
Abstract
Background/Aims
In Crohn’s disease (CD) few data are available on the usefulness of monitoring fecal calprotectin (FC) in the early postoperative setting. We assessed prospectively the accuracy of FC measured 3 months after surgery to predict the risk of endoscopic postoperative recurrence (POR) within 1 year after resection.
Methods
In 55 consecutive CD patients who had undergone ileocolonic resection samples were collected 3 months after surgery for measuring serum CRP and FC. Endoscopic POR was assessed by ileocolonoscopy within 6–12 months (median 7 months). Receiver operating characteristic (ROC) curves were generated to assess accuracy of the markers, to determine the best threshold and to calculate sensitivity, specificity, positive and negative predictive values.
Results
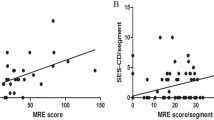
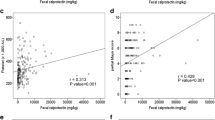
In contrast with median CRP levels, median FC concentrations measured 3 months after surgery were significantly higher in patients who later experienced endoscopic POR (Rutgeerts ≥ i2) compared with those who stayed in endoscopic remission within the following 6–12 months (205 μg/g IQR [106–721] vs. 103 μg/g IQR [60–219], p = 0.008). Area under the ROC curve for FC was 0.71. The best cutoff value of FC to identify patients in subsequent endoscopic remission 3 months after surgery was 65 μg/g (96% sensitivity, 31% specificity, 50% positive and 91% negative predictive values). In multivariate analysis, FC < 65 µg/g at 3 months was the only factor associated with subsequent endoscopic remission.
Conclusion
FC measured 3 months after surgery below 65 μg/g is an accurate marker to identify CD patients who will later stay in endoscopic remission within 1 year after resection.


Similar content being viewed by others

Abbreviations
- FC:
-
Fecal calprotectin
- hsCRP:
-
High sensitivity C-reactive protein
- CD:
-
Crohn’s disease
- ROC:
-
Receiver operating characteristic
- AUROC:
-
Area under the ROC curve
- IQR:
-
Interquartile range 25–75
- OR:
-
Odds ratio
- 95% CI:
-
95% confidence interval
References
Bouguen G, Peyrin-Biroulet L. Surgery for adult Crohn’s disease: what is the actual risk? Gut. 2011;60:1178–1181.
Buisson A, Chevaux JB, Allen PB, et al. The natural history of postoperative Crohn’s disease recurrence. Aliment Pharmacol Ther. 2012;35:625–633.
De Cruz P, Kamm MA, Hamilton AL, et al. Efficacy of thiopurines and adalimumab in preventing Crohn’s disease recurrence in high risk patients—a POCER study analysis. Aliment Pharmacol Ther. 2015;42:867–879.
De Cruz P, Kamm MA, Hamilton AM, et al. Crohn’s disease management after intestinal resection: a randomised trial. Lancet. 2015;385:1406–1417.
Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99:956–963.
Gionchetti P, Dignass A, Danese S, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: part 2: Surgical management and special situations. J Crohn’s Colitis. 2016;2017:135–149.
Buisson A, Gonzalez F, Poullenot F, et al. Comparative acceptability and perceived clinical utility of monitoring tools: a nationwide survey of patients with inflammatory bowel disease. Inflamm Bowel Dis. 2017;23:1425–1433.
Lin JF, Chen JM, Zuo JH, et al. Metaanalysis: fecal calprotectin for assessment of inflammatory bowel disease activity. Inflamm Bowel Dis. 2014;20:1407–1415.
Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and metaanalysis. Am J Gastroenterol. 2015;110:802–819.
Nancey S, Boschetti G, Moussata D, et al. Neopterin is a novel reliable fecal marker as acccurate as calprotectin for predicting endoscopic disease activity in patients with inflammatory bowel diseases. Inflamm Bowel Dis. 2013;19:1043–1052.
D’Haens G, Ferrante M, Vermeire S, et al. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatoruy bowel disease. Inflamm Bowel Dis. 2012;18:2218–2224.
Lobaton T, Lopez-Garcia A, Rodriguez-Moranta F, et al. A new rapid test for fecal calprotectin predicts endoscopic remission and postoperative recurrence in Crohn’s disease. J Crohn’s Colitis. 2013;7:641–651.
Yamamoto T, Shiraki M, Bamba T, et al. Faecal calprotectin and lactoferrin as markers for monitoring disease activity and predicting clinical recurrence in patients with Crohn’s disease after ileocolonic resection: a prospective pilot study. United Eur Gastroenterol J. 2013;1:368–374.
Lasson A, Strid H, Ohman L, et al. Fecal calprotectin one year after ileocaecal resection for Crohn’s disease—a comparison with findings at ileocolonoscopy. J Crohn’s Colitis. 2014;8:789–795.
Wright EK, Kamm MA, de Cruz P, et al. Measurement of fecal calprotectin improves monitoring and detection of recurrence of Crohn’s disease after surgery. Gastroenterology. 2015;148:938–947.
Boschetti G, Laidet M, Moussata D, et al. Levels of fecal calprotectin are associated with the severity of postoperative endoscopic recurrence in asymptomatic patients with Crohn’s disease. Am J Gastroenterol. 2015;110:865–872.
Garcia-Planella E, Manosa M, Cabré E, et al. Fecal calprotectin levels are closely correlated with the absence of relevant mucosal lesions in postoperative Crohn’s disease. Inflamm Bowel Dis. 2016;22:2879–2885.
Lopes S, Andrade P, Afonso J, et al. Correlation between calprotectin and modified Rutgeerts score. Inflamm Bowel Dis. 2016;22:2173–2181.
Schoepfer AM, Lewis JD. Serial fecal calprotectin measurements to detect endoscopic recurrence in postoperative Crohn’s disease: is colonoscopic surveillance no longer needed? Gastroenterology. 2015;148:889–892.
Qiu Y, Mao R, Chen BL, et al. Fecal calprotectin for evaluating postoperative recurrence of Crohn’s disease: a meta-analysis of prospective studies. Inflamm Bowel Dis. 2015;21:315–322.
Tham YS, Yung DE, Fay S, et al. Fecal calprotectin for detection of postoperative endoscopic recurrence in Crohn’s disease: systematic review and meta-analysis. Ther Adv Gastroenterol. 2018;11:1–12.
Lamb CA, Mohiuddin MK, Gicquel J, et al. Fecal calprotectin or lactoferrin can identify postoperative recurrence in Crohn’s disease. Br J Surg. 2009;96:663–674.
Sorrentino D, Terrosu G, Paviotti A, et al. Early diagnosis and treatment of postoperative endoscopic recurrence of Crohn’s disease: partial benefit by infliximab—a pilot study. Dig Dis Sci. 2012;57:1341–1348.
Cerrillo E, Moret I, Iborra M, et al. A nomogram combining fecal calprotectin levels and plasma cytokine profiles for individual prediction of postoperative Crohn’s disease recurrence. Inflamm Bowel Dis. 2019;25:1681–1691.
Orlando A, Modesto I, Castiglione F, et al. The role of calprotectin in predicting endoscopic post-surgical recurrence in asymptomatic Crohn’s disease: a comparison with ultrasound. European Rev Med Pharmacol Sci. 2006;10:17–22.
Boube M, Laharie D, Nancey S, et al. Variation of fecal calprotectin level within the first three months after bowel resection is predictive of endoscopic postoperative recurrence in Crohn’s disease. Dig Liver Dis 2020 (in press).
Tytgat GNJ, Mulder CJJ, Brummelkamp WH. Endoscopic lesions in Crohn’s disease early after ileocecal resection. Endoscopy. 1988;20:260–262.
Olaison G, Smedh K, Sjödahl R. Natural course of Crohn’s disease after ileocolic resection: endoscopically visualised ileal ulcers preceeding symptoms. Gut. 1992;33:331–335.
Mowatt C, Arnott I, Cahill A, et al. Mercaptopurine versus placebo to prevent recurrence of Crohn’s disease after surgical resection (TOPPIC): a multicenter, double-blind, randomized controlled trial. Lancet Gastroenterol Hepatol. 2016;1:273–282.
D’Amico F, Nancey S, Danese S, et al. A practical guide for fecal calprotectin dosage: myths and realities. J Crohns Colitis 2020 (in press).
Author information
Authors and Affiliations
Contributions
Conception and design of the study: SN, GB, MF, XR, BF. Generation, collection, assembly, analysis and/or interpretation of data: drafting or revision of the manuscript: FV, GB, CM, CC, AC, RDL, PD, EC, VK, AM, MF, XR, BF, SN. Approval of the final version of the manuscript: FV, GB, CM, CC, AC, RDL, PD, EC, VK, AM, MF, XR, BF, SN. All the authors had access to all the study data and had reviewed and approved the present final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors have declared that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Veyre, F., Boschetti, G., Meunier, C. et al. Low Levels of Fecal Calprotectin 3 Months After Surgery Predict Subsequent Endoscopic Postoperative Remission in Crohn’s Disease. Dig Dis Sci 66, 4429–4435 (2021). https://doi.org/10.1007/s10620-020-06751-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06751-z