
Abstract
Purpose
To assess the subjective quality of anterior segment photos taken from a smartphone camera adapted to the slit lamp compared to a commercial inbuilt slit-lamp camera.
Methods
Non-inferiority study. Five paired images of the anterior segment of normal eyes were taken using an iPhone 11 (Apple, Inc., Calif., USA) camera attached to a universal slit-lamp adaptor and a commercial inbuilt slit-lamp camera (Haag-Streit Diagnostics, Bern, Switzerland). Images were collated into a survey in which ophthalmology students, residents, registrars, and consultants participated to select the image taken from the inbuilt slit-lamp camera. If the image quality was subjectively indistinguishable, we expected a 50:50 split for each photograph that was presented. We selected a 10% non-inferiority margin, with the hypothesis that no less than 40% of images believed to be from the conventional camera were in fact from the smartphone camera.
Results
There were 27 respondents in the survey: ophthalmology consultants (n = 7), registrars (n = 10), residents (n = 7), intern (n = 1) and students (n = 2). The mean correct identification across the respondents was 11.3 out of 25 (45.2%) images. Overall, the smartphone camera was non-inferior to the inbuilt slit-lamp camera (p < 0.001). The non-inferiority of the smartphone camera was significant for consultants (47.4%, p < 0.01), registrars (47.6%, p < 0.001) and residents (37.7%, p < 0.0001).
Conclusions
Anterior segment images obtained with a smartphone camera were non-inferior to the commercial inbuilt slit-lamp camera. Smartphone cameras may be a non-inferior tool for communication of anterior segment images having implications for the ease of access to quality telehealth consultations.
Similar content being viewed by others


Introduction
In Australia, approximately 1.4% of all emergency department (ED) presentations are related to eye disorders [2]. Anterior segment pathology accounts for more than 90% of ED presentations related to eye disorders [3]. Specialist consultation is frequent given medical officers report decreasing confidence in slit lamp usage and management of ocular emergencies in the ED [4].
Ophthalmology consults may be performed virtually with the use of high-quality photographs, increasingly relevant with the increased uptake of telemedicine in response to the COVID-19 pandemic [5, 6]. Inbuilt slit-lamp cameras are an effective means for anterior segment photography. Despite a large proportion of EDs having access to slit lamps, medical officers report a lack of training to use them [7]. In addition, rural EDs are less likely to have access to slit lamps [8].
Conversely, smartphones are widely available and offer a wide range of functionalities. The increasing camera quality of smartphones, low cost and universality have sparked interest in their utility in ophthalmology [9]. Slit lamp photography is possible with the use of inexpensive smartphone adaptors that offer comparable image quality to inbuilt slit-lamp cameras. Observations made by previous investigators have demonstrated smartphone cameras offering good image quality, however, reproducibility and agreement on this are lacking [10,11,12,13].
Given the ease of access to a smartphone camera, there may be a role in using them to image anterior segment pathology in primary and tertiary care centres. This can be used for consultation purposes without the need for specialised slit-lamp cameras. This pilot study was designed to assess whether ophthalmology staff can discriminate between images taken of the anterior segment in healthy eyes from an inbuilt slit-lamp microscope camera compared to that of a smartphone camera attached to a universal slit-lamp adaptor.
Methods
All participants were recruited from the Royal Adelaide Hospital (RAH) Ophthalmology Department. Ethics approval was acquired from the local Human Research Ethics Committee at the Central Adelaide Local Health Network Research office (reference 13716). Consent was obtained from five staff volunteers in the department to acquire images of their anterior segment. An inexpensive adjustable slit-lamp phone adaptor was utilised as depicted in Fig. 1 [14]. The iPhone 11 (Apple, Inc., Cupertino, Calif., USA) was mounted onto the adaptor and placed over the right eyepiece of the slit lamp (Fig. 2). At the time, iOS™ (14.3) software was installed on the iPhone 11.

Adjustable slit-lamp adaptor used to attach the smartphone to the slit lamp eyepiece

Set-up of the slit lamp adaptor on the Haag-Streit BQ-900 slit-lamp using an iPhone 11 (Apple, Inc., Cupertino, Calif., USA)
A survey with each pair of images for all subjects was created using Google Forms (Alphabet Inc., California, USA). An invitation link to the survey was provided to medical students, interns, ophthalmology residents (i.e., unaccredited trainees), registrars (i.e., accredited trainees), consultant ophthalmologists. Participants were given the option of answering anonymously and recording their level of expertise. The survey consisted of 25 comparison questions and was blinded to individuals who were not involved in the imaging process. The questions asked the participants to select image captured by the commercial slit-lamp camera (Figs. 3 and 4). The correct responses were recorded.

Diffuse Illumination example photo of a participant. Left: image taken using iPhone 11. Right: image taken using Image module IM-900 of the slit lamp

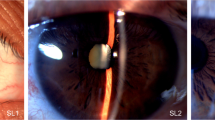
Corneal slit photographs were taken by the iPhone 11 (left) and the built-in slit lamp camera (right)
Survey design sample size calculations allowing for correlated data indicated that approximately 650 data points would be required to detect a 10% margin in non-inferiority where the null hypothesis assumed a 50:50 split with 80% power and alpha at 0.05. The p-values were calculated with a z-test and the correct variance estimate on the proportion was calculated by modelling the study as a clustered design using the survey package in R (version 4.0) with the individual as the unit of a cluster [15, 16]. A Bonferroni correction was applied for sub-group analyses.
The slit-lamp images were taken using the integrated Haag-Streit IM900 Imaging module with Eyesuite™ software (Haag-Streit Diagnostics, Bern, Switzerland) [17]. The same iPhone and slit lamp were used throughout the study. Two medical officers (MO) took sets of three photographs using both cameras, for five separate imaging techniques. These techniques were diffuse illumination, narrow corneal slit, sclerotic scatter, lens optical section, and iris retro-illumination (see Appendix, Table 1s@@). The anterior segment photos were captured simultaneously using the two cameras where one MO captured photos using the smartphone on the slit lamp, whilst the other using the Eyesuite™ software on the computer.
The settings enabled on the iPhone camera included ‘high dynamic range (HDR)’ and ‘autofocus’. The slit lamp settings were adjusted based on the imaging technique but were kept constant for all the subjects (see Appendix, Table 1s@@). The best quality images were chosen from a set of three, to simulate out-of-study conditions in which the best photos of multiple would be selected. The pairs of photos were cropped using Adobe Lightroom™ 4.1.1 (Adobe, San Jose, California, USA) to display similar structures in each photo. The cropped images were then light adjusted using Lightroom’s Auto function, in conjunction with adjusting the Exposure slider, to display visibly equal exposure. This was done to ensure survey participants would only use photo quality to discriminate the image pairs and prevent different light exposure or field angles to influence the result. The time taken for this was approximately a minute for each set of photos.
Results
Twenty-seven respondents completed the survey comprising twenty-five image questions and two quality control questions. There was a total of 675 data points extracted from the survey. Overall, the respondents achieved a mean correct score of 11.3 out of 25 (45.2%, SD 14.0) in the survey for correctly identifying the inbuilt slit lamp photos. Thus, 54.8% of respondents believed the smartphone camera was the commercial slit-lamp camera image, signifying that the smartphone camera is non-inferior to the inbuilt slit-lamp camera (z-test, p-value < 0.001). The mean score for each subset of images is shown in Fig. 5.

Mean score for each type of image. Note: All survey respondents were used for this calculation. No cohort was omitted
The survey also noted the category of the respondent as a consultant, registrar, resident, intern or student. The survey was mostly completed by the consultants 25.9% (n = 7), registrars 37% (n = 10) and residents 25.9% (n = 7). The other respondents were interns 3.7% (n = 1) and students 7.4% (n = 2). The consultant group were accurate 47.4% of the time incorrectly identifying slit-lamp camera image (p-value < 0.01). Similarly, registrars had a correct guess rate of 47.6% for slit-lamp images (p-value < 0.001) of the time and the residents strongly favoured the smartphone camera with only 37.7% correct guess rate for slit lamp images (p-value < 0.0001). The correct guess rate for slit-lamp photos is depicted in Table 1.
Respondents were asked if the images were of comparable quality and 20 out of 27 respondents (74.1%) believed they were. The respondents who did not agree with this finding achieved a mean score of 9.3 out of 25 (n = 7, 37.2%), compared to those that agreed had a mean score of 12 (n = 20, 48%) for correctly identifying slit lamp photos. Respondents also reported the difficulty experienced in comparing images as per Fig. 6.

Difficulty reported by participants in differentiating between the images
Discussion
In this study conducted by medical personnel with varying ophthalmic expertise, the smartphone camera was non-inferior to the commercial inbuilt slit-lamp camera. This suggests that adequate anterior segment imaging can be obtained without specialist equipment, offering more accessible telehealth opportunities for consultation and specialist opinion. This may reduce the time for specialist involvement in patient care and provide cost savings by reducing the need for expensive photographic equipment.
The pandemic era paves the way for smartphone devices to be used as a valuable tool for telehealth consultations in ophthalmology. Uses range from a tool to detect ptosis, cataracts, measurement of toric alignment, evaluation of globe anatomy and trachoma surveillance [18,19,20,21,22,23]. Previous pilot studies have shown that anterior segment photos taken through smartphone cameras such as the iPhone 4 s and 5 s were all of poorer quality when compared to the Zeiss photo slit lamp camera (Carl Zeiss Meditec, Dublin, Calif., USA) [24]. Others have studied anterior segment images post-cataract operation or with the use of different smartphone attachments such as the 90-dioptre lens [25,26,27,28,29]. None of these studies have compared if the subjective quality of anterior segment images captured by a smartphone camera and an inbuilt slit-lamp camera.
In contrast to the above studies, this study shows that anterior segment images taken from iPhone 11 are non-inferior to the Haag Streit BQ-900 imaging module as perceived by the ophthalmology staff. Interestingly, the resident group tended to strongly favour the smartphone images, as they correctly identified the slit lamp photos only 37.7% of the time. This preference of the resident group may be due to their education level, age, and smartphone usage which can cause deviation in the results.
The reasons for non-inferiority are multifactorial. The 12-megapixel camera on the iPhone 11 is comparable to the high sensitivity and a wide dynamic range provided by the Haag Streit Imaging Module (IM) 900. The resolution offered by iPhone 11 camera (4032-by-3024 pixels) is superior to the Haag-Streit IM 900 module (1920-by-1200 pixels) [17, 30, 31]. The other key differences are the software and functionalities of the two cameras. Similar to other smartphones, the iPhone 11 offers features such as auto-focus and optical image stabilisation capabilities that the IM 900 module does not. However, it can be argued that the IM 900 has superior stabilisation abilities as it is integrated into the slit lamp as compared to the smartphone attached to an adaptor which requires adjustments. Furthermore, the software of the iPhone 11 obtains up to 10 updates every year as compared to just an annual update for the IM 900 module which may enhance its camera’s performance [32, 33].
This study shows that the combination of a slit-lamp adaptor and smartphone has its advantages. Firstly, the adaptors are inexpensive, such as the one used in this pilot study (AUD $20) as compared to inbuilt slit-lamp cameras which costs upwards of AUD $20,000 (excluding costs of ongoing maintenance) [14, 34]. Secondly, the slit lamp illumination system provides clear image quality at higher magnification due to the reduced focusing distance to the eye [35]. The smartphone uses the slit lamp’s illumination at magnification to capture sharper images as compared to using the zoom function on the smartphone alone. No additional light source from the smartphone also results in decreased reflection on the ocular surface [36]. Lastly, the adaptors can be attached to most smartphones, are transportable and suitable for most slit lamps.
Applications of images captured from this setup are numerous. Sink, Blatt, Yoo et al. compared diagnosis achieved through remote smartphone photographs to those of in-office exams for common ophthalmology presentations such as external eye diseases or red-eye pathology. The results showed that the remote and in-office diagnosis made by different specialists were in agreement 93% of the time [37]. This pilot study supports the use of anterior segment images acquired with a smartphone camera to diagnose anterior segment pathology as they are similar to the inbuilt slit lamp camera. The inbuilt slit lamp camera is usually the benchmark for taking ocular photos and as the ophthalmology staff are unable to distinguish between the two cameras, they will likely find the smartphone images to be sufficient to make a diagnosis. Furthermore, new smartphone cameras providing stereoscopic images allow for tele-ophthalmology viewers to see in 3D similar to a slit lamp, furthering the potential applicability of these mounts [38, 39]. This can also be integrated with machine learning in the future to assess for anterior chamber depth and grading of cataracts which has potential generalizability to the primary care setting [39, 40].
There are some issues with the two imaging systems that can hinder the quality of photographs. The inbuilt slit-lamp cameras are often subject to availability and are only present in well-established ophthalmology clinics. They require integrated storage space on local computers and images are not as portable. Secondly, in our experience we found a small delay between pressing the capture button to when the image is acquired. This may interfere with the quality of the image due to patient movement. Conversely, the adaptor has inherent issues such as difficulty in attachment to the rubber ring on the eyepiece. If this occurs, an alternative is to place double sided tape on the adapter to allow for better fixation. Moreover, the depth of eye piece fixation ring is often shallow and may not always bear the weight of smartphone. Thus, removal of any protective cases or accessories on the phone may allow the adapter to hold the weight of the smartphone. Also, we found that having one hand on the smartphone and other on the slit lamp for manoeuvring provided stability in capturing photos. The quality of photos may differ between each doctor using the adapter, however, with basic slit lamp examination skills it should still produce good quality photos with a short learning curve.
The limitations of the study are that it does not apply to fundus photographs captured by a smartphone camera as others have previously compared [41]. The sample size of the study was dependent on the limited number of ophthalmology staff in the department. Only ophthalmology staff were used in the survey due to their more experience and knowledge of the slit lamp and ocular anatomical structures. However, this study could be replicated at a larger scale including other disciplines in the future. Lastly, the software used for light-adjusting photos was not completely automated and subject to user bias.
Conclusion
This pilot study demonstrates that photos captured by a smartphone camera are non-inferior to those taken with an inbuilt slit lamp camera as discriminated by medical staff in our Ophthalmology department. Anterior segment images can be captured by clinicians with the use of an inexpensive slit lamp adaptor in the absence of inbuilt photography modules. This increases the accessibility of tele-ophthalmic consultation for expert opinion in settings without proximate ophthalmologists or specialised ophthalmic imaging equipment.
Availability of data and material
Able to easily access data on the surveys through Google Forms.
Code availability
Not applicable.
References
Goel RMC, Bahrami B, Casson R, Chan W (2022) Assessing the subjective quality of anterior segment photography. Royal Aust N Z Sci Congr. https://doi.org/10.1111/ceo.14014.MeetingAbstracts873-977
AIHW (2018) Emergency department care, 2019–20 Australian hospital statistics; https://www.aihw.gov.au/reports-data/myhospitals/sectors/emergency-department-care. Accessed Dec 2021
Channa R, Zafar SN, Canner JK, Haring RS, Schneider EB, Friedman DS (2016) Epidemiology of eye-related emergency department visits. JAMA Ophthalmol 134(3):312–319
Sim D, Hussain A, Tebbal A, Daly S, Pringle E, Ionides A (2008) National survey of the management of eye emergencies in the accident and emergency departments by senior house officers: 10 years on—has anything changed? Emerg Med J 25(2):76–77
Sommer AC, Blumenthal EZ (2020) Telemedicine in ophthalmology in view of the emerging COVID-19 outbreak. Graefes Arch Clin Exp Ophthalmol 258(11):2341–2352
Saleem SM, Pasquale LR, Sidoti PA, Tsai JC (2020) Virtual ophthalmology: telemedicine in a COVID-19 era. Am J Ophthalmol 216:237–242
Sim PY, La CJ, Than J, Ho J (2020) National survey of the management of eye emergencies in the accident and emergency department by foundation doctors: has anything changed over the past 15 years? Eye 34(6):1094–1099
Tauber J, Ayoub S, Shah P, Wu M, Tsui E, Schuman JS et al (2020) Assessing the demand for teleophthalmology in florida emergency departments. Telemed e-Health 26(12):1500–1506
Chan JB, Ho HC, Ngah NF, Hussein E (2014) DIY - smartphone slit-lamp adaptor. J Mobile Technol Med 3(1):16–22
Bhatter P, Cao L, Crochetiere A, Raefsky SM, Cuevas LR, Enendu K et al (2020) Using a macro lens for anterior segment imaging in rural panama. Telemed J E Health 26(11):1414–1418
Pujari A, Mukhija R, Singh AB, Chawla R, Sharma N, Kumar A (2018) Smartphone-based high definition anterior segment photography. Indian J Ophthalmol 66(9):1375–1376
Pujari A, Behera AK, Agarwal D, Sihota R, Dada T (2020) A New technique of iPhone 11 pro max smartphone-aided angle video and standstill image documentation. J Glaucoma 29(5):e28–e30
Pujari A, Saluja G, Agarwal D, Selvan H, Sharma N (2020) Clinically useful smartphone ophthalmic imaging techniques. Graefe’s Arch Clin Exp Ophthalmol 259(2):279–287. https://doi.org/10.1007/s00417-020-04917-z
AliExpress (2020) Universal Smart Phone Cellphone Slit Lamp Adapter AliExpress; https://www.aliexpress.com/i/32964308307.html Accessed Dec 2021
R Core Team (2020) A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/. Accessed Dec 2021
Lumley T (2020) "survey: analysis of complex survey samples". R package version 4.0.
Haag-Streit (2016) Slit lamp imaging guide, 9th edn. Haag-Streit, Switzerland
Hogarty DT, Hogarty JP, Hewitt AW (2020) Smartphone use in ophthalmology: what is their place in clinical practice? Surv Ophthalmol 65(2):250–262
Kumar N, Bandello F, Sharma A (2019) Smartphone-based Gonio-imaging: a novel addition to glaucoma screening tools. J Glaucoma 28(9):e149–e150
Snyder BM, Sié A, Tapsoba C, Dah C, Ouermi L, Zakane SA et al (2019) Smartphone photography as a possible method of post-validation trachoma surveillance in resource-limited settings. Int Health 11(6):613–615
Brennan PF, McNeil AJ, Jing M, Awuah A, Finlay DD, Blighe K et al (2019) Quantitative assessment of the conjunctival microcirculation using a smartphone and slit-lamp biomicroscope. Microvasc Res 126:103907
Pujari A, Selvan H, Asif MI, Gupta B, Dada T (2019) Smartphone-aided quantification of iridocorneal angle. J Glaucoma 28(9):e153–e155
Nesemann JM, Seider MI, Snyder BM, Maamari RN, Fletcher DA, Haile BA et al (2020) Comparison of smartphone photography, single-lens reflex photography, and field-grading for trachoma. Am J Trop Med Hyg 103(6):2488–2491
Jalil M, Ferenczy SR, Shields CL (2017) iPhone 4s and iPhone 5s imaging of the eye. Ocul Oncol Pathol 3(1):49–55
Fliotsos MJ, Deljookorani S, Dzhaber D, Chandan S, Ighani M, Eghrari AO (2020) Qualitative and quantitative analysis of the corneal endothelium with smartphone specular microscopy. Cornea 39(7):924–929
Kaya A (2017) Ophthoselfie: detailed self-imaging of cornea and anterior segment by smartphone. Turk J Ophthalmol 47(3):130–132
Sanguansak T, Morley K, Morley M, Kusakul S, Lee R, Shieh E et al (2017) Comparing smartphone camera adapters in imaging post-operative cataract patients. J Telemed Telecare 23(1):36–43
Mohammadpour M, Mohammadpour L, Hassanzad M (2016) Smartphone assisted slit lamp free anterior segment imaging: a novel technique in teleophthalmology. Cont Lens Anterior Eye 39(1):80–81
Barsam A, Bhogal M, Morris S, Little B (2010) Anterior segment slitlamp photography using the iPhone. J Cataract Refract Surg 36(7):1240–1241
(Australia) A iPhone 11 - Technial Specifications: Apple. https://www.apple.com/au/iphone-11/specs/. Accessed Dec 2021
Haag-Streit (2019) Slit lamp BQ 900. Haag-Streit, Zurich
Apple About iOS 14 Updates Apple Support: Apple. https://support.apple.com/en-us/HT211808. Accessed Dec 2021
Haag-Streit (2019) Imaging modules IM 900 & IM 600, 8th edn. Haag-Streit, Switzerland
Chan JB, Ho HC, Ngah NF, Hussein E (2014) DIY-smartphone slit-lamp adaptor. J Mobile Technol Med 3(1):16–22
Kalra G, Ichhpujani P, Thakur S, Singh RB, Sharma U, Kumar S (2021) A pilot study for smartphone photography to assess bleb morphology and vasculature post- trabeculectomy. Int Ophthalmol 41:483–490
Myung D, Jais A, He L, Chang RT (2014) Simple, low-cost smartphone adapter for rapid, high quality ocular anterior segment imaging: a photo diary. J Mobile Technol Med 3(1):2–8
Sink J, Blatt S, Yoo D, Henry M, Yang SD, Vasaiwala R et al (2020) A novel telemedicine technique for evaluation of ocular exam findings via smartphone images. J Telemed Telecare 28:197–202
Solyman O, Ahmad M, Arora K, Henderson AD, Carey A (2021) Stereoscopic three-dimensional (3D) slit-lamp photography using a compact 3D digital camera. Indian J Ophthalmol 69(5):1303–1305
Hu S, Wu H, Luan X, Wang Z, Adu M, Wang X et al (2020) Portable handheld slit-lamp based on a smartphone camera for cataract screening. J Ophthalmol 2020:1037689
Chen D, Ho Y, Sasa Y, Lee J, Yen CC, Tan C (2021) Machine learning-guided prediction of central anterior chamber depth using slit lamp images from a portable smartphone device. Biosensors 11(6):182
Bifolck E, Fink A, Pedersen D, Gregory T (2018) Smartphone imaging for the ophthalmic examination in primary care. Jaapa 31(8):34–38
Kalra G, Ichhpujani P, Thakur S, Singh RB, Sharma U, Kumar S (2021) A pilot study for smartphone photography to assess bleb morphology and vasculature post- trabeculectomy. Int Ophthalmol. 41:483–490.
Sink J, Blatt S, Yoo D, Henry M, Yang SD, Vasaiwala R et al (2020) A novel telemedicine technique for evaluation of ocular exam findings via smartphone images. J Telemed Telecare 28:197–202
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. No funding was acquired for the research project.
Author information
Authors and Affiliations
Contributions
Dr RG: Manuscript preparation, Literature review, Photography and creation of surveys. Dr CM: Drafting process, literature review and photography assistance. Dr BB: Manuscript drafting process, Ethics application and consent forms. Professor RC: Manuscript drafting process. Dr WC: Manuscript drafting, provision of slit lamp adaptor and research idea.
Corresponding author
Ethics declarations
Conflicts of interest
No conflicts of interest to declare.
Consent to participate
Volunteers were asked to sign a consent process prior to agreeing for eyes to be photographed.
Ethical approval
Gained from the Central Adelaide Local Health Network Human Research and Ethics Committee, Reference number 13716.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Presented as a poster at the Royal Australian and New Zealand College of Ophthalmologists 52nd Annual Scientific Congress, February 26- March 1 2022 [1].
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Goel, R., Macri, C., Bahrami, B. et al. Assessing the subjective quality of smartphone anterior segment photography: a non-inferiority study. Int Ophthalmol 43, 403–410 (2023). https://doi.org/10.1007/s10792-022-02437-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-022-02437-9