
Abstract
Background and Purpose
Autosomal dominant hyper-IgE syndrome (AD-HIES) is a rare primary immunodeficiency disorder . It has been recognized as a multisystem disorder and is characterized by both immunologic and non-immunologic manifestations. Possible bone involvement in autosomal dominant HIES include fractures, scoliosis, cystic bone changes, and osteopenia. We sought to evaluate the changes in bone density in adolescents and young adults with AD-HIES, mostly with proven STAT3 mutation, followed in our institute.
Methods
We studied eight patients with AD-HIES who attended our immunology clinic. All patients underwent at least one bone mass dual-energy x-ray absorptiometry assessment (dual-energy x-ray absorptiometry scan).These findings were evaluated.
Results
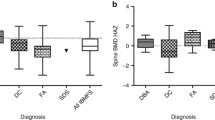
The age of the patients at the time of their first bone density scan ranged between 10 and 24 years (mean 16.1 ± 4.0 years); the duration of follow-up was 4–11 years (mean 5.8 ± 3.5 years). Four patients had a history of fractures. Mean Z score in these patients was −1.8 ± 0.7. For three patients, Z score was below −1. The other four patients had no history of fractures. Mean Z score in these patients was −0.9 ± 0.5. Only one patient in this group had a Z score below −1. Bone density was below average in all patients; mean spinal Z score was −1.6 ± 0.4. Four patients were followed through the second decade, and all showed progressive deterioration in bone density. Three were treated with alendronate sodium, with improvement in the bone scan results.
Conclusions
Bone density decreases considerably over time in adolescents and young adults suffering from AD- HIES. Treatment with alendronate sodium may be effective in alleviating osteopenia.

Similar content being viewed by others


References
Davis SD, Schaller J, Wedgwood RJ. Job’s Syndrome. Recurrent, “cold”, staphylococcal abscesses. Lancet. 1966;1:1013–5.
Buckley R, Wray B, Belmaker E. Extreme hyperimmunoglobulinemia E and undue susceptibility to infection. Pediatrics. 1972;49:59–70.
Grimbacher B, Holland SM, Gallin JI, Greenberg F, Hill SC, Malech HL, et al. Hyper-IgE syndrome with recurrent infections – an autosomal dominant multisystem disorder. N Engl J Med. 1999;340:692–702.
Leung DY, Geha RS. Clinical and immunologic aspects of the hyperimmunoglobulin E syndrome. Hematol Oncol Clin North Am. 1988;2:81–100.
Blum R, Geller G, Fish LA. Recurrent severe staphylococcal infections, eczematoid rash: extreme elevations of IgE, eosinophilia and different chemotactic responses in two generations. J Pediatr. 1977;90:607–9.
Holland SM, DeLeo FR, Elloumi HZ, Hsu AP, Uzel G, Brodsky N, et al. STAT3 mutations in the hyper-IgE syndrome. N Engl J Med. 2007;357:1608–19.
Minegishi Y, Saito M, Tsuchiya S, Tsuge I, Takada H, Hara T, et al. Dominant-negative mutations in the DNA-binding domain of STAT3 cause hyper-IgE syndrome. Nature. 2007;448:1058–62.
Freeman AF, Holland SM. The hyper-IgE syndromes. Immunol Allergy Clin North Am. 2008;28:277–91.
Milner JD, Brenchley JM, Laurence A, Freeman AF, Hill BJ, Elias KM, et al. Impaired T(H)17 cell differentiation in subjects with autosomal dominant hyper-IgE syndrome. Nature. 2008;452:773–6.
Borgess WG, Hensley T, Carey JC, Petrak BA, Hill HR. The face of Job. J Pediatr. 1998;133:303–5.
Osteoporosis prevention, diagnosis and therapy. NIH consensus statement. [No authors listed] 2000;17:1–45.
Uziel Y, Zifman E, Hashkes PJ. Osteoporosis in children: pediatric and pediatric rheumatology perspective: a review. Pediatr Rheumatol Online J. 2009;7:16.
Gunes AM, Can E, Saglam H, Ilçöl YO, Baytan B. Assessment of bone mineral density and risk factors in children completing treatment for acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2010;32:e102–7.
Samson F, Cagnard B, Leray E, Guggenbuhl P, Bridoux-Henno L, Dabadie A. Longitudinal study of bone mineral density in children after a diagnosis of Crohn’s disease. Gastroenterol Clin Biol. 2010;334:554–61.
Gordon CM, Bachrach LK, Carpenter TO, Crabtree N, El-Hajj Fuleihan G, Kutilek S, et al. Dual energy x-ray absorptiometry interpretation and reporting in children and adolescents: the 2007 ISCD pediatric official positions. J Clin Densitom. 2008;11:43–58.
Schimke LF, Sawalle-Belohradsky J, Roesler J, Wollenberg A, Rack A, Borte M, et al. Diagnostic approach to the hyper-IgE syndromes: Immunologic and clinical key findings to differentiate hyper-IgE syndromes from atopic dermatitis. J Allergy Clin Immunol. 2010;126:611–7.
Baim S, Leonard MB, Bianchi ML, Hans DB, Kalkwarf HJ, Langman CB, et al. Official positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Pediatric Position Development Conference. J Clin Densitorm. 2008;11:6–21.
Bachrach LK, Sills IN. Section on Endocrinology. Clinical report – bone densitometry in children and adolescents. Pediatrics. 2011;127:189–94.
Grimbacher B, Schäffer AA, Holland SM, Davis J, Gallin JI, Malech HL, et al. Genetic linkage of hyper-IgE syndrome to chromosome 4. Am J Hum Genet. 1999;65:735–44.
Zhang Z, Elte T, Troiano N, Maher SE, Fu XY, Bothwell AL. Osteoporosis with increased osteoclastogenesis in hematopoietic cell-specific STAT3-deficient mice. Biochem Biophys Res Commun. 2005;328:800–7.
Woellner C, Gertz EM, Schäffer AA, Lagos M, Perro M, Glocker EO, et al. Mutations in STAT3 and diagnostic guidelines for hyper-IgE. J Allergy Clin Immunol. 2009;125:424–32.
Paulson ML, Freeman AF, Holland SM. Hyper IgE syndrome: an update on clinical aspects and the role of signal transducer and activator of transcription 3. Curr Opin Allergy Clin Immunol. 2008;8:527–33.
Shaw NJ. Management of osteoporosis in children. Eur J Endocrinol. 2008;159:533–9.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scheuerman, O., Hoffer, V., Cohen, A.H. et al. Reduced Bone Density in Patients with Autosomal Dominant Hyper-IgE Syndrome. J Clin Immunol 33, 903–908 (2013). https://doi.org/10.1007/s10875-013-9895-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-013-9895-0