
Abstract
Dysfunctional expectations and interpersonal problems are associated with depression, so we measured expected emotions towards interaction partners and compared them with actual emotions. We hypothesized that, between persons, individuals with higher subclinical depression would display stronger, more stable, and less accurate negative expectations. Within persons, we hypothesized that momentary negative expectations would predict subsequent negative affect. Fifty-three students completed 6 days of Experience Sampling, consisting of one morning expectation-assessment (9 am), three assessments on actual interpersonal emotions (1 pm, 5 pm, 9 pm), and six random affect-assessments. We regressed expected emotions, experienced emotions, expectation fluctuations, and expectation violations on subclinical depression. Using mixed model analyses, we further examined whether negative expectations preceded negative affect, and whether expectation violations preceded adjustments of expectations. Higher subclinical depression predicted more negative expectations. Within persons, worse-than-expected interpersonal interactions preceded negative affect whereas better-than-expected interactions preceded reductions of negative expectations. Despite problems with skewed data, our approach appears well-suited to examine interpersonal expectations in vivo.
Similar content being viewed by others


Introduction
Negative views of the future are a central aspect of major depressive disorder (MDD). For example, the influential cognitive triad of depression acknowledges negative cognitions directed towards the future, the world, and the self as a key aspect of depressive disorders (Beck et al., 1974). Further, the hopelessness theory of depression (Abramson et al., 1989) posits that adverse childhood experiences can facilitate the development of negative inferential styles, which in turn lead to hopelessness and finally to depression when an individual is confronted with negative life events (for a review, see Liu et al., 2015). According to Abramson et al. (1989), the content domain of a person’s inferential styles functions as a vulnerability when a person is confronted with stressors in that same domain, meaning that a person who shows elevated sensitivity for interpersonal events might develop symptoms when confronted with social rejection (for a review of the various altered interpersonal processes in depression, see Hames et al., 2013). In accordance with the hopelessness theory, one of the core criteria of MDD is the presence of “depressed, sad, hopeless (…)” mood (American Psychiatric Association, 2013, p. 163).
Recently, negative cognitions about the future have received renewed attention in the “ViolEx” model (Rief & Joormann, 2019; Rief et al., 2015). As the name suggests (ViolEx is short for violation of expectations), the model focuses on a specific subtype of negative cognitions, namely expectations, which can be described as future-directed cognitions that refer to the likelihood of a specific event or experience to occur (Kube et al., 2020a). The model proposes that situation-specific negative expectations about future events are at the core of the formation and maintenance of mental disorders, such as depression (Rief & Joormann, 2019; Rief et al., 2015). As indicated by the term “situation-specific”, the work by Rief et al. focuses on expectations regarding specific real-world situations rather than generalized hopelessness or pessimism, which they nonetheless acknowledge as important underlying processes (Kube et al., 2020a). Empirical studies support the notion that situation-specific negative expectations about future events are predictive of depressive symptoms in cross-sectional and longitudinal observational designs (Kube et al., 2018a, 2018c).
At the core of the ViolEx model are so-called “expectation violations”, meaning the mismatch of expectations and actual experiences (Rief & Joormann, 2019). Specifically, the model ascribes importance to the way these expectation violations are processed (Kube et al., 2020a). Whereas healthy participants adaptively change a negative expectation in response to a disconfirmed expectation, the model suggests that people with depression (or other disorders) fail to update negative expectations about the future, contributing to the maintenance of symptoms. The ViolEx model complements established theories well, as indicated by findings that situation-specific dysfunctional expectations mediate the effect of “intermediate beliefs” (Beck, 2011, p. 189) on depressive symptoms (Kube et al., 2018a).
Situation-specific expectations have been studied in different contexts, such as expectations about one’s performance in a task (Kube et al., 2019b), the ability to regulate emotions (Kube et al., 2017), or the intensity and controllability of intrusions (Herzog et al., 2022). Expectations that received very limited empirical attention so far (D’Astolfo et al., 2020) are situation-specific expectations about interpersonal interactions. This paucity is surprising given that interpersonal expectations are an important aspect of the ViolEx model, as indicated by the fact that two of four subscales of the Depressive Expectations Scale capture expectations about social interactions (Kube et al., 2017). In fact, depression and interpersonal interactions are closely intertwined. In comparison with non-depressed controls, people with MDD show altered facial expression, eye contact, and nonverbal gestures (Hames et al., 2013). They tend to alternate between excessive reassurance seeking to achieve self-enhancement (Starr & Davila, 2008) and negative feedback seeking aiming at self-verification (Hames et al., 2013; Wakeling et al., 2020). Further, depressed individuals show social anhedonia (Atherton et al., 2015), increased sensitivity to social rejection (Gao et al., 2017), and increased negative affect in response to momentary social stressors (van Winkel et al., 2015). Given these interconnections between depression and interpersonal processes, the present paper aims at examining the ViolEx model’s predictions in the context of interpersonal interactions.
Applying the ViolEx model to interpersonal interactions is a difficult endeavor. First and foremost, assessments of expectations evidently need to be prospective, meaning that longitudinal designs of some sort are necessary to measure expectations regarding a situation before the situation occurs (e.g., longitudinal experimental designs; Kube et al., 2018b). Beyond this general caveat, interpersonal interactions are best understood in a person’s idiosyncratic context due to inter-individual differences concerning the number and quality of interactions (Wilson et al., 2015) as well as interaction partners who might trigger certain interpersonal behavior (Meehan et al., 2018). Given these challenges, the assessment of interpersonal expectations warrants a method with high ecological validity, such as the Experience Sampling Method (Myin-Germeys et al., 2009, 2018). ESM studies use diary-like self-reports to capture momentary feelings, symptoms, and other variables of interest repeatedly throughout the day in participants’ everyday lives. This method can be used to capture prospective expectations regarding anticipated meetings with real-world interaction partners (i.e., before the meeting takes place), while being unaffected by depressive recall biases (Ben-Zeev & Young, 2010; Urban et al., 2018). Further, ESM allows examining the stability of these expectations over time as well as their accuracy by comparing them with actual interpersonal experiences (i.e., expectation violations).
To the best of our knowledge, no study has examined situation-specific interpersonal expectations in a prospective ESM design as of yet, but the overarching idea is not new. In fact, several studies have used such designs to examine expectations regarding mood and pleasure in everyday life (Li et al., 2019; Thompson et al., 2017; Wu et al., 2017; Zetsche et al., 2019). In the present study, we draw on this “affective forecasting” research (Mathersul & Ruscio, 2019) inasmuch as we operationalized interpersonal expectations as expected negative emotions towards an interaction partner. This approach yields an index that is inter-individually comparable despite the idiosyncrasies of interpersonal interactions and that is well established in ESM research on interpersonal interactions (Liu et al., 2018).
Based on the ViolEx model, we have formulated several hypotheses. On a between-person level, we hypothesized that individuals with higher subclinical depressive symptoms would display (a) stronger, (b) more stable, and (c) less accurate negative expectations. The remaining hypotheses referred to the immediate effects of negative interpersonal expectations as well as experiences on current mood on a within-person level (e.g., does thinking about an upcoming unpleasant meeting result in feelings of sadness, anger, distress, etc. shortly after?). We hypothesized that (d) stronger momentary negative expectations (i.e., anticipated negative emotions) as well as (e) stronger negative experiences (i.e., actually experienced negative emotions) would predict an increase in subsequent negative affective states during the same day within persons. Also, we hypothesized that (f) violations of expectations (i.e., both better-than expected and worse-than-expected interpersonal interactions) would be associated with subsequent changes in negative affective states within persons. Specifically, we hypothesized that a worse-than-expected interaction would be associated with increased subsequent negative affect. Finally, we hypothesized that (g) positive expectation violations would predict reductions of negative expectations in subsequent interpersonal interactions with the same interaction partner, and (h) that the reduction of negative expectations would be lower in people endorsing higher subclinical depressive symptoms. The latter hypothesis was aimed at testing the assumption that negative expectations are “immune” to correcting positive experiences in people with elevated depressive symptoms (Rief & Joormann, 2019).
Methods
Recruitment
We recruited undergraduate psychology students who took part in the study for course credits. Participants were eligible if they were at least 18 years of age and reported no mental disorder. The ethics committee of the Faculty of Human Sciences at the University of Bern approved the study (ID #2016-05-00006).
Procedures
Assessments took place between August and November 2016. Initial, so-far unpublished, analyses of the dataset focused on motivational incongruence using a network approach (Lüdtke et al., in preparation). In the light of recent theoretical (Rief & Joormann, 2019) and empirical advances in the field (e.g., Zetsche et al., 2019), we decided to revisit the data. Figure 1 shows the study design.

Study flow
All participants provided written informed consent before the start of the study. The baseline assessment consisted of an array of online questionnaires as well as a face-to-face meeting, in which participants received a study smartphone and detailed instructions on how to use it. The ESM assessment phase began after the baseline assessment (days between baseline and ESM: M = 5.7, SD 5.4) and was scheduled to last 6 days. We disabled all functions of the study smartphones except for the ESM program ‘movisensXS’, version 0.8.4211 (movisens GmbH, Germany). There were 10 ESM assessments per day. Four assessments occurred at fixed times, namely at 9 a.m. (prospective assessment), as well as 1 p.m., 5 p.m., and 9 p.m. (retrospective assessments). Six additional assessments of momentary negative affect occurred at pseudo-random times between 9:30 a.m. and 9:30 p.m. with a minimum distance of 60 min in between.
Measures
Baseline measures
Participants completed an extensive baseline assessment of self-report questionnaires. For the sake of brevity, we will focus on measures that are relevant for the analyses presented here. We administered the German version (Nilges & Essau, 2015) of the Depression Anxiety Stress Scales (DASS-21). For psychometric properties of the English scales see Antony et al. (1998). On three subscales, the DASS-21 measures depression, anxiety and stress. Participants rated how much each statement applied to them over the past week. Response options ranged from 1 (“Did not apply to me at all”) to 4 (“Applied to me very much, or most of the time”). For the German version, internal consistencies of the subscales range from α = 0.78 for the stress subscale to α = 0.91 for the depression subscale. In our sample, similar values were achieved, with the highest value for the depression subscale (α = 0.87), which we used in the analyses, followed by the stress (α = 0.80) and the anxiety subscales (α = 0.79). The DASS-21 is designed to capture symptoms both in clinical and non-clinical samples (Antony et al., 1998), making it a suitable choice for our non-clinical student sample.
Prospective ESM assessment
At 9 a.m. each morning, participants completed the prospective ESM assessment. First, we asked whether an interpersonal interaction was scheduled/anticipated for the morning (9 a.m. to 1 p.m.), noon (1p.m. to 5 p.m.), or afternoon/evening (5 p.m. to 9 p.m.) of the same day. If the participant responded with “yes”, we asked them to report the gender of the person, their relationship with them (partner, colleague, fellow student, etc.), and who initiated the meeting. If they planned to interact with several persons during a specific timeframe, participants were instructed to choose the person that was most important to them. If there was no anticipated interaction, participants could skip the respective section of the prospective assessment. We used participants’ ratings of how they expected to feel towards their interaction partner (“How will you feel towards your interaction partner?”) to measure interpersonal expectations. Participants rated each of the following emotional states: sad, angry, ashamed, happy, proud, content, scared, contemptuous, and guilty. Ratings were provided on 7-point Likert-scales ranging from “not at all” to “very” (e.g., “not angry at all” to “very angry”). We calculated the scale “negative interpersonal expectations” as the mean score of the items “sad”, “angry”, “ashamed”, “scared”, and “guilty”.
Retrospective ESM assessments
Three retrospective ESM assessments were scheduled at 1 p.m., 5 p.m., and 9 p.m. Participants reported whether the expected interaction took place and whether it was terminated prematurely. If the interaction took place, participants rated how they actually felt during the interaction, using the same aforementioned items (i.e., “sad”, “angry”, “ashamed”, “scared”, and “guilty”), resulting in a score of the actual negativity of the interpersonal experience. If an interaction was cancelled, we asked participants to guess how they would have felt during the interaction but these ratings were not considered in the present study.
Expectation violations (combination of prospective and retrospective ESM assessments)
Expectation violations were operationalized as the difference between a retrospective (i.e., experience-based) and a prospective (i.e., expectation-based) rating of negative emotions for a specific interpersonal interaction (expectation violation interaction i = negative experience interaction i – negative expectation interaction i). Hence, a positive value indicates that the actually experienced negative emotions were stronger than anticipated, so the interaction was “worse than expected”. For certain analyses, we considered only better-than-expected expectation violations (see Table 4), which we recoded so that higher values represent stronger positive expectation violations.
Pseudo-random ESM assessments of affect
At pseudo-random times between 9:30 a.m. and 9:30 p.m., participants reported positive and negative emotional states using a short version of the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988) called PANAVA-KS (Schallberger, 2005). The 10-item scale was developed for ESM research specifically and it covers positive activation (four items), negative activation (four items), as well as valence (two items) on 7-point Likert scales ranging from a positive to a negative pole (e.g., from relaxed to distressed). For the present analyses, we computed momentary negative affect as the mean score of the following items: distress (relaxed to distressed), anger (peaceful to angry), sadness (sad to happy), worry (free from worry to worried), and dissatisfaction (satisfied to dissatisfied). Higher ratings either reflect less positive or more negative affect, but we will refer to “negative affect” throughout to simplify the terminology.
Internal consistency of ESM measures
The nested structure of ESM assessments clustered within participants requires a reliability measure which takes the dependency of assessments into account (Bonito et al., 2012; Nezlek, 2017), so we relied on a multilevel procedure proposed by Bolger and Laurenceau (2013, pp. 127–138). Using the VARCOMP command in SPSS version 27 (IBM SPSS Statistics, RRID:SCR_016479), we obtained the time*person variance as well as the error variance to assesses the reliability of within-subject change over time, indicating whether there is “adequate systematic time x person variance” in a dataset (Bolger & Laurenceau, 2013, p. 137). In addition to the multilevel reliability, we report the classical Cronbach’s α, using data from the first assessment per participant.
Multilevel reliability scores were .70 for the negative expectations scale, .69 for the negative experiences scale, and .79 for the negative affect scale. The cross-sectional Cronbach’s α values were α = .83 for the negative expectations scale, α = .65 for the negative experiences scale, and α = .73 for the negative affect scale.
Power considerations
The target sample size was initially set to n = 50 based on the recommendation that intensive longitudinal Experience Sampling studies require sample sizes of at least n = 50 at level two (i.e., participants in this case) to avoid biased estimates of second-level standard errors (Maas & Hox, 2005). Upon revisiting the dataset to conduct the analyses presented here, we did not perform additional a priori power calculations. However, we considered the existing dataset to be large enough to answer the questions at hand based on previous studies in the field, such as an observational study of situation-specific dysfunctional expectations in a student sample (Kube et al., 2018a), which found medium to large correlations between dysfunctional expectations and the Beck’s Depression Inventory II (contemporaneous: r = .63, 1-year lag: r = .46).
Data preparation
We provided the option to access ESM questionnaires manually so that participants could catch up on prompted assessments that were missed. For some participants, this resulted in multiple entries for the same assessment (e.g., two retrospective emotion ratings for the same interpersonal interaction). If there was more than one fully and timely completed rating, we retained the later rating as the participant likely corrected their initial response (this applied to 27 out of 3982 cases, corresponding to 0.7%).
The first hypothesis of the present study was that individuals with higher subclinical depressive symptoms show stronger negative expectations, less variability of negative expectations, and stronger expectation violations, averaged across the whole 6-day ESM period (i.e., one index per participant). We aggregated negative expectations and negative experiences by computing the person-mean of ratings across the 6-day assessment period, whereas the variability of negative interpersonal expectations was operationalized as the day-to-day person-SD across the 6 days. To obtain an aggregated value of expectation violations, we computed the difference between each interpersonal expectation and the corresponding interpersonal experience and computed the person-mean. This value indicates whether participants showed a general “bias” towards too optimistic vs. pessimistic expectations across interpersonal interactions.
Analyses
Between-person analyses of aggregated ESM data
The aggregated scores of negative expectations and subclinical depressive symptoms showed skew with a high proportion of participants that reported no or almost no depressive symptoms and negative expectations, respectively. Skew indices were 1.69 (SE = 0.33) for negative expectations and 1.57 (SE = 0.04) for subclinical depressive symptoms. To account for this skew (and to facilitate the interpretation of planned moderation analyses), we initially planned to conduct a median split to dichotomize the sample based on subclinical depressive symptoms. However, as median splits have received considerable criticism and may lead to loss of information (McClelland et al., 2015), we decided to conduct a conventional linear regression analyses with bias corrected and accelerated (BCa) bootstrapping (5000 samples) to obtain robust significance estimates. For descriptive purposes, we nonetheless present baseline characteristics for high versus low depressive symptoms based on the median split in Table 1.
Precursors of moment-to-moment fluctuations of negative affect
In addition to aforementioned between-person analyses, which make only limited use of the intensive longitudinal within-person ESM data, we conducted lagged regression mixed model analyses (LMM), which allow examining the moment-to-moment fluctuations of variables and their precursors within persons. LMM account for the clustering of occasions nested within participants, which is defining for ESM and other longitudinal research designs, while also flexibly handling missing data (Twisk, 2019, p. 150). All models included random intercepts but no random slopes. For moderation analyses, we included subclinical depressive symptoms as a predictor at the person-level and added the “predictor x subclinical depression” interaction.
LMM effects are comprised of two components, namely a within-person effect and a between-person effect. We were interested primarily in the within-person effect as it represents the moment-to-moment fluctuations within persons. Therefore, we person-mean centered predictor variables by computing the within-person mean of the predictor variable (e.g., negative expectations) and subtracting each value from it. Expectation violations were not centered as they were calculated as within-person difference scores, which do not require centering. If there was no within-person effect of moment-to-moment fluctuations, we followed up on the analyses with so-called “hybrid models” (Twisk, 2019, p. 139), which include both the person-mean centered predictor as well as the person-mean itself, allowing to disentangle within- from between-person effects. We conducted separate LMMs to explore the effect of negative interpersonal expectations, negative experiences, and expectation violations on subsequent negative affect.
Precursors of expectation adjustments
The ViolEx model predicts that individuals with depression retain dysfunctional negative expectations despite experiencing disconfirming positive expectation violations. To test this assumption, we identified participants who interacted with the same interaction partner repeatedly during the ESM period (using nicknames that participants provided for their interaction partners) and examined the effect of positive expectation violations on subsequent changes of negative expectations (expectation adjustment person i, t0 = negative expectation person i, t0 – negative expectation person i, t-1). Subsequently, we examined whether the effect was contingent on subclinical depressive symptoms using an interaction term.
Results
Participant characteristics and adherence
A total of n = 55 participants completed the baseline assessment. We had to exclude two participants because they completed less than 33% of the scheduled ESM assessments, so the final sample consisted of n = 53 participants. Baseline characteristics are presented in Table 1. The proportion of female participants was higher in the subgroup endorsing subclinical depressive symptoms below the median.
The majority of included participants (n = 51; 96%) used the study smartphone for 6 days as intended. One participant turned off the smartphone prematurely after 4 days, and another participant kept it on for 7 days, resulting in a grand mean of 5.98 days of usage (SD = 0.30). Assessments were flagged as missing if they were dismissed, ignored, discontinued, or completed more than 30 min late. The proportion of missing or late assessments was 20.4% for the fixed prospective/retrospective assessments and 17.1% for pseudo-random assessments of affect, resulting in 18.3% missing assessments overall.
Between-person associations of subclinical depressive symptoms and negative expectations
Results of simple linear regression analyses with BCa bootstrapping are presented Table 2. Higher subclinical depressive symptoms were associated with stronger expected negative emotions across interpersonal interactions (i.e., negative expectations) during the 6-day ESM period, as indicated by a conventional significance test as well as robust BCa bootstrap significance testing. In contrast, there was no effect of subclinical depressive symptoms on actually experienced negative emotions during interpersonal interactions (i.e., negative experiences). While the conventional p-value indicated no effect of subclinical depressive symptoms on the day-to-day variability of negative expectations, robust bootstrapping indicated significant effects. Irrespective of this inconsistency, either result contradicts our hypothesis that stronger subclinical depressive symptoms are associated with more stable (negative) expectations. Bootstrapping even suggests that the variability of negative expectations could be larger when subclinical depressive symptoms are higher. Lastly, we found no effect of subclinical depressive symptoms on averaged expectation violations.
Given that the proportion of female participants differed between people above versus below the median of subclinical depressive symptoms (see Table 1), we repeated analyses presented in Table 2 with gender as a covariate. Adding gender as a covariate did not change the direction or significance of effects.
Negative interpersonal expectations as within-person precursors of negative affect
Within-person fluctuations of negative expectations did not predict negative affect during subsequent hours of the day (see Table 3), which was supported by a hybrid model, indicating that person-mean values of negative expectations were associated with momentary negative affect (b = 1.507, SE = 0.371, t(df) = 4.064 (56.29), p < .001) whereas momentary fluctuations of negative expectations were not (b = 0.044, SE = 0.077, t(df) = 0.570 (1595.72), p = .569). This pattern of results suggests that it is not the ebb and flow of expectations which predicts fluctuations of negative affect, but instead a person’s “general” negativity of expectations.
Negative interpersonal experiences as within-person precursors of negative affect
The effects of negative experiences on negative affect were similar to those of negative expectations (see Table 3). Whereas moment-to-moment fluctuations of negative experiences did not predict subsequent negative affect in the hybrid model (b = 0.190, SE = 0.119, t(df) = 1.599 (330.55), p = .111), the tendency to report stronger negative interpersonal experiences on average did predict negative affect (b = 1.379, SE = 0.325, t(df) = 4.241 (51.12), p < .001).
Expectation violations as within-person precursors of negative affect
The worse an interaction was when compared to a person’s expectations, the more negative affect was reported in subsequent hours of the day (Table 3). Accordingly, a better-than-expected interaction resulted in less negative affect. We examined whether this effect differed depending on the level of subclinical depressive symptoms but there was no interaction (see Table 3, model 4).
In sum, the results presented in Table 3 indicate that it is not the negativity of a momentary interaction, but rather the unexpected negativity, which predicts subsequent negative affect, irrespective of the intensity of subclinical depressive symptoms.
Day-to-day adjustments of interpersonal expectations within persons
If a person’s interpersonal expectation does not match the actual experience, this should lead to an adaptive adjustment of expectations in a subsequent interaction with the same interaction partner. Adaptation of expectations represents a central aspect of the ViolEx model, in that individuals with depression are hypothesized to show an insufficient adjustment of negative expectations in light of correcting experiences, particularly of positive expectation violations (Kube et al., 2019b). Here, we examined whether better-than-expected expectation violations would predict the extent to which participants would adjust their negative expectation downwards when they interacted with the same person at least twice.
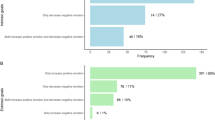
There were 154 interpersonal interactions with the same interaction partner provided by n = 45 participants (the median number of days between two interactions with the same partner was one). Unfortunately (both for the participants and our analysis), only few interpersonal interactions were better-than-expected interactions, namely 24 interactions reported by n = 17 participants. The majority of same-partner expectations were accurate (125 accurate assessments; 88%). Despite this constraint, we conducted the analysis as planned.
As can be seen in Table 4, there was an association between the strength of the positive expectation violation and the amount of downward adjustment of negative expectations from one interaction to the next (model 1). This effect was not moderated by the severity of subclinical depressive symptoms, meaning that the adjustment of negative expectations was not significantly reduced for people with higher depressive symptoms. Given that there was a trend in the hypothesized direction, we conducted an exploratory simple slope analysis to descriptively compare the effect of positive expectation violations on subsequent downward adjustments of negative expectations between individuals below versus above the median of subclinical depressive symptoms. This analysis must be interpreted with caution, but simple slopes suggest a descriptively larger reduction of negative expectations in people with low depressive symptoms (n = 16 cases; blow = − 1.300, SE = 0.185, t(df) = 7.025 (19.19), p < .001) compared to people with high depressive symptoms (n = 8 cases; bhigh = − 0.657, SE = 0.224, t(df) = 2.937 (14.65), p = .010).
Discussion
In the present study, we tested several hypotheses derived from the ViolEx model (Rief & Joormann, 2019) by using intensive longitudinal real-world data on interpersonal interactions in an undergraduate sample. On a between-person level, we examined whether individuals with comparably higher subclinical depressive symptoms would show stronger and more stable negative expectations as well as stronger average expectation violations. On a within-subject level, we examined whether momentary negative expectations, negative experiences (i.e., actually experienced negative emotions during interpersonal interactions), and expectation violations would predict increased subsequent negative affect. Lastly, we examined whether positive expectation violations would predict within-person adjustments of negative expectations and whether people with elevated subclinical depressive symptoms would adjust their negative expectations to a lesser degree when experiencing positive expectation violations. Linear regression analyses indicated that higher subclinical depressive symptoms were associated with more negative expectations regarding interpersonal interactions (averaged across the 6-day ESM period), while there was no effect on actual negative experiences (i.e., negative emotions experienced during interpersonal interactions). This finding tentatively suggests that negative expectations could be more relevant to subclinical depressive symptoms than actual negative experiences. In linear mixed model analyses of within-person associations, we found no effects of momentary negative expectations on subsequent negative affect. Instead, unexpected expectation-violating negative experiences predicted subsequent increases of negative affect throughout the day. Lastly, we found that, across the whole sample, better-than-expected interpersonal interactions resulted in a reduction of negative expectations, indicating an adaptive adjustment of expectations based on recent interpersonal experiences. Contrary to our hypothesis, we found that the tendency to adjust negative expectations following unexpectedly positive interpersonal interactions was not dependent on the level of subclinical depressive symptoms. However, a statistical trend of higher subclinical depressive symptoms being associated with a reduced adjustment of expectations tentatively suggests that it might be worthwhile to examine this effect further in future studies.
The main results of our study are in line with the predictions of the ViolEx model (Kube et al., 2020b), but it remains unclear whether a generalization from our subclinical sample to clinical populations is warranted. Despite this caveat, our findings can be discussed in light of the existing literature. For example, individuals with clinically relevant depression report reduced hope, higher expectations of experiencing negative events as well as lower expectations for positive events (Thimm et al., 2013), and they overestimate the likelihood of negative mood in an ESM setting (Zetsche et al., 2019). Our findings add to this body of evidence in that we found that individuals with elevated subclinical depressive symptoms show stronger negative expectations in the interpersonal domain.
The study by Zetsche et al. (2019), and also other ESM studies on “mood forecasting” (e.g., Thompson et al., 2017) show that it is important to consider not only expectations regarding negative affect but also positive affect. In fact, a lack of positive expectations specifically, rather than the presence of negative expectations, appears to be associated with depression, for example in an observational longitudinal study of adolescents (Horwitz et al., 2017), in a meta-analysis of anticipatory pleasure for future experiences in depression (Hallford & Sharma, 2019), and in neuroscientific studies on blunted reward sensitivity in depression (Alloy et al., 2016). In hindsight, one might argue that we should have focused on expectations regarding a lack of positive emotions during interpersonal interactions but we decided to adhere to the pre-defined analysis plan to ensure methodological rigor. From a practical point of view, adding additional analyses using an alternative operationalization of negative expectations would have further inflated the number of analyses, increasing the risk of alpha error inflation. In future studies on interpersonal expectations, the differentiation into increased negative versus reduced positive expectations could be conceptualized in the framework of approach- and avoidance goals (Grosse Holtforth, et al., 2007). In this framework, negative expectations either represent a tendency to avoid aversive interpersonal experiences (i.e., avoidance goals, such as being criticized) or a failure to achieve appetitive goals (i.e., an approach goal, such as being admired).
The rigidity of negative expectations despite disconfirming positive expectation violations (explained through processes such as cognitive immunization; Kube et al., 2019b) is arguably one of the most important aspects of the ViolEx model, not least because it could be translated into targeted interventions (Kube et al., 2019a). Unfortunately, our data did not allow examining this aspect of the model in depth due to the small proportion of individuals who interacted with the same partner repeatedly and reported positive expectation violations. It seems to be a worthwhile endeavor to pursue the study of interpersonal expectation-adjustments in depression further, for example complemented by processes that are well-established in neuroscience, such as a measure of confidence in one’s predictions (for an integrative review, see Kube et al., 2020b). Confidence ratings could be of particular interest given that depression is linked to reduced specificity for positive future thinking (similar to autobiographic memories), whereas the specificity of negative and neutral thoughts about the future is not reduced (Gamble et al., 2019).
Limitations and future directions
Our results must be interpreted in light of several limitations. Beyond general peculiarities of healthy student samples (Henrich et al., 2010), recruiting non-clinical participants was problematic in our case because it led to extremely sparse ratings of depressive symptoms, negative expectations, and negative interpersonal experiences. To illustrate, the mean ratings of negative expectations were M = 1.095 for the participants endorsing subclinical depressive symptoms below the median, and M = 1.376 for participants above the median. Given that the scale ranged from 1 to 7, ratings showed floor effects across the whole sample. Although we termed the scale “negative expectations”, our participants rather reported very positive expectations. A concerning by-product of consistently positive ratings was that there was very little variation in ratings of negative expectations and negative experiences. Given that standard errors are computed using the sample standard deviations, this might have led to inflated test-statistics, underestimated p-values, and overestimated effect sizes. In sum, despite being in line with model predictions, the generalization of our results to populations with more severe depressive symptoms is problematic not only due to the characteristics of our sample (very young, healthy, educated, and predominantly female) but also due to limited variation in the data. Lastly, it is important to note that our analyses were not pre-registered and, although theory-driven, to some extend exploratory. Our results require independent replication in a more heterogeneous sample with higher levels of depressive symptoms, preferably people with MDD diagnoses. Despite the aforementioned limitations, the newly developed “prospective ESM” methodology has proven feasible and well-suited to answer the questions at hand. Unlike retrospective assessment methods, our ESM-based measurements were not liable to memory biases (Ben-Zeev & Young, 2010), and we were able to achieve high overall adherence rates with only two participants showing insufficient compliance, while more than 80% of participants provided valid responses in the final sample, which is above the average response rates for ESM studies on mobile devices (approximately 70%; van Berkel et al., 2018).
If corroborated in a clinical population, our findings have the potential to add to advances in the development of cognitive-behavioral interventions, for example by maximizing the violation of dysfunctional expectations (Rief & Joormann, 2019) or by increasing the salience of an expectation-disconfirming experience (Craske et al., 2014). Such interventions might be most effective in vivo using so-called ecological momentary interventions (Colombo et al., 2019) given that findings on exposure therapy for anxiety disorders show a renewal of conditional fear if surrounding contexts are changed (Bouton, 1993). Another potential treatment approach would be to target the rigidity of negative interpersonal expectations by providing information that reduces the impact of cognitive immunization (Kube et al., 2019a), although it must be noted that the effect of cognitive immunization is subject to debate, as a recent study failed to demonstrate an effect of cognitive immunization on expectation updating in a non-clinical sample (Kube & Glombiewski, 2022). Interestingly, negative mood, a central aspect of the present study, could be a potential moderator of the effect (Kube & Glombiewski, 2020).
In sum, the present study was a promising first step towards understanding the moment-to-moment effects of negative interpersonal expectations and possible associations with affect and subclinical depressive symptoms. The prospective ESM approach appears feasible and well-suited to examine interpersonal processes and associated expectations in vivo. The preliminary findings are in line with sound theoretical underpinnings, and they offer pathways to add to existing interventions.
Data availability
The data that support the findings of this study are available from the corresponding author, TL, upon reasonable request.
References
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory-based subtype of depression. Psychological Review, 96(2), 358–372. https://doi.org/10.1037/0033-295x.96.2.358
Alloy, L. B., Olino, T., Freed, R. D., & Nusslock, R. (2016). Role of reward sensitivity and processing in major depressive and bipolar spectrum disorders. Behavior Therapy, 47(5), 600–621. https://doi.org/10.1016/j.beth.2016.02.014
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.). American Psychiatric Publishing Inc.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. https://doi.org/10.1037/1040-3590.10.2.176
Atherton, B. D., Nevels, R. M., & Moore, M. T. (2015). Predicting symptoms of depression from social anhedonia and emotion regulation. The Journal of Nervous and Mental Disease, 203(3), 170–174. https://doi.org/10.1097/NMD.0000000000000262
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond (2nd ed.). Guilford Press.
Beck, A. T., Weissman, A., Lester, D., & Trexler, L. (1974). The measurement of pessimism: The hopelessness scale. Journal of Consulting and Clinical Psychology, 42(6), 861–865. https://doi.org/10.1037/h0037562
Ben-Zeev, D., & Young, M. A. (2010). Accuracy of hospitalized depressed patients’ and healthy controls’ retrospective symptom reports: An experience sampling study. The Journal of Nervous and Mental Disease, 198(4), 280–285. https://doi.org/10.1097/NMD.0b013e3181d6141f
Bolger, N., & Laurenceau, J.-P. (2013). Intensive longitudinal methods: An introduction to diary and experience sampling research. Guilford Press.
Bonito, J. A., Ruppel, E. K., & Keyton, J. (2012). Reliability estimates for multilevel designs in group research. Small Group Research, 43(4), 443–467. https://doi.org/10.1177/1046496412437614
Bouton, M. E. (1993). Context, time, and memory retrieval in the interference paradigms of pavlovian learning. Psychological Bulletin, 114(1), 80–99. https://doi.org/10.1037/0033-2909.114.1.80
Colombo, D., Fernandez-Alvarez, J., Patane, A., Semonella, M., Kwiatkowska, M., Garcia-Palacios, A., Cipresso, P., Riva, G., & Botella, C. (2019). Current state and future directions of technology-based ecological momentary assessment and intervention for major depressive disorder: A systematic review. Journal of Clinical Medicine, 8(4), 465. https://doi.org/10.3390/jcm8040465
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. https://doi.org/10.1016/j.brat.2014.04.006
D’Astolfo, L., Kirchner, L., & Rief, W. (2020). No1LikesU!—A pilot study on an ecologically valid and highly standardised experimental paradigm to investigate social rejection expectations and their modification. Clinical Psychology in Europe, 2(2), 1–21. https://doi.org/10.32872/cpe.v2i2.2997
Gamble, B., Moreau, D., Tippett, L. J., & Addis, D. R. (2019). Specificity of future thinking in depression: A meta-analysis. Perspectives on Psychological Science, 14(5), 816–834. https://doi.org/10.1177/1745691619851784
Gao, S., Assink, M., Cipriani, A., & Lin, K. (2017). Associations between rejection sensitivity and mental health outcomes: A meta-analytic review. Clinical Psychology Review, 57, 59–74. https://doi.org/10.1016/j.cpr.2017.08.007
Grosse Holtforth, M., Pincus, A. L., Grawe, K., Mauler, B., & Castonguay, L. G. (2007). When what you want is not what you get: Motivational correlates of interpersonal problems in clinical and nonclinical samples. Journal of Social and Clinical Psychology, 26(10), 1095–1119. https://doi.org/10.1521/jscp.2007.26.10.1095
Hallford, D. J., & Sharma, M. K. (2019). Anticipatory pleasure for future experiences in schizophrenia spectrum disorders and major depression: A systematic review and meta-analysis. British Journal of Clinical Psychology, 58(4), 357–383. https://doi.org/10.1111/bjc.12218
Hames, J. L., Hagan, C. R., & Joiner, T. E. (2013). Interpersonal processes in depression. Annual Review of Clinical Psychology, 9(1), 355–377. https://doi.org/10.1146/annurev-clinpsy-050212-185553
Henrich, J., Heine, S. J., & Norenzayan, A. (2010). The weirdest people in the world? Behavioral and Brain Sciences, 33(2–3), 61–83. https://doi.org/10.1017/S0140525X0999152X
Herzog, P., Barth, C., Rief, W., Brakemeier, E.-L., & Kube, T. (2022). How expectations shape the formation of intrusive memories: An experimental study using the trauma film paradigm. Cognitive Therapy and Research, 46(4), 809–826. https://doi.org/10.1007/s10608-022-10290-4
Horwitz, A. G., Berona, J., Czyz, E. K., Yeguez, C. E., & King, C. A. (2017). Positive and negative expectations of hopelessness as longitudinal predictors of depression, suicidal ideation, and suicidal behavior in high-risk adolescents. Suicide and Life-Threatening Behavior, 47(2), 168–176. https://doi.org/10.1111/sltb.12273
Kube, T., & Glombiewski, J. A. (2020). How depressive symptoms hinder positive information processing: An experimental study on the interplay of cognitive immunisation and negative mood in the context of expectation adjustment. Cognitive Therapy and Research, 45(3), 517–528. https://doi.org/10.1007/s10608-020-10191-4
Kube, T., & Glombiewski, J. A. (2022). No evidence for the involvement of cognitive immunisation in updating beliefs about the self in three non-clinical samples. Cognitive Therapy and Research, 46(1), 43–61. https://doi.org/10.1007/s10608-021-10256-y
Kube, T., D’Astolfo, L., Glombiewski, J. A., Doering, B. K., & Rief, W. (2017). Focusing on situation-specific expectations in major depression as basis for behavioural experiments—Development of the depressive expectations scale. Psychology and Psychotherapy: Theory, Research and Practice, 90(3), 336–352. https://doi.org/10.1111/papt.12114
Kube, T., Rief, W., Gollwitzer, M., Gartner, T., & Glombiewski, J. A. (2019b). Why dysfunctional expectations in depression persist—Results from two experimental studies investigating cognitive immunization. Psychological Medicine, 49(9), 1532–1544. https://doi.org/10.1017/S0033291718002106
Kube, T., Rief, W., Gollwitzer, M., & Glombiewski, J. A. (2018b). Introducing an experimental paradigm to investigate expectation change (EXPEC). Journal of Behavior Therapy and Experimental Psychiatry, 59, 92–99. https://doi.org/10.1016/j.jbtep.2017.12.002
Kube, T., Rozenkrantz, L., Rief, W., & Barsky, A. (2020a). Understanding persistent physical symptoms: Conceptual integration of psychological expectation models and predictive processing accounts. Clinical Psychology Review, 76, 101829. https://doi.org/10.1016/j.cpr.2020.101829
Kube, T., Glombiewski, J. A., Gall, J., Touissant, L., Gärtner, T., & Rief, W. (2019a). How to modify persisting negative expectations in major depression? An experimental study comparing three strategies to inhibit cognitive immunization against novel positive experiences. Journal of Affective Disorders, 250, 231–240. https://doi.org/10.1016/j.jad.2019.03.027
Kube, T., Glombiewski, J. A., & Rief, W. (2018a). Situational expectations mediate the effect of global beliefs on depressive symptoms: A 1-year prospective study using a student sample. Current Opinion in Psychiatry, 31(5), 409–416. https://doi.org/10.1097/YCO.0000000000000443
Kube, T., Schwarting, R., Rozenkrantz, L., Glombiewski, J. A., & Rief, W. (2020b). Distorted cognitive processes in major depression: A predictive processing perspective. Biological Psychiatry, 87(5), 388–398. https://doi.org/10.1016/j.biopsych.2019.07.017
Kube, T., Siebers, V. H. A., Herzog, P., Glombiewski, J. A., Doering, B. K., & Rief, W. (2018c). Integrating situation-specific dysfunctional expectations and dispositional optimism into the cognitive model of depression—A path-analytic approach. Journal of Affective Disorders, 229, 199–205. https://doi.org/10.1016/j.jad.2017.12.082
Li, X., Zhang, Y. T., Huang, Z. J., Chen, X. L., Yuan, F. H., & Sun, X. J. (2019). Diminished anticipatory and consummatory pleasure in dysphoria: Evidence from an experience sampling study. Frontiers in Psychology, 10, 2124. https://doi.org/10.3389/fpsyg.2019.02124
Liu, H., Xie, Q. W., & Lou, V. W. Q. (2018). Everyday social interactions and intra-individual variability in affect: A systematic review and meta-analysis of ecological momentary assessment studies. Motivation and Emotion, 43(2), 339–353. https://doi.org/10.1007/s11031-018-9735-x
Liu, R. T., Kleiman, E. M., Nestor, B. A., & Cheek, S. M. (2015). The hopelessness theory of depression: A quarter century in review. Clinical Psychology: Science and Practice, 22(4), 345–365. https://doi.org/10.1111/cpsp.12125
Lüdtke, T., Steiner, F., Berger, T., & Westermann, S. (in preparation). Assessment and representation of conflict between motives in daily life: Introducing motive networks.
Maas, C. J. M., & Hox, J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology: European Journal of Research Methods for the Behavioral and Social Sciences, 1(3), 86–92. https://doi.org/10.1027/1614-2241.1.3.86
Mathersul, D. C., & Ruscio, A. M. (2019). Forecasting the future, remembering the past: Misrepresentations of daily emotional experience in generalized anxiety disorder and major depressive disorder. Cognitive Therapy and Research, 44(1), 73–88. https://doi.org/10.1007/s10608-019-10048-5
McClelland, G. H., Lynch, J. G., Irwin, J. R., Spiller, S. A., & Fitzsimons, G. J. (2015). Median splits, type II errors, and false–positive consumer psychology: Don’t fight the power. Journal of Consumer Psychology, 25(4), 679–689. https://doi.org/10.1016/j.jcps.2015.05.006
Meehan, K. B., Cain, N. M., Roche, M. J., Clarkin, J. F., & De Panfilis, C. (2018). Rejection sensitivity and interpersonal behavior in daily life. Personality and Individual Differences, 126, 109–115. https://doi.org/10.1016/j.paid.2018.01.029
Myin-Germeys, I., Oorschot, M., Collip, D., Lataster, J., Delespaul, P., & van Os, J. (2009). Experience sampling research in psychopathology: Opening the black box of daily life. Psychological Medicine, 39(9), 1533–1547. https://doi.org/10.1017/S0033291708004947
Myin-Germeys, I., Kasanova, Z., Vaessen, T., Vachon, H., Kirtley, O., Viechtbauer, W., & Reininghaus, U. (2018). Experience sampling methodology in mental health research: New insights and technical developments. World Psychiatry, 17(2), 123–132. https://doi.org/10.1002/wps.20513
Nezlek, J. B. (2017). A practical guide to understanding reliability in studies of within-person variability. Journal of Research in Personality, 69, 149–155. https://doi.org/10.1016/j.jrp.2016.06.020
Nilges, P., & Essau, C. (2015). Die depressions-angst-stress-skalen [the depression-anxiety-stress-scales]. Der Schmerz, 29(6), 649–657. https://doi.org/10.1007/s00482-015-0019-z
Rief, W., & Joormann, J. (2019). Revisiting the cognitive model of depression: The role of expectations. Clinical Psychology in Europe, 1(1), 1–19. https://doi.org/10.32872/cpe.v1i1.32605
Rief, W., Glombiewski, J. A., Gollwitzer, M., Schubo, A., Schwarting, R., & Thorwart, A. (2015). Expectancies as core features of mental disorders. Current Opinion in Psychiatry, 28(5), 378–385. https://doi.org/10.1097/YCO.0000000000000184
Schallberger, U. (2005). Kurzskalen zur erfassung der positiven aktivierung, negativen aktivierung und valenz in experience sampling studien (panava-ks) [short scales to assess positive activation, negative activation, and valence in experience sampling studies (panava-ks)]. Retrieved February 3, 2022, from Forschungsberichte aus dem Projekt:“Qualität des Erlebens in Arbeit und Freizeit, 6. Retrieved from https://www.psychologie.uzh.ch/institut/angehoerige/emeriti/schallberger/schallberger-pub/PANAVA_05.pdf
Starr, L. R., & Davila, J. (2008). Excessive reassurance seeking, depression, and interpersonal rejection: A meta-analytic review. Journal of Abnormal Psychology, 117(4), 762–775. https://doi.org/10.1037/a0013866
Thimm, J. C., Holte, A., Brennen, T., & Wang, C. E. (2013). Hope and expectancies for future events in depression. Frontiers in Psychology, 4, 470. https://doi.org/10.3389/fpsyg.2013.00470
Thompson, R. J., Spectre, A., Insel, P. S., Mennin, D., Gotlib, I. H., & Gruber, J. (2017). Positive and negative affective forecasting in remitted individuals with bipolar i disorder, and major depressive disorder, and healthy controls. Cognitive Therapy and Research, 41(5), 673–685. https://doi.org/10.1007/s10608-017-9840-2
Twisk, J. W. R. (2019). Applied mixed model analysis (2nd ed.). Cambridge University Press.
Urban, E. J., Charles, S. T., Levine, L. J., & Almeida, D. M. (2018). Depression history and memory bias for specific daily emotions. PLoS ONE, 13(9), e0203574. https://doi.org/10.1371/journal.pone.0203574
van Berkel, N., Ferreira, D., & Kostakos, V. (2018). The experience sampling method on mobile devices. ACM Computing Surveys, 50(6), 1–40. https://doi.org/10.1145/3123988
van Winkel, M., Nicolson, N. A., Wichers, M., Viechtbauer, W., Myin-Germeys, I., & Peeters, F. (2015). Daily life stress reactivity in remitted versus non-remitted depressed individuals. European Psychiatry, 30(4), 441–447. https://doi.org/10.1016/j.eurpsy.2015.02.011
Wakeling, S., Stukas, A. A., Wright, B. J., & Evans, L. (2020). Negative feedback seeking and excessive reassurance seeking behavior and depression: A meta-analytic review. Journal of Social and Clinical Psychology, 39(9), 788–823. https://doi.org/10.1521/jscp.2020.39.9.788
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. https://doi.org/10.1037//0022-3514.54.6.1063
Wilson, R. E., Harris, K., & Vazire, S. (2015). Personality and friendship satisfaction in daily life: Do everyday social interactions account for individual differences in friendship satisfaction? European Journal of Personality, 29(2), 173–186. https://doi.org/10.1002/per.1996
Wu, H., Mata, J., Furman, D. J., Whitmer, A. J., Gotlib, I. H., & Thompson, R. J. (2017). Anticipatory and consummatory pleasure and displeasure in major depressive disorder: An experience sampling study. Journal of Abnormal Psychology, 126(2), 149–159. https://doi.org/10.1037/abn0000244
Zetsche, U., Burkner, P. C., & Renneberg, B. (2019). Future expectations in clinical depression: Biased or realistic? Journal of Abnormal Psychology, 128(7), 678–688. https://doi.org/10.1037/abn0000452
Acknowledgements
We thank Kristina Hedelt and Fabian Steiner for their valuable contribution to data collection and –curation.
Funding
Open Access funding enabled and organized by Projekt DEAL. While conducting the study, SW received funding from the UniBE initiator grant. During analysis and write-up, SW and TL were funded by their institution. The study did not receive further funding. The funding had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
SW was responsible for funding acquisition, investigation, project administration, resources, the planning of the study, the conceptualization, the methodology, and writing—review and editing. TL performed the data curation, formal analysis, writing of the draft and visualization of results. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. The ethics committee of the Faculty of Human Sciences at the University of Bern approved the study (#2016-05-00006).
Informed consent
All participants provided written informed consent prior to participation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lüdtke, T., Westermann, S. Negative expectations regarding interpersonal interactions in daily life are associated with subclinical depressive symptoms in a student sample: A prospective experience sampling study. Motiv Emot 47, 125–136 (2023). https://doi.org/10.1007/s11031-022-09985-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11031-022-09985-8