
Abstract
Introduction
Notwithstanding proven renoprotection from RAAS blockade (AB) with ACE inhibitors and ARBs, and despite increasing utilization of AB in the US, we have continued to experience a CKD/ESRD epidemic. Given concerns for iatrogenic CKD/ESRD, we designed a prospective study to analyze the course of eGFR following withdrawal of AB in such patients.
Patients
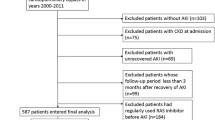
Between September 2002 and February 2005, all consecutive CKD patients on AB presenting with >25% increase in baseline serum creatinine were enrolled. eGFR following withdrawal of AB was monitored. The main outcome measures were serum creatinine, MDRD eGFR, and UA/Cr.
Results
100 Caucasians, M:F = 52:48, mean age 71.5 years were enrolled. Mean follow up was 26 months. Sixteen patients progressed to ESRD, of whom seven died. In 74, eGFR improved from 23.9 ± 9 (7–47) to 39.2 ± 15.4 (17–89) ml/min/1.73 m2 BSA, 26.5 (3–46) months after stopping AB (P = 0.001). The majority of the cohort, 95 patients, had known risk factors: 26 with RAS, 12 hypovolemia, 11 sepsis, 10 NSAIDs/cox II inhibtor use/abuse, 7 CIN, 2 congestive heart failure, 2 obstructive uropathy, and 27 with other medical and surgical causes, including malignancies, postoperative states, and infections. In the 26 with RAS, 5 with higher baseline creatinine −2.1 ± 0.6 versus 1.5 ± 0.4 mg/dL, P = 0.013, progressed to ESRD; 4/5 ESRD patients died after 6.3 months. The remaining five patients (one male and four females), mean age 68 (44–83) years, demonstrated sustained improved eGFR with discontinuation (four) or reduction (one) of RAAS blockade, despite normal renal arteries and the absence of known traditional risk factors. UA/Cr generally increased following withdrawal of AB.
Conclusions
Worsening azotemia in older susceptible CKD patients on AB, often but not always associated with known precipitating risk factors, remains under-recognized. Sustained improved eGFR often follows the discontinuation of AB. The practising physician should be well aware of these syndromes. Our observations call for further study.


Similar content being viewed by others


Abbreviations
- AB:
-
RAAS blockade
- ACEIs:
-
Angiotensin converting enzyme inhibitors
- ARBs:
-
Angiotensin receptor blockers
- CIN:
-
Contrast-induced nephropathy
- CKD:
-
Chronic kidney disease
- eGFR:
-
Estimated glomerular filtration rate by MDRD formula (ml/min/1.73 m2 BSA)
- ESRD:
-
End stage renal disease
- HD:
-
Hemodialysis
- LORFFAB:
-
Late-onset renal failure from angiotensin blockade
- MABP:
-
Mean arterial blood pressure
- MDRD:
-
Modification of diet in renal disease study group formula for GFR prediction
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- PTA:
-
Percutaneous transluminal angioplasty
- RAAS:
-
Renin angiotensin aldosterone system
- RAS:
-
Renal artery stenosis
- SCr:
-
Serum creatinine
- UA/Cr:
-
Urine albumin creatinine ration (mg/g)
References
Onuigbo M, Weir MR (2003) Evidence-based treatment of hypertension in patients with diabetes mellitus. Diabetes Obes Metab 5(1):13–26
Lewis EJ, Hunsicker LG, Bain RP et al (1993) The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med 329(20):1456–1462. (Erratum in: N Engl J Med 330(2):152
Ruggenenti P, Perna A, Gherardi G et al (1999) Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria. Lancet 354(9176):359–364
Brenner BM, Cooper ME, de Zeeuw D et al (2001) Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345:861–869
Lewis EJ, Hunsicker LG, Clarke WR et al (2001) Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345:851–860
Nelson CR, Knapp DA (2000) Trends in antihypertensive drug therapy of ambulatory patients by US office-based physicians. Hypertension 36(4):600–603
Jones CA, Krolewski AS, Rogus J et al (2005) Epidemic of end-stage renal disease in people with diabetes in the United States population: do we know the cause? Kidney Int 67(5):1684–1691
Centers for Disease Control, Prevention (CDC) (2007) Prevalence of chronic kidney disease and associated risk factors—United States, 1999–2004. MMWR Morb Mortal Wkly Rep 56(8):161–165
Pfeffer MA, Swedberg K, Granger CB et al (2003) Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-overall programme. Lancet 362(9386):759–766
Suissa S, Hutchinson T, Brophy JM et al (2006) ACE-inhibitor use and the long-term risk of renal failure in diabetes. Kidney Int 69:913–919
Kalra PA, Mamtora H, Holmes AM et al (1990) Renovascular disease and renal complications of angiotensin-converting enzyme inhibitor therapy. Q J Med 77(282):1013–1018
Devoy MAB, Tomson CR, Edmunds ME et al (1992) Deterioration in renal function associated with angiotensin converting enzyme inhibitor therapy is not always reversible. J Intern Med 232(6):493–498
Thomas MC (2000) Diuretics, ACE inhibitors and NSAIDs—the triple whammy. Med J Aust 172(4):184–185
Descombes E, Fellay G (2000) End-stage renal failure after irbesartan prescription in a diabetic patient with previously stable chronic renal insufficiency. Ren Fail 22(6):815–821
Vachharajani TJ, Dacie JE, Yaqoob MM et al (2005) Detection of occult renovascular disease in unexplained chronic kidney disease. Int Urol Nephrol 37(4):793–796
Levey AS, Bosch JP, Lewis JB et al (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group. Ann Intern Med 130(6):461–470
Onuigbo M, Onuigbo N (2007) Renal failure from RAAS blockade in CKD patients: a prospective 50-month analysis—A call for pragmatic caution to optimize cardiorenal protection with RAAS blockade. Am J Kidney Dis 49(4):A64 (abstract #159)
Onuigbo MAC, Onuigbo NTC (2006) Late-onset renal failure from RAAS blockade. Kidney Int 70:1378–1379 (Letter to editor)
Hansen HP, Rossing P, Tarnow L et al (1995) Increased glomerular filtration rate after withdrawal of long-term antihypertensive treatment in diabetic nephropathy. Kidney Int 47(6):1726–1731
Apperloo AJ, de Zeeuw D, de Jong PE (1997) A short-term antihypertensive treatment-induced fall in glomerular filtration rate predicts long-term stability of renal function. Ann Intern Med 51(3):793–797
Raine AE (1990) Angiotensin-converting enzyme inhibition and renovascular disease. Q J Med 77(282):997–999
Ballermann BJ, Onuigbo MAC (2000) Angiotensins. In: Handbook of Physiology, edited by Fray, JCS: Section 7, The Endocrine System, Vol III. Endocrine Regulation of water and electrolyte balance. New York, NY: Oxford University Press; pp 104–155
Tsalamandris C, Allen TJ, Gilbert RE et al (1994) Progressive decline in renal function in diabetic patients with and without albuminuria. Diabetes 43(5):649–655
Onuigbo MA (2003) Causes of renal failure in patients with type 2 diabetes mellitus. JAMA 290(14):1855 (Letter to the Editor)
Bakris GL, Weir MR (2000) Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: is this a cause for concern? Arch Intern Med 160(5):685–693
Acknowledgements
We acknowledge the resourcefulness and expertise of Vinay Nijhawan, MD, Interventional Radiologist, Midelfort Clinic, Eau Claire, Wisconsin in MRA diagnostics.
Author information
Authors and Affiliations
Corresponding author
Additional information
No external funding was involved in this study. Institutional review board (IRB) approval was obtained.
This work is dedicated to the memory of a pleasant unnamed 74-year-old white woman, with ESRD, who died suddenly at home watching television, probably from a malignant arrhythmia.
Rights and permissions
About this article
Cite this article
Onuigbo, M.A.C., Onuigbo, N.T.C. Late-onset renal failure from angiotensin blockade (LORFFAB) in 100 CKD patients. Int Urol Nephrol 40, 233–239 (2008). https://doi.org/10.1007/s11255-007-9299-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-007-9299-2