predictive values and 72.6% negative predictive values (Tables 3 and 4, Fig. 1).

ROC curves of FCV-19S for anxiety, health anxiety, and posttraumatic symptomatology
Based on the above results, 32.7% of the female participants and 7.8% of the male participants were classified as cases with elevated fear indicating that the majority of the participants experienced normal emotions of fear (Table 5).
Discussion
The purpose of determining a cutoff score for the Greek FCV-19S version was to develop the best criteria to discriminate adults with extreme fear of COVID-19 from those displaying a normal fear reaction. Although Ahorsu et al. pointed out in their original paper that the scale’s sensitivity and specificity could not be examined because the study participants originated from the general Iranian population, obtaining a cutoff score is a common practice in the psychiatry and psychology research field to enable classification of study participants into either cases or non-cases (Blanco et al. 2019; Ebrahimi et al. 2018; Lee 2020b; Oliveira et al. 2015; Silva et al. 2015). Despite widespread use of the FCV-19S scale worldwide, lack of a cutoff score limits the opportunity to compare study results and explore cultural differences between different populations, since a cutoff may facilitate both comparison and interpretation of research outcomes (Cook and Beckman 2006).
The results of this study nominated a cutoff of 16.5 or higher with AUC outcomes indicating moderate accuracy. Moreover, cutoff points showed significant predictive power for anxiety, health anxiety, and posttraumatic stress symptomatology. The strong relationship between the FCV-19S scale and anxiety has been demonstrated in recent studies (Harper et al. 2020; Tsipropoulou et al. 2020; Parlapani et al. 2020a, 2020b), proving the scale’s utility in identifying stressful emotions. Health anxiety symptomatology, an expected consequence of prolonged fear due to a perceived threat to health (Winter et al. 2020), was also related to a more severe fear of COVID-19 (Mertens et al. 2020). Therefore, determining a valid cutoff point with significant predictive power was of significance. Lastly, a fear construct is expected to have a significant predictive power of posttraumatic stress symptomatology, confirmed by current results as well, since the most common clinical manifestation of fear is PTSD (Gonzalez and Martinez 2014).
Different studies, conducted in other countries during the peak of the pandemic (e.g., Bangla (Sakib et al. 2020), English (Winter et al. 2020), Japanese (Masuyama et al. 2020), Hebrew (Bitan et al. 2020), Italian (Soraci et al. 2020), Russian-Belarusian (Reznik et al. 2020), and Turkish (Haktanir et al. 2020; Satici et al. 2020)), reported FCV-19S mean scores that exceeded the cutoff point score of 16.5, obtained from this study to distinguish elevated from normal fear of COVID-19. On the contrary, data from the current study, obtained after the recall of imposed measures, produced a lower overall mean compared with the proposed cutoff score, indicating that intense fear has been diminished. Still, a significant number of participants continue to suffer from elevated fear, as the pandemic crisis is not over yet.
It should be noted though that the current study exploring the cutoff scores was conducted for further evaluation of the scale’s validity and predicting ability, and not for diagnostic purposes. The criteria used here may not be the gold standard criteria for fear of COVID-19, due to lack of other instruments assessing the same construct while this study was being conducted. Anxiety, health anxiety, and PTSD scales were used as the most relevant. Therefore, the proposed cutoff point must be interpreted with caution. In addition, the present study had some limitations. The study’s cross-sectional design limited the opportunity to evaluate the effect of time on fear emotions. Convenience sampling used in this study may have limited results’ generalizability due to a “volunteer-effect” and the potential underrepresentation of less educated and socially disadvantaged individuals. Administration of self-reported questionnaires instead of clinician- administered interviews to address psychiatric symptomatology may have resulted in response bias. Lastly, women were overrepresented, roughly comprising four-fifths of the sample, something that may have influenced study results, since women were shown to display significantly higher levels of COVID-19-related fear compared with men (Parlapani et al. 2020b).
Conclusions
The FCV-19S is a scale that was timely developed published 2 weeks after the World Health Organization had declared COVID-19 a pandemic. The scale immediately captured the scientific interest of many researchers across the world, as it has been used to assess fear of COVID-19 while the pandemic was ongoing. This study provided empirical support for the scale’s adequacy to assess COVID-19-related fear and determined a cutoff point of 16.5 or higher with significant predictive power for anxiety, health anxiety, and posttraumatic stress symptomatology. Although the cutoff point is not proposed for diagnostic purposes, its application may enable a quick, primary screening for elevated fear to identify individuals that may be more vulnerable towards developing psychiatric symptomatology. Individuals with levels of fear exceeding the cutoff score may be further clinically assessed, to evaluate the psychological burden imposed by the pandemic. Such an approach may enhance the identification of at-risk individuals and therefore the prompt delivery of preventive and/or supportive interventions. Lastly, the extent to which COVID-19 continues to nurture longer-lasting feelings of fear remains to be investigated.
References
Abramowitz, J. S., Deacon, B. J., & Valentiner, D. P. (2007). The short health anxiety inventory: psychometric properties and construct validity in a non-clinical sample. Cognitive Therapy and Research, 31(6), 871–883. https://doi.org/10.1007/s10608-006-9058-1.
Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The fear of COVID-19 scale: development and initial validation. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00270-8.
Alberts, N. M., Hadjistavropoulos, H. D., Jones, S. L., & Sharpe, D. (2013). The short health anxiety inventory: a systematic review and meta-analysis. Journal of Anxiety Disorders, 27(1), 68–78. https://doi.org/10.1016/j.janxdis.2012.10.009.
Alberts, N. M., Sharpe, D., Kehler, M. D., & Hadjistavropoulos, H. D. (2011). Health anxiety: comparison of the latent structure in medical and non-medical samples. Journal of Anxiety Disorders, 25(4), 612–614. https://doi.org/10.1016/j.janxdis.2011.01.011.
Alomo, M., Gagliardi, G., Peloche, S., Somers, M., Alzina, P., & Prokopez, C. (2020). Actitudes y temores ante la pandemia por COVID-19 en Argentina [Attitudes and fears about COVID-19 pandemic in Argentina]. https://doi.org/10.13140/RG.2.2.13068.74881.
Alyami, M., Henning, M., Krägeloh, C. U., & Alayami, H. (2020). Psychometric evaluation of the Arabic version of the Fear of COVID-19 Scale. International Journal of Mental Health Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00316-x.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association. https://doi.org/10.1176/appi.books.9780890425596.
Amin, S. (2020a). The psychology of coronavirus fear: are healthcare professionals suffering from corona-phobia? International Journal of Healthcare Management, 1–8. https://doi.org/10.1080/20479700.2020.1765119.
Amin, S. (2020b). Why ignore the dark side of social media? A role of social media in spreading corona-phobia and psychological well-being. International Journal of Mental Health Promotion, 22(1), 29–38. https://doi.org/10.32604/IJMHP.2020.011115.
Andridge, R. R., & Little, R. J. A. (2010). A review of hot deck imputation for survey non-response. International Statistical Review, 78, 40–64. https://doi.org/10.1111/j.1751-5823.2010.00103.x.
Arpaci, I., Karataş, K., & Baloğlu, M. (2020). The development and initial tests for the psychometric properties of the COVID-19 Phobia Scale (C19P-S). Personality and Individual Differences, 164, Article 110108. https://doi.org/10.1016/j.paid.2020.110108.
Asmundson, G. J., & Taylor, S. (2020). Coronaphobia: Fear and the 2019-nCoV outbreak. Journal of Anxiety Disorders, 70, Article 102196. https://doi.org/10.1016/j.janxdis.2020.102196.
Barrios, I., Ríos-González, C., O’Higgins, M., González, I., García, O., Díaz, N. R., Castaldelli-Maia, J.M., Ventriglio, A., & Torales, J. (2020). Psychometric properties of the Spanish version of the Fear of COVID-19 Scale (FCV-19S). Research Square Preprints. https://doi.org/10.21203/rs.3.rs-33345/v1.
Bharatharaj, J., Alyami, M., Henning, M. A., Alyami, H., & Krägeloh, C. U. (2020). Tamil version of the Fear of COVID-19 Scale. Research Square Preprint. https://doi.org/10.21203/rs.3.rs-40914/v1.
Bitan, D. T., Grossman-Giron, A., Bloch, Y., Mayer, Y., Shiffman, N., & Mendlovic, S. (2020). Fear of COVID-19 scale: psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Research, Article 113100. https://doi.org/10.1016/j.psychres.2020.113100.
Blakey, S. M., Reuman, L., Jacoby, R. J., & Abramowitz, J. S. (2015). Tracing “Fearbola”: psychological predictors of anxious responding to the threat of Ebola. Cognitive Therapy and Research, 39(6), 816–825. https://doi.org/10.1007/s10608-015-9701-9.
Blanco, V., Guisande, M. A., Sánchez, M. T., Otero, P., & Vázquez, F. L. (2019). Spanish validation of the 10-item Connor–Davidson Resilience Scale (CD-RISC 10) with non-professional caregivers. Aging & Mental Health, 23(2), 183–188. https://doi.org/10.1080/13607863.2017.1399340.
Blekas, A., Voitsidis, P., Athanasiadou, M., Parlapani, E., Chatzigeorgiou, A. F., Skoupra, M., Syngelakis, M., Holeva, V., & Diakogiannis, I. (2020). COVID-19: PTSD symptoms in Greek healthcare professionals. Psychological Trauma: Theory, Research, Practice, and Policy. (TRA-2020-2091 [tra-1198]). In press.
Broche-Pérez, Y., Fernández-Fleites, Z., Jiménez-Puig, E., Fernández-Castillo, E., & Rodríguez-Martin, B. C. (2020). Gender and fear of COVID-19 in a Cuban population sample. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00377-y.
Brunet, A., Weiss, D. S., Metzler, T. J., Best, S. R., Neylan, T. C., Rogers, C., Fagan, J., & Marmar, C. R. (2001). The Peritraumatic distress inventory: a proposed measure of PTSD criterion A2. American Journal of Psychiatry, 158(9), 1480–1485. https://doi.org/10.1176/appi.ajp.158.9.1480.
Chi, X., Chen, S., Chen, Y., Chen, D., Yu, Q., Guo, T., Cao, Q., Zheng, X., Huang, S., Hossain, M., Stubbs, B., Yeung, A., & Zou, L. (2020). Psychometric evaluation of the Fear of COVID-19 Scale among Chinese population. PsyArXiv Preprints. https://doi.org/10.31234/osf.io/t5jne.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences, 2nd edn. Á/L.
Cook, D. A., & Beckman, T. J. (2006). Current concepts in validity and reliability for psychometric instruments: theory and application. The American Journal of Medicine, 119(2), 166.e7–166.e16. https://doi.org/10.1016/j.amjmed.2005.10.036.
Clark, D. M., & Oates, M. (2014). Improving access to psychological therapies: measuring improvement and recovery adult services. National Health Service England.
Doshi, D., Karunakar, P., Sukhabogi, J. R., Prasanna, J. S., & Mahajan, S. V. (2020). Assessing coronavirus fear in Indian population using the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00332-x.
Dutheil, F., Mondillon, L., & Navel, V. (2020). PTSD as the second tsunami of the SARS-Cov2 pandemic. Psychological Medicine, 1–2. https://doi.org/10.1017/S0033291720001336.
Ebrahimi, A., Rief, W., Mirshahzadeh, P., Zanjani, H. A., Dehsorkhi, H. N., Roohafza, H., Feizi, A., & Adibi, P. (2018). Psychometric properties of the Persian version of screening for Somatic Symptom Disorders-7 (SOMS-7). Iranian Journal of Psychiatry, 13(4), 264–273.
Faro, A., dos Santos Silva, L., dos Santos, D. N., & Feitosa, A. L. B. (2020). Adaptação e validação da Escala de Medo da COVID-19 [Adaptation and validation of the Fear of COVID-19 Scale]. SciELO Preprints. https://doi.org/10.1590/SciELOPreprints.898.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/bf03193146.
Fiorillo, A., & Gorwood, P. (2020). The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. European Psychiatry, 63(1), Article e32. https://doi.org/10.1192/j.eurpsy.2020.35.
Gonzalez, P., & Martinez, K. G. (2014). The role of stress and fear on the development of psychopathology. The Psychiatric Clinics of North America, 37(4), 535–546. https://doi.org/10.1016/j.psc.2014.08.010.
Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., Khan, M., O'Connor, R. C., Pirkis, J., & COVID-19 Suicide Prevention Research Collaboration. (2020). Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry, 7(6), 468–471. https://doi.org/10.1016/S2215-0366(20)30171-1.
Haktanir, A., Seki, T., & Dilmaç, B. (2020). Adaptation and evaluation of Turkish version of the Fear of COVID-19 Scale. Death Studies, 1–9. https://doi.org/10.1080/07481187.2020.1773026.
Hamm, A. O. (2019). Fear, anxiety, and their disorders from the perspective of psychophysiology. Psychophysiology, 57(2), Article e13474. https://doi.org/10.1111/psyp.13474.
Hansen, M., Andersen, T. E., Armour, C., Elklit, A., Palic, S., & Mackrill, T. (2010). PTSD-8: a short PTSD inventory. Clinical Practice and Epidemiology in Mental Health, 6(1), 101–108. https://doi.org/10.2174/1745017901006010101.
Harper, C. A., Satchell, L. P., Fido, D., & Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID-19 pandemic. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00281-5.
Huarcaya-Victoria, J., Villarreal-Zegarra, D., Podestà, A., Luna-Cuadros, M. A. (2020). Psychometric properties of a Spanish version of the Fear of COVID-19 Scale in general population of Lima, Peru. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00354-5.
Hyde, J., Ryan, K. M., & Waters, A. M. (2019). Psychophysiological markers of fear and anxiety. Current Psychiatry Reports, 21(7), 56. https://doi.org/10.1007/s11920-019-1036-x.
Κaramouzi, P., Parlapani, E., Nikopoulou, V. A., Giazkoulidou, A., Tsipropoulou, V., Pampouchidou, M., Asaridou, M., Holeva, V., & Diakogiannis, I. (2020). Quarantine in Greece: How living with the wrong person impacts mental health. ResearchGate Preprint. https://doi.org/10.13140/RG.2.2.21465.95842.
Kato, T. A., Kanba, S., & Teo, A. R. (2019). Hikikomori: multidimensional understanding, assessment, and future international perspectives. Psychiatry and Clinical Neurosciences, 73(8), 427–440. https://doi.org/10.1111/pcn.12895.
Kato, T. A., Sartorius, N., & Shinfuku, N. (2020). Forced social isolation due to COVID-19 and consequent mental health problems: lessons from hikikomori. Psychiatry and Clinical Neurosciences. Advance online publication, 74, 506–507. https://doi.org/10.1111/pcn.13112.
Lee, S. A. (2020a). Measuring coronaphobia: the psychological basis of the Coronavirus Anxiety Scale. Neurological Sciences, 33, 0–0. https://doi.org/10.14744/DAJPNS.2020.00069.
Lee, S. A. (2020b). Coronavirus Anxiety Scale: a brief mental health screener for COVID-19 related anxiety. Death Studies, 44(7), 393–401. https://doi.org/10.1080/07481187.2020.1748481.
Leonidou, C., & Panayiotou, G. (2016). Assessing health anxiety with the Greek SHAI: psychometric properties and identification of correlates and predictors. European Health Psychologist, 18(S), 526.
Macedo, P., Pimenta, V., Alves, M., Uria, A. S. R., & Salgado, H. (2017). Hikikomori goes global: a Portuguese case. European Psychiatry, 41(S1), S514. https://doi.org/10.1016/j.eurpsy.2017.01.670.
Mahmood, Q. K., Jafree, S. R., & Qureshi, W. A. (2020). The psychometric validation of FCV19S in Urdu and socio-demographic association with fear in the people of the Khyber Pakhtunkhwa (KPK) province in Pakistan. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00371-4.
Mailliez, M., Griffiths, M. D., & Carre, A. (2020). Validation of the French version of the Fear of COVID-19 Scale and its associations with depression, anxiety and differential emotions. Research Square Preprint. https://doi.org/10.21203/rs.3.rs-46616/v1.
Martínez-Lorca, M., Martínez-Lorca, A., Criado-Álvarez, J. J., & Armesilla, M. D. C. (2020). The Fear of COVID-19 Scale: Validation in Spanish university students. Psychiatry Research, 293, Article 113350. https://doi.org/10.1016/j.psychres.2020.113350.
Masuyama, A., Shinkawa, H., & Kubo, T. (2020). Development and validation of the Japanese version Fear of COVID-19 Scale among adolescents. PsyArXiv Preprint. https://doi.org/10.31234/osf.io/jkmut.
Mertens, G., Gerritsen, L., Duijndam, S., Salemink, E., & Engelhard, I. M. (2020). Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. Journal of Anxiety Disorders, 74, Article 102258. https://doi.org/10.1016/j.janxdis.2020.102258.
Mesch, G. S., & Schwirian, K. P. (2019). Vaccination hesitancy: Fear, trust, and exposure expectancy of an Ebola outbreak. Heliyon, 5(7), Article e02016. https://doi.org/10.1016/j.heliyon.2019.e02016.
Mollica, R. F., Caspi-Yavin, Y., Bollini, P., Truong, T., Tor, S., & Lavelle, J. (1992). The Harvard Trauma Questionnaire: validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees. Journal of Nervous and Mental Disease, 180(2), 111–116. https://doi.org/10.1097/00005053-199202000-00008.
Morriss, R., Patel, S., Malins, S., Guo, B., Higton, F., James, M., Wu, M., Brown, P., Boycott, N., Kaylor-Hughes, C., Morris, M., Rowley, E., Simpson, J., Smart, D., Stubley, M., Kai, J., & Tyrer, H. (2019). Clinical and economic outcomes of remotely delivered cognitive behaviour therapy versus treatment as usual for repeat unscheduled care users with severe health anxiety: a multicentre randomised controlled trial. BMC Medicine, 17(1), Article 16. https://doi.org/10.1186/s12916-019-1253-5.
Mucci, F., Mucci, N., & Diolaiuti, F. (2020). Lockdown and isolation: psychological aspects of COVID-19 pandemic in the general population. Clinical Neuropsychiatry: Journal of Treatment Evaluation, 17(2), 63–64. https://doi.org/10.36131/CN20200205.
Naguy, A., Moodliar-Rensburg, S., & Alamiri, B. (2020). Coronaphobia and chronophobia – a psychiatric perspective. Asian Journal of Psychiatry, 51, Article 102050. https://doi.org/10.1016/j.ajp.2020.102050.
National Public Health Organization. (2020). Current state of Covid-19 outbreak in Greece and timeline of key containment events. https://eody.gov.gr/en/current-state-of-covid-19-outbreak-in-greece-and-timeline-of-key-containment-events/.
Oliveira, M. A., Bendo, C. B., Paiva, S. M., Vale, M. P., & Serra-Negra, J. M. (2015). Determining cut-off points for the dental fear survey. The Scientific World Journal, 2015, Article 983564. https://doi.org/10.1155/2015/983564.
Ornell, F., Schuch, J. B., Sordi, A. O., & Kessler, F. H. P. (2020). “Pandemic fear” and COVID-19: mental health burden and strategies. Brazilian Journal of Psychiatry, 42(3), 232–235. https://doi.org/10.1590/1516-4446-2020-0008.
Pakpour, A. H., & Griffiths, M. D. (2020). The fear of COVID-19 and its role in preventive behaviors. Journal of Concurrent Disorders. https://concurrentdisorders.ca/2020/04/03/the-fear-of-covid-19-and-its-role-in-preventive-behaviors/.
Pakpour, A. H., Griffiths, M. D., & Lin, C. Y. (2020). Assessing psychological response to the COVID-19: the Fear of COVID-19 Scale and the COVID Stress Scales. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00334-9.
Pang, N. T. P., Kamu, A., Hambali, N. L. B., Mun, H. C., Kassim, M. A., Mohamed, N. H., Ayu, F., Rahim, S. S. S. A., Omar, A., & Jeffree, M. S. (2020). Malay version of the Fear of COVID-19 Scale: validity and reliability. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00355-4.
Parlapani, E., Holeva, V., Nikopoulou, V. A., Sereslis, K., Athanasiadou, M., Godosidis, A., Stephanou, T., & Diakogiannis, I. (2020a). Intolerance of uncertainty and loneliness in older adults during the COVID-19 pandemic. Frontiers in Psychiatry. Advance online publication. https://doi.org/10.3389/fpsyt.2020.00842.
Parlapani, E., Holeva, V., Voitsidis, P., Blekas, A., Gliatas, I., Porfyri, G. N., Golemis, A., Papadopoulou, K., Dimitriadou, A., Chatzigeorgiou, A. F., Bairachtari, V., Patsiala, S., Skoupra, M., Papigkioti, K., Kafetzopoulou, C., & Diakogiannis, I. (2020b). Fear of COVID-19 and behavioral responses to the pandemic in a Greek population. Frontiers in Psychiatry. Advance online publication. https://doi.org/10.3389/fpsyt.2020.00821.
Patient Centered Primary Care Institute. (n.d.). Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures. https://www.phqscreeners.com/images/sites/g/files/g10016261/f/201412/instructions.pdf.
Perz, C. A., Lang, B. A., & Harrington, R. (2020). Validation of the Fear of COVID-19 Scale in a US college sample. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00356-3.
Presti, G., McHugh, L., Gloster, A., Karekla, M., & Hayes, S. C. (2020). The dynamics of fear at the time of COVID-19: a contextual behavioral science perspective. Clinical Neuropsychiatry, 17(2), 65–71. https://doi.org/10.36131/CN20200206.
Ransing, R., Ramalho, R., Orsolini, L., Adiukwu, F., Gonzalez-Diaz, J. M., Larnaout, A., Pinto da Costa, M., Grandinetti, P., Drita Bytyçi, D. G., Shalbafanm, M., Patil, I., Nofal, M., Pereira-Sanchezo, V., & Kilic, O. (2020). Can COVID-19 related mental health issues be measured? Brain, Behavior, and Immunity, 88, 32–34. https://doi.org/10.1016/j.bbi.2020.05.049.
Reznik, A., Gritsenko, V., Konstantinov, V., Khamenka, N., & Isralowitz, R. (2020). COVID-19 fear in Eastern Europe: validation of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00283-3.
Rogers, J. P., Chesney, E., Oliver, D., Pollak, T. A., McGuire, P., Fusar-Poli, P., Zandi, M. S., Lewis, G., & David, A. S. (2020). Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. The Lancet Psychiatry, 7(7), 611–627. https://doi.org/10.1016/S2215-0366(20)30203-0.
Sakib, N., Bhuiyan, A .K. M. I., Hossain, S., Al Mamun, F., Hosen, I., Abdullah, A. H., Sarker, M. A., Mohiuddin, M. S., Rayhan, I., Hossain, M., Sikder, M. T., Gozal, D., Muhit, M., Islam, S. M. S., Griffiths, M. D., Pakpour, A. H., & Mamun, M. A. (2020). Psychometric validation of the Bangla Fear of COVID-19 Scale: confirmatory factor analysis and Rasch analysis. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00289-x.
Salkovskis, P. M., Rimes, K. A., Warwick, H. M. C., & Clark, D. M. (2002). The Health Anxiety Inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine, 32(5), 843–853. https://doi.org/10.1017/S0033291702005822.
Satici, B., Gocet-Tekin, E., Deniz, M. E., & Satici, A. S. (2020). Adaptation of the Fear of COVID-19 Scale: its association with psychological distress and life satisfaction in Turkey. International Journal of Mental Health Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00294-0.
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., & Benedek, D. M. (2020). Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry and Clinical Neurosciences, 74(4), 281–282. https://doi.org/10.1111/pcn.12988.
Silva, T. B., Osório, F. L., & Loureiro, S. R. (2015). SDQ: discriminative validity and diagnostic potential. Frontiers in Psychology, 6, 811. https://doi.org/10.3389/fpsyg.2015.00811.
Skapinakis, P. (2007). The 2-item Generalized Anxiety Disorder scale had high sensitivity and specificity for detecting GAD in primary care. Evidence-Based Medicine, 12(5), 149–149. https://doi.org/10.1136/ebm.12.5.149.
Soraci, P., Ferrari, A., Abbiati, F. A., Del Fante, E., De Pace, R., Urso, A., & Griffiths, M. D. (2020). Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00277-1.
Sousa, V. D., & Rojjanasrirat, W. (2011). Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: α clear and user-friendly guideline. Journal of Εvaluation in Clinical Practice, 17(2), 268–274. https://doi.org/10.1111/j.1365-2753.2010.01434.x.
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092.
Steimer, T. (2002). The biology of fear- and anxiety-related behaviors. Dialogues in Clinical Neuroscience, 4(3), 231–249.
Tannenbaum, M. B., Hepler, J., Zimmerman, R. S., Saul, L., Jacobs, S., Wilson, K., & Albarracín, D. (2015). Appealing to fear: a meta-analysis of fear appeal effectiveness and theories. Psychological Bulletin, 141(6), 1178–1204. https://doi.org/10.1037/a0039729.
Taylor, S., & Asmundson, G. J. (2020). Life in a post-pandemic world: what to expect of anxiety-related conditions and their treatment. Journal of Anxiety Disorders, 72, Article 102231. https://doi.org/10.1016/j.janxdis.2020.102231.
Tsang, S., Royse, C. F., & Terkawi, A. S. (2017). Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi Journal of Anaesthesia, 11(5), 80–89. https://doi.org/10.4103/sja.SJA_203_17.
Tsipropoulou, V., Nikopoulou, V. A., Holeva, V., Nasika, Z., Diakogiannis, I., Sakka, S., Kostikidou, S., Varvara, C., Spyridopoulou, E., & Parlapani, E. (2020). Psychometric properties of the Greek version of FCV-19S. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00319-8.
World Health Organization. (2020). WHO announces COVID-19 disease outbreak a pandemic. Mar 12, 2020. http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
Williams, K. C. (2012). Fear appeal theory. Research in Business and Economics Journal, 5(1), 1–21.
Winter, T., Riordan, B., Pakpour, A., Griffiths, M., Mason, A., Poulgrain, J., & Damian, S. (2020). Evaluation of the English version of the Fear of COVID-19 Scale and its relationship with behavior change and political beliefs. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.31234/osf.io/mvtd8.
World Medical Association. (2001). World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bulletin of the World Health Organization, 79(4), 373–374 https://apps.who.int/iris/handle/10665/268312.
Author information
Authors and Affiliations
Contributions
Study planning: V. Holeva and E. Parlapani. Study plan validation: P. Karamouzi. Project implication: P. Voitsidis and A. Blekas. Data interpretation: G. Porfyri. Data analysis: K. Papigkioti and S. Patsiala. Writing the first draft: V. A. Nikopoulou. Review and edit: V. Holeva and E. Parlapani. Final approval: I. Diakogiannis.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nikopoulou, V.A., Holeva, V., Parlapani, E. et al. Mental Health Screening for COVID-19: a Proposed Cutoff Score for the Greek Version of the Fear of COVID-19 Scale (FCV-19S). Int J Ment Health Addiction 20, 907–920 (2022). https://doi.org/10.1007/s11469-020-00414-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-020-00414-w