
Abstract
Background
Postural orthostatic tachycardia syndrome (POTS) is a rare disease that is believed to be mediated by dysautonomia. Gastrointestinal complaints in POTS patients are common and disturbing but not well characterized.
Aims
We hypothesized that gastrointestinal dysmotility may be contributory to these symptoms.
Methods
We studied 12 POTS patients who presented with gastrointestinal symptoms to a tertiary referral center. Gastrointestinal symptoms were quantified using a previously validated symptom questionnaire. All patients underwent gastroduodenal manometry (GDM); select patients also underwent further testing including esophageal manometry (EM), anorectal manometry (ARM), plain abdominal radiography (AXR), abdominal computed tomography (CT), gastric emptying studies (GES), and colonic transit time (CTT) studies.
Results
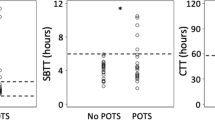
The four most common symptoms were bloating, constipation, abdominal pain, and nausea/vomiting, all experienced by greater than 70 % of patients. On GDM testing, 93 % of patients demonstrated signs of neuropathy, and the most common abnormalities observed included bursts of uncoordinated phasic activity in both fasting (59 %) and post-prandial (42 %) states, low contractility in the post-prandial state (67 %), and lack of post-prandial pattern (42 %). A total of 67 % of patients undergoing EM and 86 % of those undergoing ARM demonstrated abnormalities consistent with dysmotility. On AXR or CT, 58 % demonstrated either dilated intestinal loops or air-fluid levels. On CTT 80 % demonstrated delayed colonic transit, while on GES 60 % demonstrated delayed gastric emptying.
Conclusions
In this cohort of POTS patients with gastrointestinal symptoms, there is a high prevalence of abnormal manometric and radiographic findings suggestive of dysmotility.

Similar content being viewed by others


References
Robertson D. The epidemic of orthostatic tachycardia and orthostatic intolerance. Am J Med Sci. 1999;317:75–77.
Stewart JM. Pooling in chronic orthostatic intolerance: arterial vasoconstrictive but not venous compliance defects. Circulation. 2002;105:2274–2281.
Sandroni P, Opfer-Gehrking TL, McPhee BR, Low PA. Postural tachycardia syndrome: clinical features and follow-up study. Mayo Clin Proc. 1999;74:1106–1110. doi:10.4065/74.11.1106.
Thieben MJ, Sandroni P, Sletten DM, et al. Postural orthostatic tachycardia syndrome: the Mayo clinic experience. Mayo Clin Proc. 2007;82:308–313. doi:10.4065/82.3.308.
Triadafilopoulos G, Sharma R. Features of symptomatic gastroesophageal reflux disease in elderly patients. Am J Gastroenterol. 1997;92:2007–2011.
Gerson LB, Edson R, Lavori PW, Triadafilopoulos G. Use of a simple symptom questionnaire to predict Barrett’s esophagus in patients with symptoms of gastroesophageal reflux. Am J Gastroenterol. 2001;96:2005–2012. doi:10.1111/j.1572-0241.2001.03933.x.
Thumshirn M, Bruninga K, Camilleri M. Simplifying the evaluation of postprandial antral motor function in patients with suspected gastroparesis. Am J Gastroenterol. 1997;92:1496–1500.
Schuffler MD, Rohrmann CA, Chaffee RG, Brand DL, Delaney JH, Young JH. Chronic intestinal pseudo-obstruction. A report of 27 cases and review of the literature. Medicine. 1981;60:173–196.
Stanghellini V, Camilleri M, Malagelada JR. Chronic idiopathic intestinal pseudo-obstruction: clinical and intestinal manometric findings. Gut. 1987;28:5–12.
Frank JW, Sarr MG, Camilleri M. Use of gastroduodenal manometry to differentiate mechanical and functional intestinal obstruction: an analysis of clinical outcome. Am J Gastroenterol. 1994;89:339–344.
Rosa ESL, Gerson L, Davila M, Triadafilopoulos G. Clinical, radiologic, and manometric characteristics of chronic intestinal dysmotility: the Stanford experience. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2006;4:866–873. doi:10.1016/j.cgh.2006.05.001.
Quigley EM, Deprez PH, Hellstrom P, et al. Ambulatory intestinal manometry: a consensus report on its clinical role. Dig Dis Sci. 1997;42:2395–2400.
Rao SS, Azpiroz F, Diamant N, Enck P, Tougas G, Wald A. Minimum standards of anorectal manometry. Neurogastroenterol Motil Off J Eur Gastrointest Motil Soc. 2002;14:553–559.
Rao SS, Mudipalli RS, Stessman M, Zimmerman B. Investigation of the utility of colorectal function tests and Rome II criteria in dyssynergic defecation (Anismus). Neurogastroenterology and motility: the Official Journal of the European Gastrointestinal Motility Society. 2004;16:589–596. doi:10.1111/j.1365-2982.2004.00526.x.
Summers RW, Anuras S, Green J. Jejunal manometry patterns in health, partial intestinal obstruction, and pseudoobstruction. Gastroenterology. 1983;85:1290–1300.
Stanghellini V, Corinaldesi R, Ghidini C, et al. Reversibility of gastrointestinal motor abnormalities in chronic intestinal pseudo-obstruction. Hepatogastroenterology. 1992;39:34–38.
Schuffler MD, Pope CE 2nd. Studies of idiopathic intestinal pseudoobstruction. II. Hereditary hollow visceral myopathy: family studies. Gastroenterology. 1977;73:339–344.
Tobon F, Reid NC, Talbert JL, Schuster MM. Nonsurgical test for the diagnosis of Hirschsprung’s disease. N Engl J Med. 1968;278:188–193. doi:10.1056/NEJM196801252780404.
Zhang HY, Feng JX, Huang L, Wang G, Wei MF, Weng YZ. Diagnosis and surgical treatment of isolated hypoganglionosis. World J Pediatr. 2008;4:295–300. doi:10.1007/s12519-008-0053-3.
Burnstock G. Purinergic nerves. Pharmacol Rev. 1972;24:509–581.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huang, R.J., Chun, C.L., Friday, K. et al. Manometric Abnormalities in the Postural Orthostatic Tachycardia Syndrome: A Case Series. Dig Dis Sci 58, 3207–3211 (2013). https://doi.org/10.1007/s10620-013-2865-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-013-2865-9