
Abstract
Background
The outbreak of COVID19 evolved rapidly into a global pandemic, forcing hospitals, including inflammatory bowel disease (IBD) referral units, to change their practices to ensure quality of care.
Aims
To describe the clinical outcomes and the fulfilment of the treatment schedule of patients with IBD treated with biological agents in a single-center of a red-zone of the pandemic, and to report the patients’ perceptions about COVID-19 and the measures adopted at our center.
Methods
Therapeutic adherence and clinical outcomes were collected for all patients undergoing treatment with intravenous biologicals and subcutaneous biologicals at our center. A telephone survey was also performed to assess these patients’ perceptions of the COVID pandemic and the related measures adopted at their IBD unit.
Results
A total of 234 patients were included (117 on intravenous and 117 on subcutaneous biologicals). Only 10% of patients postponed intravenous infusions intentionally and 5% postponed the collection of subcutaneous biologicals at the hospital pharmacy. Only five confirmed COVID-19 cases were registered (2.1%), all of them of mild severity. One hundred and fifty-five patients participated in the survey (77 on intravenous and 78 on subcutaneous drugs). Fear of going to the hospital was the most common reason for postponing biological administrations. Among those on combination therapy, only 7% admitted to have withdrawn immunosuppressants.
Conclusions
Adherence to intravenous and subcutaneous biological therapies during the pandemic was high in a single-center cohort of IBD patients even though the cumulative incidence of confirmed COVID-19 was low.
Similar content being viewed by others


Introduction
The World Health Organization officially declared coronavirus disease 2019 (COVID-19) to be a pandemic on March 11. On March 14, when almost 6000 confirmed cases had been diagnosed in the country, the Spanish Government declared a state of emergency with a complete national lockdown and social distancing measures. At that time, in order to limit the spread of the infection, most of the referral IBD units in Spain had already applied general measures such as the cancellation of elective onsite consultation, elective endoscopic examinations and surgeries, and the widespread use of telephone or e-mail assistance [1]. In addition to the measures stipulated by the Government and Health Administration, every hospital and IBD unit applied changes to their clinical practice according to the characteristics of their population, the staff available at the unit and, of course, simple common sense, leading to different decisions being taken at different centers [1].
The relationship between severe acute respiratory syndrome coronavirus (SARS-CoV-2) infection and IBD seems complex and is still to be established. Gastrointestinal tract permeability may be increased in patients with IBD, with a higher expression of angiotensin-converting enzyme; this has led some authors to suggest that there is a theoretical increased risk of SARS-CoV-2 infection via the gut in IBD patients [2]. Moreover, a high proportion of patients with IBD are treated with immunosuppressive therapies, putting them at an increased risk of infections. On the other hand, the more severe presentations of COVID-19 have been related to a hyperinflammatory cytokine response and some of the most frequently used immunosuppressive therapies for immune-mediated diseases have also been used for COVID-19 [3]. In addition, in the international database of COVID-19 in patients with IBD (SECURE-IBD), corticosteroids but not anti-TNF agents were associated with adverse outcomes of the infection [4]. In fact, by August 25, 2020, only 19% of the 2156 cases reported in this registry were undergoing biological therapy at the time of COVID-19 diagnosis [5]. Therefore, we aimed to describe the clinical outcomes and the fulfilment of the treatment schedule of IBD patients treated with biological agents at our unit, as well as to report patients’ perceptions of COVID-19 and the measures adopted at our center.
Patients and Methods
Study Population
This was a cross-sectional observational study. All adult patients treated with subcutaneous or intravenous biological agents for IBD at our center were identified from the local IBD database (local ENEIDA registry [6]) and confirmed from the hospital pharmacy’s registry of biological treatments. Patients were included in the study if a biological drug was released (in the case of subcutaneous drugs) or administered (in the case of intravenous drugs) at our center, and if biological treatment was ongoing or initiated between March 1 and April 30, 2020, the two months that saw the peak of the first wave of the pandemic. Patients on biological treatment for indications other than IBD were excluded.
Characteristics of the Inflammatory Bowel Disease Unit and Changes Implemented During the Pandemic
Our center, Hospital Universitari Germans Trias i Pujol, is a university hospital located on the northern coast of the Barcelona metropolitan area with a long tradition in the management of patients with IBD. Our IBD unit is staffed by four physicians and one nurse committed the clinical care of up to 1500 patients. During the outbreak, three physicians were reassigned to inpatient COVID-19 management. During the lockdown, all elective consultations were performed by telephone, and non-elective e-mail or telephone assistance was available 7 days a week. Patients were advised to continue with their immunosuppressant medications (thiopurines, methotrexate and biological agents), remain at home whenever possible, wear masks when going outside, and to consult the IBD unit via telephone or e-mail in case of symptoms or doubts. Subcutaneous biological drugs (which were routinely released to patients at the hospital’s pharmacy monthly for adalimumab and golimumab) were released every 2 months; the day care unit was re-located in a “clean” area of the hospital, distance between seats was increased, surgical masks were supplied to patients, and a COVID-related symptoms checklist was performed by phone with every patient the day before an intravenous infusion. Intravenous infusions of biological agents were maintained at the same time frames as previously planned; the day before a planned infusion, patients received a phone call from the medical staff in order to explain all these measures, confirm the planned treatment administration, assess the clinical status of IBD, and to check for symptoms of COVID-19.
Data Collection
Demographic features and clinical and treatment data were collected from the local ENEIDA database, including the treatment schedule for the biological therapy at the beginning and at the end of the study period. The ENEIDA registry was approved by the local Ethics Committee, and patients signed an informed consent for us to collect their data in the database. Moreover, all the changes in IBD-related medications due to disease flares or clinical worsening were also recorded. Dates of administration (for intravenous drugs) or release (for subcutaneous drugs) immediately before and during the study period were collected from the pharmacy database, and the cause of delay, whether medical or intentional, in the administration/release was recorded whenever known.
Finally, all patients were invited to participate in a telephone survey (after giving their verbal consent) specifically designed to ascertain patients’ fears and perceptions regarding COVID-19, as well as the information given and the preventive measures adopted by our unit. Data are expressed as raw numbers and frequencies.
Results
Characteristics of the Study Population
A total 234 patients were included in the study of whom 117 were treated with intravenous and 117 were treated with subcutaneous biological agents. Table 1 summarizes the main demographic and clinical features of both groups. The main differences were a predominance of males and a greater proportion of Crohn’s disease and combination therapy in the intravenous therapy group.
Features and Changes of Biological Therapies and Clinical Outcomes During the Pandemic
Table 2 summarizes the main features of treatment schedules. Among the patients on intravenous therapies, a total of 139 infusions were administered during the study period: none in 11 patients, one in 79, two in 23, and three in four patients. Eighteen patients (15%) postponed at least one scheduled infusion during the pandemic (most of them at 2 to 4 weeks), six following medical advice and 12 intentionally (10%). During the pandemic, the treatment schedule was changed by the attending physician for eight patients (7%): four were dose-escalated, three optimized, and one discontinued. Additionally, biological therapy was changed in three patients.
Among the patients on subcutaneous therapies, only six patients (5%) postponed the collection of the drug at the hospital pharmacy, one following medical advice and five intentionally. During the study period, the treatment schedule was changed by the attending physician for two patients: one was dose-escalated and one was optimized. Additionally, biological therapy was changed for one patient.
Finally, five patients developed a disease flare-up (four on intravenous treatments and one on subcutaneous) and five had confirmed COVID-19 (two on intravenous treatments and three on subcutaneous), all of them of mild severity, requiring neither hospital admittance nor specific therapy.
Patients’ Perceptions During the Pandemic
A total of 77 patients who were on intravenous biological therapies and 78 who were on subcutaneous biological therapies participated in the telephone survey. Table 3 summarizes the main results of the survey. In all, 59% were actively working, 81% followed the lockdown and only 10% lived alone during the pandemic. Eleven patients (7%) reported COVID-19 in at least one family member. Thirty-eight percent consulted our unit by mail or phone call, more often patients on intravenous therapies. Forty-six per cent claimed to be familiar with the specific recommendations regarding IBD and COVID-19 made by scientific societies and the Public Health Administration. Seventeen per cent stated that they had postponed any of the administrations of biological agents during the pandemic, and this was more frequent among patients on subcutaneous therapies. The reason for postponement was fear of going to the hospital for 50% of both groups. Additionally, 7% of those who were on combination therapy acknowledged having withdrawn transiently or definitively from the thiopurine or methotrexate treatment. Among subcutaneous biological users, 60% collected the drug themselves from the hospital pharmacy.
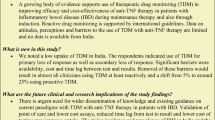
Figure 1 shows the results of the questions in which the patients were asked to score 0 to 10 (0 = completely disagree, 10 = completely agree) their perceptions on several issues. Globally their perception of the risk of becoming infected because of the disease, their therapy or due to the need to go to the hospital was heterogenous, with a wide scoring range, particularly among the group of patients treated with intravenous biologicals. However, those patients who went to the hospital during the pandemic were highly satisfied with the measures that were implemented at the hospital to increase their safety.

Patients’ perceptions on the changes implemented at the inflammatory bowel disease unit. Results are expressed on an analogical scale. Gray boxes represent the interquartile range and the black line represents the median values
Discussion
Our study specifies the proportion of patients with confirmed COVID-19 among all the users of biological therapies, together with the adherence to these therapies, in a single-center located in a pandemic red zone. The results of the present study agree with the available data suggesting that biological therapies do not increase the risk nor worsen the prognosis of COVID-19 [4, 7, 8] and supports the recommendation of continuing IBD therapies (including immunosuppressants) despite the pandemic [9]. We observed only five cases of confirmed COVID-19 (all of them of mild severity) among 234 patients (2.1%) on ongoing biological therapies, 62% of whom were on concomitant immunosuppressants. Our results are very similar to those reported for IBD patients in the Madrid area. In a study performed at a single center in Madrid during the same period, the prevalence of laboratory-confirmed COVID-19 cases among IBD patients was 1.6% among those receiving biological therapies [7]. Another recently published series from another single-center study performed in Madrid observed a cumulative incidence of confirmed COVID-19 of 3.5%, of whom only 17.8% were undergoing biological therapies [8]. Whether this low rate of confirmed infection among biological-treated IBD patients is the result of a better control of intestinal mucosal inflammation or the preventive effect of receiving anti-cytokine therapies remains unknown.
It is known that IBD patients fear contracting COVID-19, particularly those treated with immunosuppressive drugs [10, 11], a fact also stated in our survey. This may have a positive impact on a stricter fulfilment of the preventive measures but may have a negative impact on immunosuppressive treatment adherence, particularly for biological therapies, since the patients must go to the hospital for treatment administration or collection. In an anonymous Web survey performed with the support of the European Federation of Crohn’s and Ulcerative colitis associations with the participation of 3815 IBD patients from 51 countries, 4% of respondents stated they had stopped taking their IBD medication during the pandemic on their own initiative [10]. Grunert et al., in another anonymous survey performed at two German centers on 398 IBD patients, 3.8% reported having reduced their medication on their own account, 2% of whom were on biological agents [11]. The only available data from a large cohort of IBD patients on biological therapies comes from the early experience during the pandemic at a high-volume referral center in Rome (Italy) [12]. The authors reported that only 65% of patients maintained their schedules, and among those on intravenous biological therapies, 20% experienced a delay in their planned infusions, either due to the patients’ decision or for practical issues, while only 10% of patients on subcutaneous therapies were able to collect their drug. Our results showed, objectively, that 10% of patients on intravenous biologicals intentionally postponed at least one of the administrations, while among those on subcutaneous therapy, 5% postponed drug collection at the hospital pharmacy, and 22% of those who participated in the telephonic survey stated they postponed any of the planned administrations. Moreover, we observed a low rate of self-reported discontinuation of immunosuppressants among the surveyed patients who were on combination therapy. We think that these high adherence rates can be explained by the fact that all the patients on intravenous therapies received a phone call the day before infusion by a doctor from our unit (reinforcing the benefits of continuing therapy), our active advice for continuing therapies through the twitter account of the IBD unit and the rapid responses to requests for information through our institutional e-mail.
Using objective data on compliance in biological therapies (administered infusions for intravenous drugs and drug collection from the hospital pharmacy in the case of subcutaneous drugs) at a single center is one of the strengths of our study; however, it also has several limitations. Firstly, we cannot rule out that some cases of COVID-19 among our IBD population were missed because we only took into account confirmed cases of COVID-19. However, during the pandemic, diagnostic tests were performed only on those patients with moderate-to-severe symptoms and asymptomatic or mild cases of SARS-CoV-2 infection were therefore underdiagnosed. Secondly, we considered all the biologicals together, even though their different mechanism of action might have different implications on both the risk of infection and the potential deleterious or beneficial effects on infection outcomes.
In conclusion, we observed a high rate of adherence to biological therapies among IBD patients during the peak of the first wave of the pandemic, despite their fears of SARS-CoV-2 infection. Patients on active biological therapies showed a relatively low rate of confirmed COVID-19. The measures implemented at the hospital to increase patient safety were welcome and may have heightened adherence to biological therapies.
References
Martin Arranz E, Suarez Ferrer C, García Ramírez L, et al. Management of COVID-19 pandemic in Spanish inflammatory bowel disease units: results from a national survey. Inflamm Bowel Dis. 2020;26:1149–1154.
Al-Ani AH, Prentice RE, Rentsch CA, et al. Review article: prevention, diagnosis and management of COVID-19 in the IBD patient. Aliment Pharmacol Ther. 2020;52:54–72.
Zhou H, Fang Y, Xu T, Ni WJ, Shen AZ, Meng XM. Potential therapeutic targets and promising drugs for combating SARS-CoV-2. Br J Pharmacol. 2020;177:3147–3161.
Brenner EJ, Ungaro RC, Gearry RB, et al. Corticosteroids, but not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: results from an international registry. Gastroenterology. 2020;159:481.e1–491.e3.
Brenner EJ, Ungaro RC, Colombel JF, et al. SECURE-IBD Database public data update. https://covidibd.org/current-data/. Accessed August 30, 2020.
Zabana Y, Panés J, Nos P, et al. The ENEIDA registry (Nationwide study on genetic and environmental determinants of inflammatory bowel disease) by GETECCU: design, monitoring and functions. Gastroenterol Hepatol. 2020;43:551–558.
Taxonera C, Sagastagoitia I, Alba C, Mañas N, Olivares D, Rey E. 2019 novel coronavirus disease (COVID-19) in patients with inflammatory bowel diseases. Aliment Pharmacol Ther. 2020;52:276–283.
Guerra I, Algaba A, Jiménez L, et al. Incidence, clinical characteristics, and evolution of SARS-Cov-2 infection in patients with inflammatory bowel disease: a single-center study in Madrid, Spain. Inflamm Bowel Dis. 2020. https://doi.org/10.1093/ibd/izaa221.
Hanzel J, Ma C, Marshall JK, Feagan BG, Jairath V. Managing inflammatory bowel disease during COVID-19: summary of recommendations from gastrointestinal societies. Clin Gastroenterol Hepatol. 2020;18:2143–2146.
D’Amico F, Rahier JF, Leone S, Peyrin-Biroulet L, Danese S. Views of patients with inflammatory bowel disease on the COVID-19 pandemic: a global survey. Lancet Gastroenterol Hepatol. 2020;5:631–632.
Grunert PC, Reuken PA, Stallhofer J, Teich N, Stallmach A. Inflammatory bowel disease in the COVID-19 pandemic—the patients’ perspective. J Crohns Colitis. 2020. https://doi.org/10.1093/ecco-jcc/jjaa126.
Scaldaferri F, Pugliese D, Privitera G, et al. Impact of COVID-19 pandemic on the daily management of biotechnological therapy in inflammatory bowel disease patients: reorganisational response in a high-volume Italian inflammatory bowel disease centre. United Eur Gastroenterol J. 2020;8:775–781.
Acknowledgments
The authors wish to thank all the participating patients for their collaboration.
Funding
The study had no funding.
Author information
Authors and Affiliations
Contributions
ED designed the study, constructed the study database, performed statistical analyses, interpreted the results, and drafted the manuscript. II, MP, and LM collected clinical data, performed telephone surveys and critically reviewed the manuscript. MM, MC, LG and FC performed statistical analyses, interpreted the results, and critically reviewed the manuscript. GC and CQ collected pharmaceutical data and critically reviewed the manuscript. All authors approved the final version of the article.
Corresponding author
Ethics declarations
Conflict of interest
LM has served as a speaker or has received research or education funding or advisory fees from Takeda and Janssen. MC has served as a speaker or has received research or education funding or advisory fees from Takeda, Janssen, Faes Farma, and MSD; FC has served as a speaker or has received research or education funding or advisory fees from Takeda, Janssen, MSD, and Ferring. MM has served as a speaker or has received research or education funding or advisory fees from FAES, Ferring MSD, AbbVie, Takeda and Janssen; ED has served as a speaker and has received research and educational funding and advisory fees from MSD, AbbVie, Takeda, Celltrion, Samsung Bioepis, Kern Pharma, Pfizer, Janssen, Celgene, Adacyte Therapeutics, Otsuka Pharmaceuticals, Ferring, Shire Pharmaceuticals, Tillots, Thermofisher, Grifols, Gilead, Roche and Gebro. The remaining authors declared no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Iborra, I., Puig, M., Marín, L. et al. Treatment Adherence and Clinical Outcomes of Patients with Inflammatory Bowel Disease on Biological Agents During the SARS-CoV-2 Pandemic. Dig Dis Sci 66, 4191–4196 (2021). https://doi.org/10.1007/s10620-020-06807-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06807-0