
Abstract
Aim
Our purpose was to review the clinical and imaging findings in a series of patients with septic thrombophlebitis of the portal venous system in order to define criteria that might allow more confident and timely diagnosis.
Materials and Methods
This is a retrospective case series. The clinical and imaging features were analyzed in 33 subjects with septic thrombophlebitis of the portal venous system.
Results
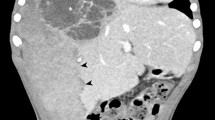
All 33 patients with septic thrombophlebitis of the portal venous system had pre-disposing infectious or inflammatory processes. Contrast-enhanced CT studies of patients with septic thrombophlebitis typically demonstrate an infectious gastrointestinal source (82%), thrombosis (70%), and/or gas (21%) of the portal system or its branches, and intrahepatic abnormalities such as a transient hepatic attenuation difference (THAD) (42%) or abscess (61%).
Conclusions
Septic thrombophlebitis of the portal system is often associated with an infectious source in the gastrointestinal tract and sepsis. Contrast-enhanced CT demonstrates an infectious gastrointestinal source, thrombosis or gas within the portal system or its branches, and intrahepatic abnormalities such as abscess in most cases. We report a THAD in several of our patients, an observation that was not made in prior reports of septic thrombophlebitis.





Similar content being viewed by others


References
Bradbury MS, et al. Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. 2002;22:527–541.
Balthazar EJ, Gollapudi P. Septic thrombophlebitis of the mesenteric and portal veins: CT imaging. J Comput Assist Tomogr. 2000;24:755–760.
Lee HK, et al. Portal vein thrombosis: CT features. Abdom Imaging. 2008;33:72–79.
Slovis TL, et al. Complicated appendiceal inflammatory disease in children: pylephlebitis and liver abscess. Radiology. 1989;171:823–825.
Plemmons RM, Dooley DP, Longfield RN. Septic thrombophlebitis of the portal vein (pylephlebitis): diagnosis and management in the modern era. Clin Infect Dis. 1995;21:1114–1120.
Witte CL, et al. Protean manifestations of pylethrombosis. A review of thirty-four patients. Ann Surg. 1985;202:191–202.
Mathieu D, Vasile N, Grenier P. Portal thrombosis: dynamic CT features and course. Radiology. 1985;154:737–741.
Itai Y, Moss AA, Goldberg HI. Transient hepatic attenuation difference of lobar or segmental distribution detected by dynamic computed tomography. Radiology. 1982;144:835–839.
Lim GM, et al. Septic thrombosis of the portal vein: CT and clinical observations. J Comput Assist Tomogr. 1989;13:656–658.
Graham GA, Bernstein RB, Gronner AT. Gas in the portal and inferior mesenteric veins caused by diverticulitis of the sigmoid colon. Report of a case with survival. Radiology. 1975;114:601–602.
Tublin ME, Dodd GD 3rd, Baron RL. Benign and malignant portal vein thrombosis: differentiation by CT characteristics. AJR Am J Roentgenol. 1997;168:719–723.
Harbin WP, Robert NJ, Ferrucci JT Jr. Diagnosis of cirrhosis based on regional changes in hepatic morphology: a radiological and pathological analysis. Radiology. 1980;135:273–283.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ames, J.T., Federle, M.P. Septic Thrombophlebitis of the Portal Venous System: Clinical and Imaging Findings in Thirty-Three Patients. Dig Dis Sci 56, 2179–2184 (2011). https://doi.org/10.1007/s10620-010-1533-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1533-6