
Abstract
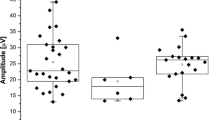
To investigate the retinal development in healthy preterm infants through standard ganzfeld electroretinograms (ERG) and compare the difference of ERG between the healthy preterm and term infants. Forty-nine 49 healthy infants were recruited to this study, including 20 preterm and 29 term infants. All the infants were grouped as follows: term 40 W group (ERG recorded at birth), term 44 W group (ERG recorded at 4 weeks after birth), preterm 35 W group (ERG recorded at birth) and preterm 40 W group (ERG recorded at due date). Standard ganzfeld flash ERG was performed according to the ISCEV standard for the clinical electroretinogram (2008). The ERG amplitudes in the term 44 W group were notably larger than those of the term 40 W group, but there was no significant difference between the two groups for combined-b and cone-b responses. The implicit time of cone-b, combined-a and 30 Hz in term 44 W group was significantly shorter than that in term 40 W group, and there was no significant difference in other ERG responses between the two groups. Amplitude of ERG waves in preterm 35 W group was only 48.7–78.0% of that in term 40 W group, and the difference of all ERG waves between the two groups was statistically significant, but there was no significant difference between the two groups for implicit time of all responses except rod-b. There was no significant difference between the amplitude of ERG waves in term 40 W and preterm 40 W groups; however, implicit time of cone-a and cone-b in term 40 W is significantly longer than that in preterm 40 W group. The ERG amplitudes in the preterm 35 W group were notably smaller than those of the preterm 40 W group, and except cone-a response, the difference between the two groups was statistically significant, while the difference of the implicit time between the two groups was not significant. OPs could not be recorded in some infants. OPs were seen significantly less frequently in the preterm 35 W group than in either the term 40 W group (Fisher exact test, P = 0.006) or the term 44 W group (Fisher exact test, P = 0.02). No other significant inter-group frequency differences were found. The mean amplitude ratio b/a was not significantly different between the four groups (P > 0.05) (analysis of variance). The retina is not fully developed at birth in healthy preterm infants. The preterm ISCEV ERG matures rapidly after birth and by term reaches the degree of maturation found in term born neonates.


Similar content being viewed by others

References
Winkelman JE, Horsten GP (1962) The ERG of Premature and Full-Term Born Infants during their First Days of Life. Ophthalmologica 143:92–101
Mactier H, Dexter JD, Hewett JE, Latham CB, Woodruff CW (1988) The electroretinogram in preterm infants. J Pediatr 113:607–612
Mets MB, Smith VC (1995) Postnatal retinal development as measured by the electroretinogram in premature infants. Doc Ophthalmol 90:111–127
Fulton AB, Hansen RM (1996) Photoreceptor function in infants and children with a history of mild retinopathy of prematurity. J Opt Soc Am A 13:566–571
Fulton AB, Hansen RM (1996) Electroretinogram responses and refractive errors in patients with a history of retinopathy of prematurity. Doc Ophthalmol 91:87–100
Kennedy KA, Ipson MA, Birch DG, Tyson JE, Anderson JL, Nusinowitz S, West L, Spencer R, Birch EE (1997) Light reduction and the electroretinogram of preterm infants. Arch Dis Child 76:F168–F173
Mactier H, Hamilton R, Bradnam MS, Turner TL, Dudgeon J (2000) Contact lens electroretinography in preterm infants from 32 weeks after conception: a development in current methodology. Arch Dis Child Fetal Neonatal Ed 82:F233–F236
Berezovsky A, Moraes NSB, Nusinowitz S, Salomao SR (2003) Standard full-field Electroretinography in healthy preterm infants. Doc Ophthalmol 107:243–249
Hamilton R, Bradnam MS, Dudgeon J, Mactier MH (2008) Maturation of Rod Function in Preterm Infants with and without Retinopathy of Prematurity. J Pediatr 153:605–611
Marmor MF, Fulton AB, Holder GE, Miyake Y, Brigell M, Bach M (2009) ISCEV Standard for full-field clinical electroretinography (2008 update). Doc Ophthalmol 118:69–77
Hendrickson A, Drucker D (1992) The development of parafoveal and mid-peripheral human retina. Behav Brain Res 49:21–31
Grose J, Harding GFA, Wilton AY, Bissenden JG (1989) The maturation of the pattern-reversal VEP and flash ERG in pre-term infants. Clin Vision Sci 4:239–246
Birch EE, Birch DG, Petrig B, Uauy R (1990) Retinal and cortical function of very low birthweight infants at 36 and 57 weeks postconception. Clin Vision Res 5:363–373
van Hof V, Duin J, Mohn G (1986) The development of visual acuity in normal fullterm and preterm infants. Vision Res 26:909–916
Leaf AA, Green CR, Esack A, Costeloe KL, Prior PF (1995) Maturation of electroretinograms and visual evoked potentials in preterm infants. Dev Med Child Neurol 37:814–826
Westall CA, Panton CM, Levin AV (1999) Time courses for maturation of electroretino-gram responses from infancy to adulthood. Doc Ophthalmol 96:355–379
Moskowitz A, Hansen RM, Fulton AB (2005) ERG oscillatory potentials in infants. Doc Ophthalmol 110:265–270
Flores-Guevara R, Renault F, Ostre C, Richard P (1996) Maturation of the electroretinogram in children: stability of the amplitude ratio a/b. Electroencephalogr Clin Neurol 100:422–427
Breton ME, Quinn GE, Schueller AW (1995) Development of electroretinogram and rod phototransduction response in human infants. Invest Ophthalmol Vis Sci 36:1588–1602
Tremblay F, Parkinson JE (2003) Alteration of electroretinographic recordings when performed under sedation or halogenate anesthesia in a pediatric population. Doc Ophthalmol 107:271–279
Fulton AB, Hansen RM, Westall CA (2003) Development of ERG responses: The ISCEV rod, maximal and cone responses in normal subjects. Doc Ophthalmol 107:235–241
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhou, X., Huang, X., Chen, H. et al. Comparison of electroretinogram between healthy preterm and term infants. Doc Ophthalmol 121, 205–213 (2010). https://doi.org/10.1007/s10633-010-9248-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-010-9248-8