
Abstract
Background
Bicuspid aortic valves (BAVs) are associated with accelerated valvular dysfunction. Increasing rates of conduction system disease are seen in patients with calcific tricuspid aortic valves (TAVs). However, little is known regarding the extent of conduction disorders in BAV patients. We sought to determine the extent of infra-hisian conduction pathology among patients with BAVs undergoing EP studies.
Methods
We prospectively analyzed patients presenting to the EP laboratory from 2006 to 2017 at our institution. Thirty-three BAV patients had measured HV intervals. Each individual was matched by age and gender to two control patients. Clinical characteristics were collected and compared, and patients followed for outcomes.
Results
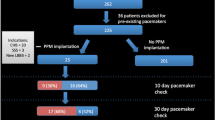
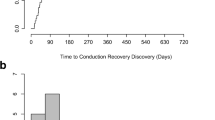
The BAV cohort had a mean age of 47.8 ± 17.2 years (range 19–76 years). Indications for referral to the EP lab in the BAV cohort included SVT ablation (n = 16), VT ablation (n = 10), and EP study for syncope, pre-syncope, or palpitations (n = 29). Patients with BAVs had a mean HV interval of 58.7 ms ± 18.6 ms, compared to a mean of 47.2 ms ± 9.6 ms for controls (p value = 0.0001). Over a 10-year follow-up period, 9 BAV patients (27%) went on to require permanent pacing compared to 6 patients (9%) in the control group (p value = 0.03).
Conclusion
Compared to patients with TAVs presenting for EP evaluation, individuals with BAVs have longer HV intervals and a significantly increased requirement for pacemaker therapy over long-term follow-up. Closer monitoring of progressive conduction system disease in BAV patients may be warranted.



Similar content being viewed by others

Abbreviations
- BAV:
-
Bicuspid aortic valve
- EPS:
-
Electrophysiologic study
- LV EF:
-
Left ventricular ejection fraction
- SVT:
-
Supraventricular tachycardia
- HV:
-
His-ventricular interval
- HTN:
-
Hypertension
References
Siu SC, Silversides CK. Bicuspid aortic valve disease. J Am Coll Cardiol. 2010;55(25):2789–800.
Braverman AC, Guven H, Beardslee MA, Makan M, Kates AM, Moon MR. The bicuspid aortic valve. Curr Probl Cardiol. 2005;30(9):470–522.
Tzemos N, Lyseggen E, Silversides C, Jamorski M, Tong JH, Harvey P, et al. Endothelial function, carotid-femoral stiffness, and plasma matrix metalloproteinase-2 in men with bicuspid aortic valve and dilated aorta. J Am Coll Cardiol. 2010;55(7):660–8.
Kong WKF, Delgado V, Bax JJ. Bicuspid aortic valve: what to image in patients considered for transcatheter aortic valve replacement? Circ Cardiovasc Imaging. 2017;10(9).
Rajamannan NM, Evans FJ, Aikawa E, Grande-Allen KJ, Demer LL, Heistad DD, et al. Calcific aortic valve disease: not simply a degenerative process: a review and agenda for research from the National Heart and Lung and Blood Institute Aortic Stenosis Working Group. Executive summary: calcific aortic valve disease-2011 update. Circulation. 2011;124(16):1783–91.
Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111(24):3316–26.
Ward C. Clinical significance of the bicuspid aortic valve. Heart. 2000;83(1):81–5.
Robicsek F, Thubrikar MJ, Cook JW, Fowler B. The congenitally bicuspid aortic valve: how does it function? Why does it fail? Ann Thorac Surg. 2004;77(1):177–85.
Losenno KL, Goodman RL, Chu MW. Bicuspid aortic valve disease and ascending aortic aneurysms: gaps in knowledge. Cardiol Res Pract. 2012;2012:145202.
Mahadevia R, Barker AJ, Schnell S, Entezari P, Kansal P, Fedak PWM, et al. Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy. Circulation. 2014;129(6):673–82.
van Rosendael PJ, Kamperidis V, Kong WK, et al. Comparison of quantity of calcific deposits by multidetector computed tomography in the aortic valve and coronary arteries. Am J Cardiol. 2016;118(10):1533–8.
Lewin MB, Otto CM. The bicuspid aortic valve: adverse outcomes from infancy to old age. Circulation. 2005;111(7):832–4.
Masri A, Svensson LG, Griffin BP, Desai MY. Contemporary natural history of bicuspid aortic valve disease: a systematic review. Heart. 2017;103(17):1323–30.
Roberts WC. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970;26(1):72–83.
Roberts WC, Vowels TJ, Ko JM. Natural history of adults with congenitally malformed aortic valves (unicuspid or bicuspid). Medicine (Baltimore). 2012;91(6):287–308.
Friedman HS, Zaman Q, Haft JI, Melendez S. Assessment of atrioventricular conduction in aortic valve disease. Br Heart J. 1978;40(8):911–7.
MacMillan RM, Demorizi NM, Gessman LJ, Maranhao V. Correlates of prolonged HV conduction in aortic stenosis. Am Heart J. 1985;110(1 Pt 1):56–60.
Erdogan HB, Kayalar N, Ardal H, Omeroglu SN, Kirali K, Guler M, et al. Risk factors for requirement of permanent pacemaker implantation after aortic valve replacement. J Card Surg. 2006;21(3):211–5 discussion 216-217.
Guglielmetti L, Nazif T, Sorabella R, Akkoc D, Kantor A, Gomez A, et al. Bicuspid aortic valve increases risk of permanent pacemaker implant following aortic root replacement. Eur J Cardiothorac Surg. 2016;50(3):497–503.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39 e14.
Dhingra RC, Amat-y-Leon F, Pietras RJ, et al. Sites of conduction disease in aortic stenosis: significance of valve gradient and calcification. Ann Intern Med. 1977;87(3):275–80.
Calloway TJ, Martin LJ, Zhang X, Tandon A, Benson DW, Hinton RB. Risk factors for aortic valve disease in bicuspid aortic valve: a family-based study. Am J Med Genet A. 2011;155A(5):1015–20.
Girdauskas E, Rouman M, Disha K, Dubslaff G, Fey B, Theis B, et al. Aortopathy in bicuspid aortic valve stenosis with fusion of right-left versus right-non-coronary cusps: are these different diseases? J Heart Valve Dis. 2016;25(3):262–9.
Erkapic D, De Rosa S, Kelava A, Lehmann R, Fichtlscherer S, Hohnloser SH. Risk for permanent pacemaker after transcatheter aortic valve implantation: a comprehensive analysis of the literature. J Cardiovasc Electrophysiol. 2012;23(4):391–7.
Ribeiro V, Mota Garcia R, Frutuoso C, Melão F, Pereira M, Pinho P, et al. Permanent pacemaker implantation after aortic valve replacement: long-term dependency or rhythm recovery? Rev Port Cardiol. 2015;34(9):529–33.
Tarricone R. Cost-of-illness analysis. What room in health economics? Health Policy. 2006;77(1):51–63.
Leyva F. Yes to cardiac devices. But at what cost? Europace. 2013;15(3):313–4.
Fanourgiakis J, Simantirakis E, Maniadakis N, Kourlaba G, Kanoupakis E, Chrysostomakis S, et al. Cost-of-illness study of patients subjected to cardiac rhythm management devices implantation: results from a single tertiary Centre. Europace. 2013;15(3):366–75.
Funding
Drs. Sauer and Nguyen receive significant research grants from Biosense Webster and CardioNXT and educational grants from St. Jude Medical, Boston Scientific, and Medtronic.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Biswas, M., Sandhu, A., Kay, J.D. et al. Patients with bicuspid aortic valves may be associated with infra-hisian conduction disease requiring pacemakers. J Interv Card Electrophysiol 61, 29–35 (2021). https://doi.org/10.1007/s10840-020-00785-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00785-z