
Abstract
Purpose
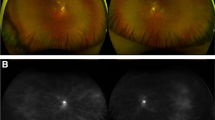
To report continuing diffuse retinal dysfunction following resolution of immune reconstitution uveitis (IRU) in patients with cytomegalovirus retinitis (CMVR).
Methods
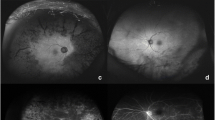
Retrospective case series describing two patients with IRU following CMVR who underwent serial fundus photography and macular optical coherence tomography. One patient had serial electrophysiology.
Results
Both patients had CMVR successfully treated with antiviral medication. The affected eyes later developed IRU that resolved with steroids. However, following resolution, chronic retinal damage was evidenced by ellipsoid line loss in one case and gradual optic disc cupping in the other. Electrophysiology in both cases revealed generalized retinal dysfunction worse in the eye with more severe IRU and demonstrated objectively the efficacy of treatment intervention in the patient with serial recordings.
Conclusions
Patients with IRU following CMV retinitis may have continuing diffuse retinal dysfunction despite apparent recovery and normal visual acuity. An aggressive approach to inflammation control may be warranted in such patients.




Similar content being viewed by others

References
Stoll M, Schmidt RE (2003) Immune restoration inflammatory syndromes: the dark side of successful antiretroviral treatment. Curr Infect Dis Rep 5(3):266–276
Yanagisawa K, Ogawa Y, Hosogai M et al (2017) Cytomegalovirus retinitis followed by immune recovery uveitis in an elderly patient with rheumatoid arthritis undergoing administration of methotrexate and tofacitinib combination therapy. J Infect Chemother 23(8):572–575. https://doi.org/10.1016/j.jiac.2017.03.002
Downes KM, Tarasewicz D, Weisberg LJ, Cunningham ET (2016) Good syndrome and other causes of cytomegalovirus retinitis in HIV-negative patients—case report and comprehensive review of the literature. J Ophthalmic Inflamm Infect 6(1):3. https://doi.org/10.1186/s12348-016-0070-7
Robinson MR, Reed G, Csaky KG, Polis MA, Whitcup SM (2000) Immune-recovery uveitis in patients with cytomegalovirus retinitis taking highly active antiretroviral therapy. Am J Ophthalmol 130(1):49–56
Yeo TH, Yeo TK, Wong EP, Agrawal R, Teoh SC (2016) Immune recovery uveitis in HIV patients with cytomegalovirus retinitis in the era of HAART therapy-a 5-year study from Singapore. J Ophthalmic Inflamm Infect 6(1):41. https://doi.org/10.1186/s12348-016-0110-3
Lin Y-C, Yang C-H, Lin C-P et al (2008) Cytomegalovirus retinitis and immune recovery uveitis in AIDS patients treated with highly active antiretroviral therapy in Taiwanese. Ocul Immunol Inflamm 16(3):83–87. https://doi.org/10.1080/09273940802056307
Karavellas MP, Lowder CY, Macdonald C, Avila CP, Freeman WR (1998) Immune recovery vitritis associated with inactive cytomegalovirus retinitis: a new syndrome. Arch Ophthalmol (Chicago, Ill. 1960) 116(2):169–175
Zegans ME, Walton RC, Holland GN, O’Donnell JJ, Jacobson MA, Margolis TP (1998) Transient vitreous inflammatory reactions associated with combination antiretroviral therapy in patients with AIDS and cytomegalovirus retinitis. Am J Ophthalmol 125(3):292–300
Rangel CM, Prada AM, Varon C, Merayo-Lloves J (2015) Immune recovery uveitis in a patient with previously undiagnosed cytomegalovirus retinitis. BMJ Case Rep. https://doi.org/10.1136/bcr-2015-212095
Goldberg DE, Wang H, Azen SP, Freeman WR (2003) Long term visual outcome of patients with cytomegalovirus retinitis treated with highly active antiretroviral therapy. Br J Ophthalmol 87(7):853–855
El-Bradey MH, Cheng L, Song M-K, Torriani FJ, Freeman WR (2004) Long-term results of treatment of macular complications in eyes with immune recovery uveitis using a graded treatment approach. Retina 24(3):376–382
Kempen JH, Min Y-I, Freeman WR et al (2006) Risk of immune recovery uveitis in patients with AIDS and cytomegalovirus retinitis. Ophthalmology 113(4):684–694. https://doi.org/10.1016/j.ophtha.2005.10.067
Urban B, Bakunowicz-Łazarczyk A, Michalczuk M (2014) Immune recovery uveitis: pathogenesis, clinical symptoms, and treatment. Mediators Inflamm. https://doi.org/10.1155/2014/971417
Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group (2005) Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 140(3):509–516. http://www.ncbi.nlm.nih.gov/pubmed/16196117
Lenassi E, Robson AG, Hawlina M, Holder GE (2012) The value of two-field pattern electroretinogram in routine clinical electrophysiologic practice. Retina 32:588–599. https://doi.org/10.1097/IAE.0b013e31822059ae
McCulloch DL, Marmor MF, Brigell MG et al (2015) ISCEV Standard for full-field clinical electroretinography (2015 update). Doc Ophthalmol 130(1):1–12. https://doi.org/10.1007/s10633-014-9473-7
Bach M, Brigell MG, Hawlina M et al (2013) ISCEV standard for clinical pattern electroretinography (PERG): 2012 update. Doc Ophthalmol 126(1):1–7. https://doi.org/10.1007/s10633-012-9353-y
Berthe P, Baudouin C, Garraffo R, Hofmann P, Taburet AM, Lapalus P (1994) Toxicologic and pharmacokinetic analysis of intravitreal injections of foscarnet, either alone or in combination with ganciclovir. Invest Ophthalmol Vis Sci 35(3):1038–1045
Müller M, Wandel S, Colebunders R et al (2010) Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis 10(4):251–261. https://doi.org/10.1016/S1473-3099(10)70026-8
Gupta MP, Patel S, Orlin A et al (2018) Spectral domain optical coherence tomography findings in macula-involving cytomegalovirus retinitis. Retina 38(5):1000–1010. https://doi.org/10.1097/IAE.0000000000001644
Latkany PA, Holopigian K, Lorenzo-Latkany M, Seiple W (1997) Electroretinographic and psychophysical findings during early and late stages of human immunodeficiency virus infection and cytomegalovirus retinitis. Ophthalmology 104(3):445–453
Donahue SP (1998) Human immunodeficiency virus-associated vision loss: electroretinogram attenuation. Am J Ophthalmol 126(5):729–731
Moschos MM, Margetis I, Markopoulos I, Moschos MN (2011) Optical coherence tomography and multifocal electroretinogram study in human immunodeficiency virus-positive children without infectious retinitis. Clin Exp Optom 94(3):291–295. https://doi.org/10.1111/j.1444-0938.2011.00603.x
Cantrill HL, Ramsay RC, Knobloch WH, Purple RL (1981) Electrophysiologic changes in chronic pars planitis. Am J Ophthalmol 91(4):505–512
Holder GE, Robson AG, Pavesio C, Graham EM (2005) Electrophysiological characterisation and monitoring in the management of birdshot chorioretinopathy. Br J Ophthalmol 89(6):709–718. https://doi.org/10.1136/bjo.2004.047837
Schrier RD, Song M-K, Smith IL et al (2006) Intraocular viral and immune pathogenesis of immune recovery uveitis in patients with healed cytomegalovirus retinitis. Retina 26(2):165–169
Karavellas MP, Azen SP, MacDonald JC et al (2001) Immune recovery vitritis and uveitis in AIDS: clinical predictors, sequelae, and treatment outcomes. Retina 21(1):1–9
Dunn JP (1998) Immune recovery vitritis in HIV infection: abstracts and commentary. JAMA 280(2):185–186
Holland GN (2008) AIDS and ophthalmology: the first quarter century. Am J Ophthalmol 145(3):397-408.e1. https://doi.org/10.1016/j.ajo.2007.12.001
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. None of the authors have a proprietary interest in the material submitted.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Summary statement
Patients with immune reconstitution uveitis following cytomegalovirus retinitis may have continuing diffuse retinal dysfunction despite apparent full clinical recovery and normal visual acuity. Electrophysiology reveals the extent and severity of retinal dysfunction and informs management.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yuen, Y.S., Holder, G.E., Lingam, G. et al. Diffuse retinal dysfunction following immune reconstitution uveitis in patients with prior cytomegalovirus retinitis: a novel observation. Doc Ophthalmol 147, 139–145 (2023). https://doi.org/10.1007/s10633-023-09947-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-023-09947-6